Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About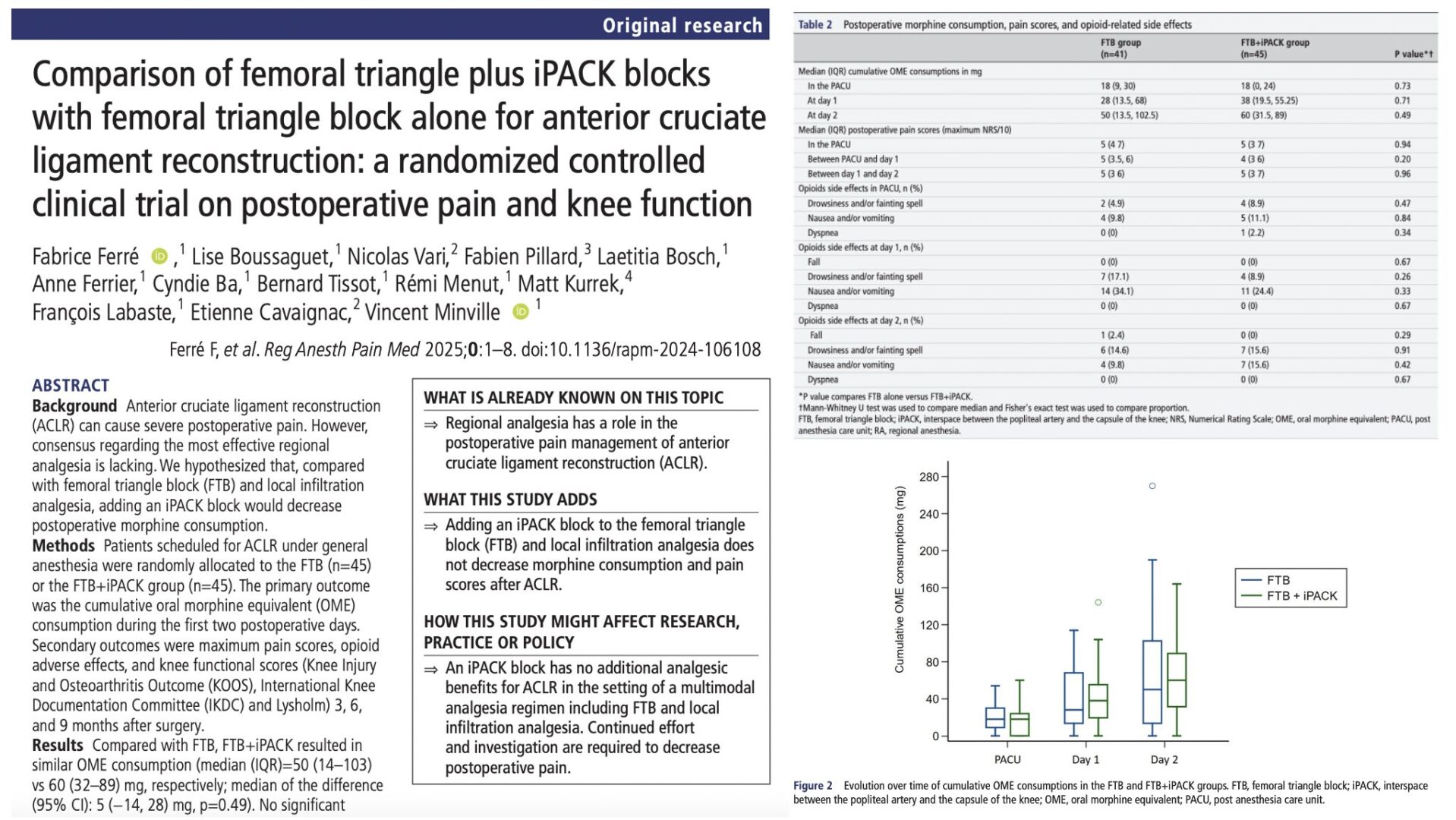




Anterior cruciate ligament reconstruction (ACLR) is a frequent orthopedic procedure, particularly among young, active individuals and athletes. Despite advances in surgical technique and perioperative care, managing postoperative pain remains a critical component of ensuring early mobilization, optimal rehabilitation, and high patient satisfaction. Inadequate pain control can delay recovery, prolong opioid use, and hinder long-term functional outcomes
