Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Types of breech presentation
- Management of breech presentation
Definition and mechanisms
- Breech presentation refers to the fetus in the longitudinal lie with the buttocks or lower extremity entering the pelvis first
- Three types:
- Frank breech: fetus has flexion of both hips, and the legs are straight with the feet near the fetal face, in a pike position
- Complete breech: fetus sits with flexion of both hips and both legs in a tuck position
- Incomplete breech: can have any combination of one or both hips extended, also known as footling (one leg extended) breech, or double footling breech (both legs extended)
- Occurs in 3-4% of all term pregnancies
- A higher percentage of breech presentations occurs with less advanced gestational age
- At 32 weeks, 7% of fetuses are breech
- At 28 weeks or less, 25% are breech
- Clinical conditions associated with a breech presentation include those that may increase or decrease fetal motility, or affect the vertical polarity of the uterine cavity
- It is unsafe for a breech baby to be born vaginally due to the risk of injury (dislocated or broken bones) or umbilical cord problems (flattening or twisting)
- Turning the baby into the head-first position and/or a planned C-section are the safest option
Etiology
- Prematurity
- Multiple gestations
- Aneuploidies
- Congenital anomalies: fetal sacrococcygeal teratoma, fetal thyroid goiter
- Mullerian anomalies
- Uterine leiomyoma
- Placental polarity as in placenta previa
- Polyhydramnios
- Oligohydramnios
- Previous history of breech presentation (recurrence rate is 10% for the second pregnancy and 27% in the third pregnancy)
Evaluation
- Physical exam: palpation of a hard, round, mobile structure at the fundus and the inability to palpate a presenting part in the lower abdomen superior to the pubic bone or the engaged breach in the same area, should raise suspicion of a breech presentation
- Cervical exam: the lack of a palpable presenting part, palpation of a lower extremity, usually a foot, or for the engaged breech, palpation of the soft tissue of the fetal buttocks may be noted
- Note that the soft tissue of the fetal buttocks may be interpreted as caput of the fetal vertex if the patient has been laboring
- Ultrasound confirms the diagnosis
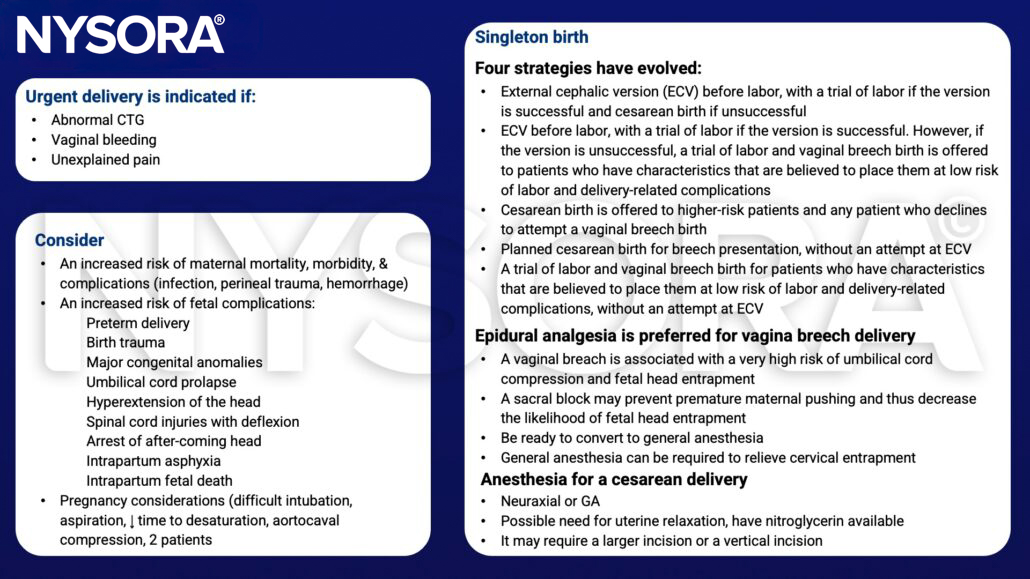
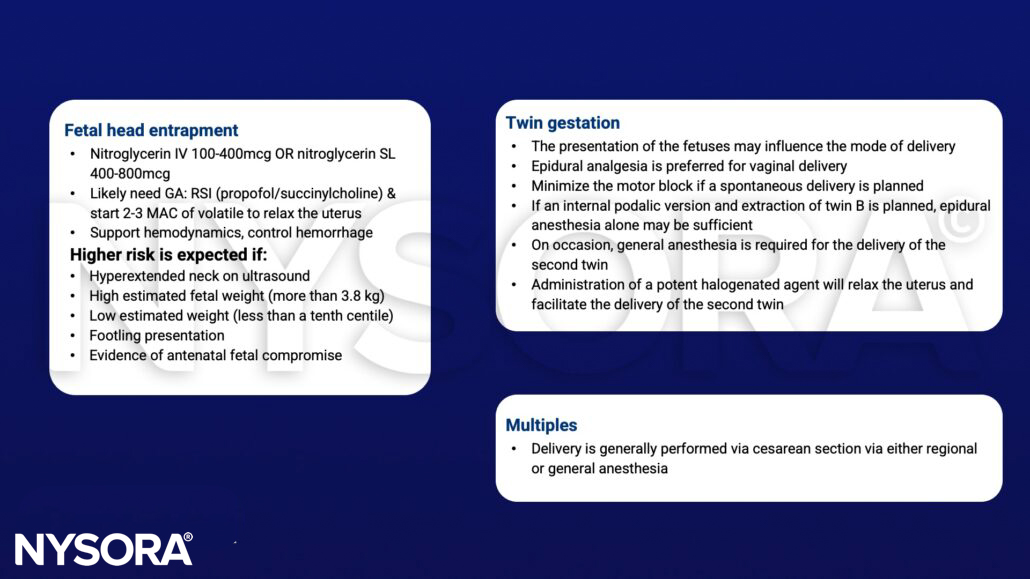
Management
Suggested reading
- Gray CJ, Shanahan MM. 2022. Breech presentation. StatPearls.
- Hofmeyer GD. 2022. Overview of breech presentation. Up to date.
- 2017. Management of Breech Presentation. BJOG: An International Journal of Obstetrics & Gynaecology 124, e151–e177.
- Stitely ML, Gherman RB. Labor with abnormal presentation and position. Obstet Gynecol Clin North Am. 2005;32(2):165-179.
- Pratt SD. Anesthesia for breech presentation and multiple gestation. Clin Obstet Gynecol. 2003;46(3):711-729.
- Pollack KL, Chestnut DH. 1990. Anesthesia for complicated vaginal deliveries. Anesthesiology clinics of North America. 8;1:115-129.