Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About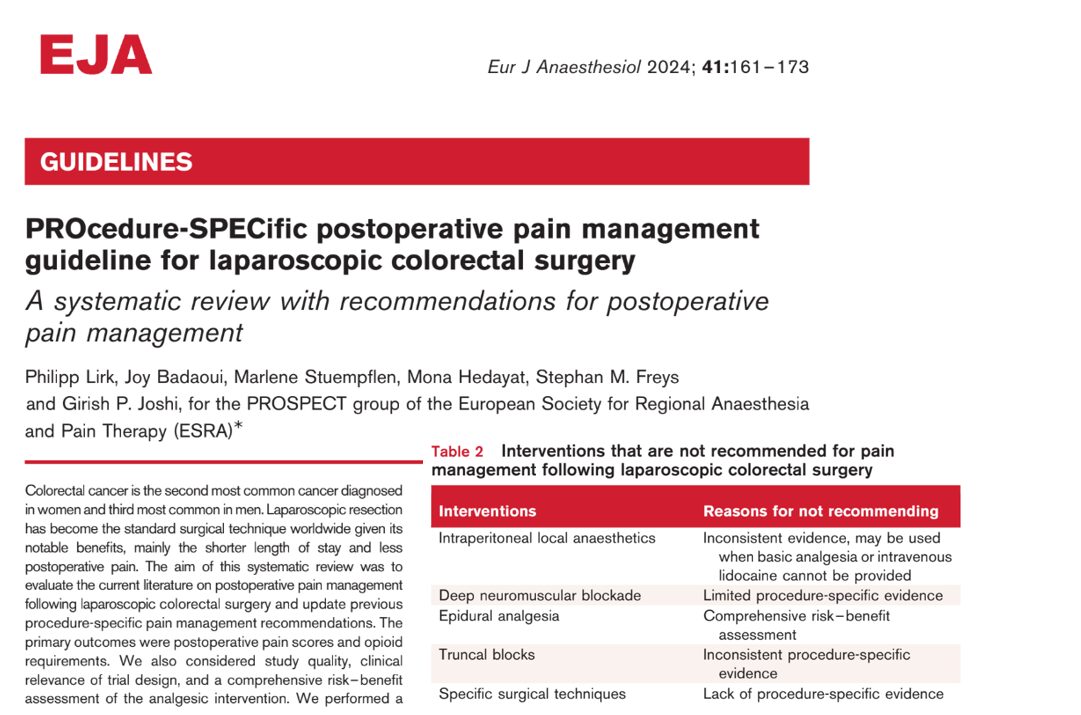




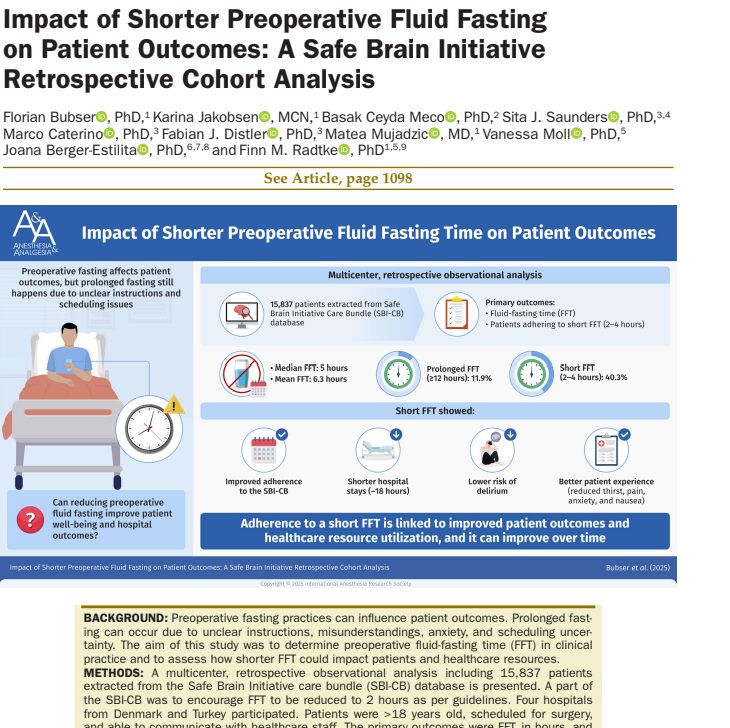
Laparoscopic colorectal surgery is the standard treatment for colorectal cancer, the second most common cancer in women and the third most common in men. The minimally invasive nature of this procedure results in shorter hospital stays and less postoperative pain. The PROSPECT Working Group has conducted a comprehensive systematic review of current literature to update evidence-based recommendations for postoperative pain management specific to laparoscopic colorectal surgery.
Recommended interventions
- Basic analgesia:
- Paracetamol (Acetaminophen): Standard for both rectal and colonic surgeries.
- Nonsteroidal Anti-inflammatory Drugs (NSAIDs) or COX-2 Inhibitors: For colonic surgery (but not rectal surgery due to potential risk of anastomotic leakage).
- Surgical port site wound infiltration: Simple and cost-effective method for managing localized pain.
- Rescue opioids: For breakthrough pain, used cautiously to minimize side effects and dependency.
Interventions with no consensus
Intravenous lidocaine:
- May be considered when basic analgesia cannot be provided.
- Evidence on its effectiveness is inconsistent, with some studies reporting analgesic and opioid-sparing effects and others showing no benefit.
Intrathecal morphine:
- Provides effective pain relief but may cause side effects such as pruritus, respiratory depression, and urinary retention.
- Not routinely recommended due to its invasive nature and potential side effects.
Not recommended interventions
- Intraperitoneal Local Anaesthetics (IPLA): Inconsistent evidence of effectiveness.
- Deep neuromuscular blockade: Limited evidence of benefit for pain relief.
- Epidural analgesia: Invasive, with minimal benefits compared to less invasive alternatives.
- Truncal nerve blocks (e.g., TAP, QLB, ESPB): Inconsistent evidence and potential risks of local anaesthetic toxicity.
- Specific surgical techniques: No clear evidence that variations in surgical techniques significantly impact postoperative pain.
Why NSAIDs are not recommended for rectal surgery
While NSAIDs and COX-2 inhibitors are effective in reducing postoperative pain, their use in rectal surgery is discouraged due to the potential risk of anastomotic leakage. This complication can lead to serious postoperative morbidity, outweighing the analgesic benefits of these medications.
Managing postoperative pain: Step-by-step
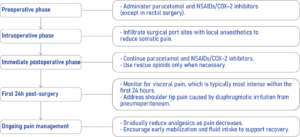
Conclusion
Effective postoperative pain management after laparoscopic colorectal surgery involves a combination of paracetamol, NSAIDs/COX-2 inhibitors (for colonic surgery), and surgical port site wound infiltration, with rescue opioids used as needed. While intravenous lidocaine and intrathecal morphine may provide additional pain relief, their use is not routinely recommended due to inconsistent evidence and potential side effects. These evidence-based guidelines aim to optimize pain control, reduce opioid consumption, and enhance patient recovery following surgery.
For more detailed information, refer to the full guidelines published in the European Journal of Anaesthesiology, 2024.Reference: Lirk P et al. PROcedure-SPECific postoperative pain management guideline for laparoscopic colorectal surgery: A systematic review with recommendations for postoperative pain management. Eur J Anaesthesiol. 2024;4:161-173
Read about this topic and more on NYSORA’s Anesthesia Assistant App. Don’t miss out—download now.