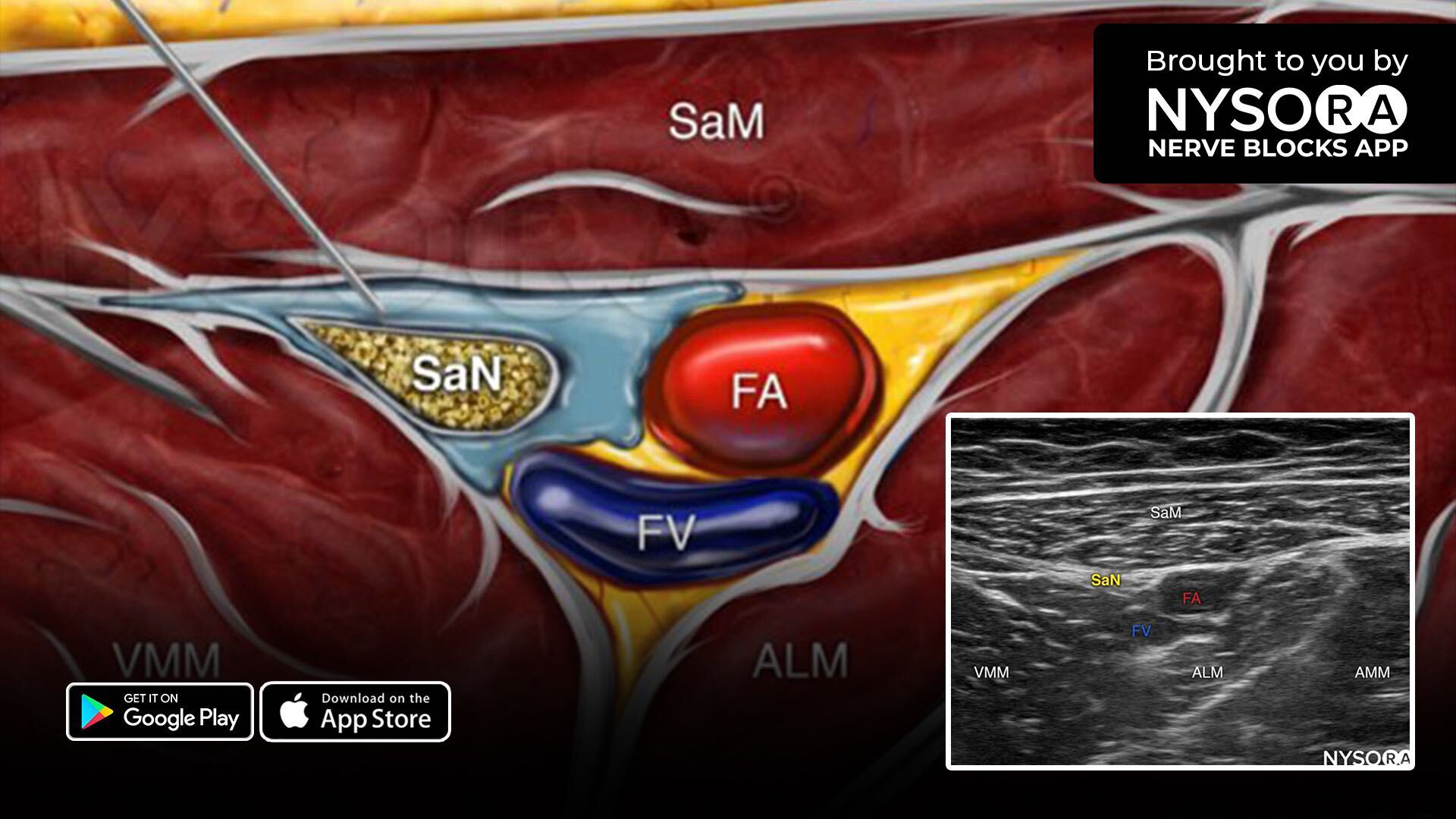
Over the years, regional anesthesia has emerged as an important adjunct in multimodal analgesic strategies for ACLR. Among these, the femoral triangle block (FTB), a variant of the adductor canal block, has become increasingly popular for its ability to provide anterior knee analgesia with minimal motor impairment. However, posterior knee pain remains a challenging area, often inadequately addressed by FTB alone.
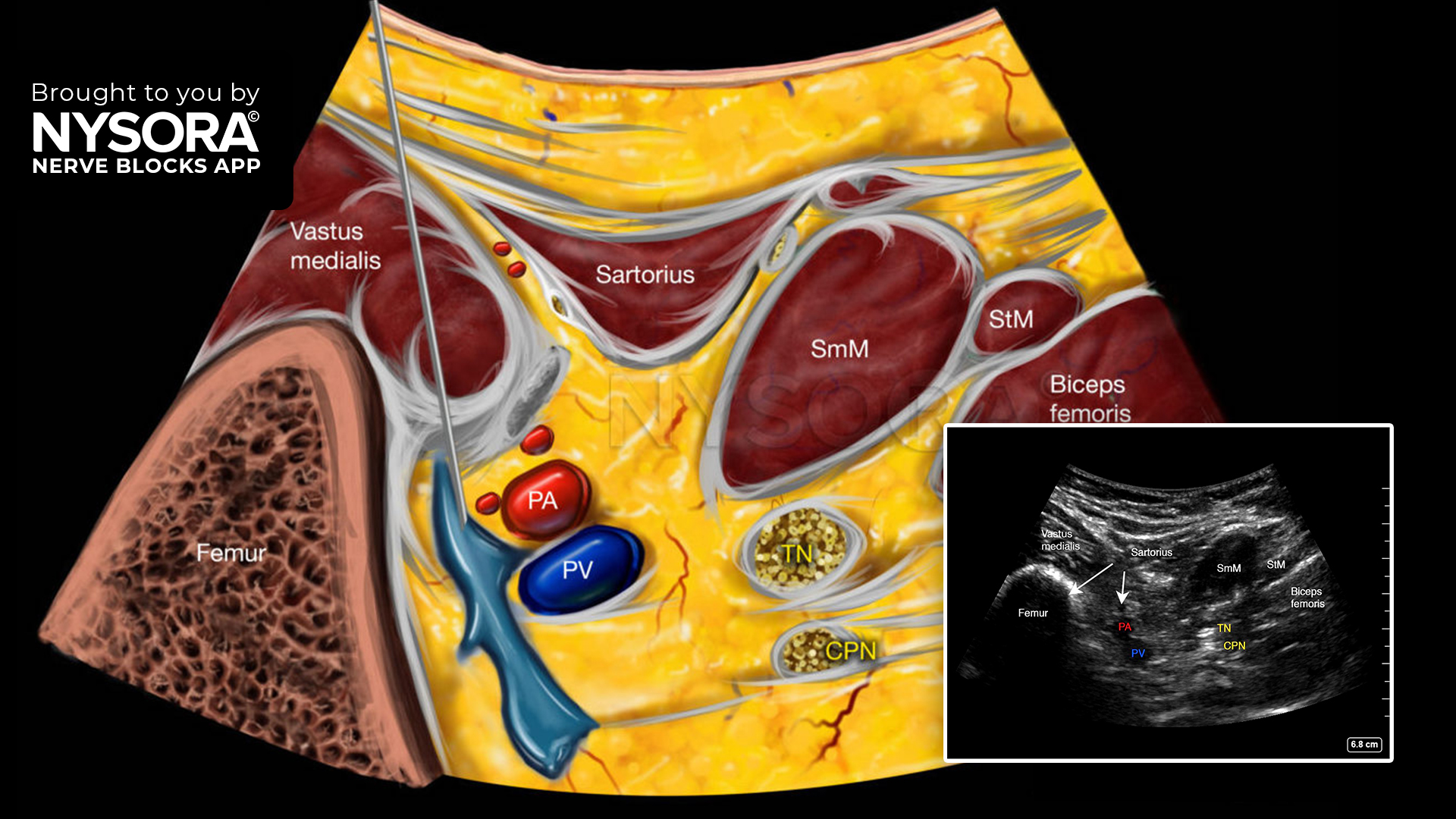
The interspace between the popliteal artery and the capsule of the posterior knee (iPACK) block was developed to target sensory nerves innervating the posterior capsule without affecting the tibial or peroneal nerves, thus preserving motor function. The iPACK has shown promising results in total knee arthroplasty (TKA), but its role in ACLR is still being defined.
This randomized controlled trial evaluated whether adding an iPACK block to a standard analgesic regimen, including FTB and local infiltration, provides superior pain control and functional outcomes after ACLR
Study objective and methods
The study aimed to determine if the addition of an iPACK block to FTB reduces opioid consumption and improves pain scores and functional outcomes following ACLR.
- Design: Single-blind, randomized controlled trial conducted at a French academic hospital.
- Participants: 90 adult patients undergoing primary ACLR under general anesthesia.
- FTB group: Received ultrasound-guided FTB with 15 mL of 0.2% ropivacaine.
- FTB + iPACK group: Received the same FTB plus an iPACK block (25 mL of 0.2% ropivacaine) targeting the posterior knee capsule.
- Common to both groups: Surgical infiltration analgesia with 20 mL of ropivacaine, single-shot spinal anesthesia with intrathecal morphine, and multimodal postoperative analgesia including paracetamol, NSAIDs, and oral opioids as needed.
- Primary outcome: Cumulative oral morphine equivalent (OME) consumption in the first 48 hours postoperatively.
- Secondary outcomes: Pain scores (NRS 0–10), opioid-related side effects, and knee function (measured using KOOS, IKDC, and Lysholm scores) at 3, 6, and 9 months.
Key findings
- Opioid consumption: There was no statistically significant difference in cumulative opioid use between the two groups during the first 48 hours after surgery. Patients in the FTB group consumed a median of 50 mg OME, while those in the FTB + iPACK group consumed a median of 60 mg (p = 0.49).
- Pain scores: Pain intensity was similar between groups across all time points. In the PACU, both groups reported a median NRS of 5. On postoperative days 1 and 2, pain scores remained comparable, with no significant differences observed.
- Side effects: The incidence of opioid-related adverse events, such as nausea, sedation, and falls, did not differ significantly between groups.
- Knee function: Functional scores (KOOS, IKDC, Lysholm) at 3, 6, and 9 months were comparable between groups. However, across both groups, patients with lower OME consumption (< 50 mg) in the first 48 hours had slightly higher functional scores, though differences did not reach clinical significance.
Conclusion
The addition of an iPACK block to femoral triangle block and local infiltration analgesia did not provide additional analgesic or functional benefits in patients undergoing ACLR. Pain control was already effective with the standard multimodal regimen, making it difficult to demonstrate added value from iPACK in this setting. Both approaches preserved motor function and supported good postoperative recovery.
Future research
Further studies should explore personalized analgesic strategies targeting patients at higher risk of severe postoperative pain. Trials designed to optimize block combinations or target specific pain sources, such as graft harvest sites, may reveal more meaningful benefits. Additionally, efforts to correlate acute pain control with long-term knee function in larger cohorts could help identify predictors of successful recovery. Finally, studies should assess objective success rates of iPACK using imaging or sensory mapping to better understand its role in ACLR analgesia.
For more detailed information, refer to the full article in RAPM.
Ferré F et al. Comparison of femoral triangle plus iPACK blocks with femoral triangle block alone for anterior cruciate ligament reconstruction: a randomized controlled clinical trial on postoperative pain and knee function. Reg Anesth Pain Med. Published online March 7, 2025.
Download the Nerve Blocks App HERE for in-depth insights on the femoral triangle and iPACK blocks. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Manual Course on NYSORA’s LMS!