Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Define umbilical cord prolapse
- Describe the risk factors for developing umbilical cord prolapse
- Umbilical cord prolapse management
Definition and mechanisms
- Umbilical cord prolapse is an obstetric emergency in which the umbilical cord descends through the cervix alongside (occult) or past (overt) the fetal presenting part
- It can occur before or during the delivery of the baby, usually close to the end of pregnancy (after 37 weeks)
- Compression of, or vasospasm of, the umbilical cord impairs the blood flow between the placenta and fetus, leading to fetal hypoxia and bradycardia
- Fetal hypoxia may result in fetal death or permanent disability if not rapidly diagnosed and managed
- Early recognition and intervention are important to reduce the adverse outcomes in the fetus
Classification
- Overt prolapse: Cord exits the cervix before the fetal presenting part
- Occult prolapse: Cord exits the cervix with the fetal presenting part
Complications
- Surviving infants may develop complications secondary to asphyxia (i.e., neonatal encephalopathy and cerebral palsy)
- Stillbirth
Risk factors
- Maternal age ≥35 years
- Premature rupture of membranes
- Preterm delivery
- Low birth weight
- Multiple gestation pregnancies
- Placenta praevia
- Polyhydramnios
- Fetal malpresentation (i.e., breech presentation)
- External cephalic version procedure
- Intrauterine growth restriction
- Fetal and cord abnormalities
Diagnosis
- Fetal bradycardia (<120 bpm) in the setting of ruptured membranes should prompt immediate evaluation for potential cord prolapse
- Umbilical cord prolapse is diagnosed by seeing or palpating the prolapsed cord on pelvic examination
| Overt prolapse | Occult prolapse |
|---|---|
| Diagnosis is clinical and made by palpation of a pulsating structure in the vaginal vault or visibly protruding from the vaginal introitus Typically accompanied by fetal bradycardia or severe variable decelerations | Only fetal bradycardia may appear The cord is not visible or palpable ahead of the fetal presenting part |
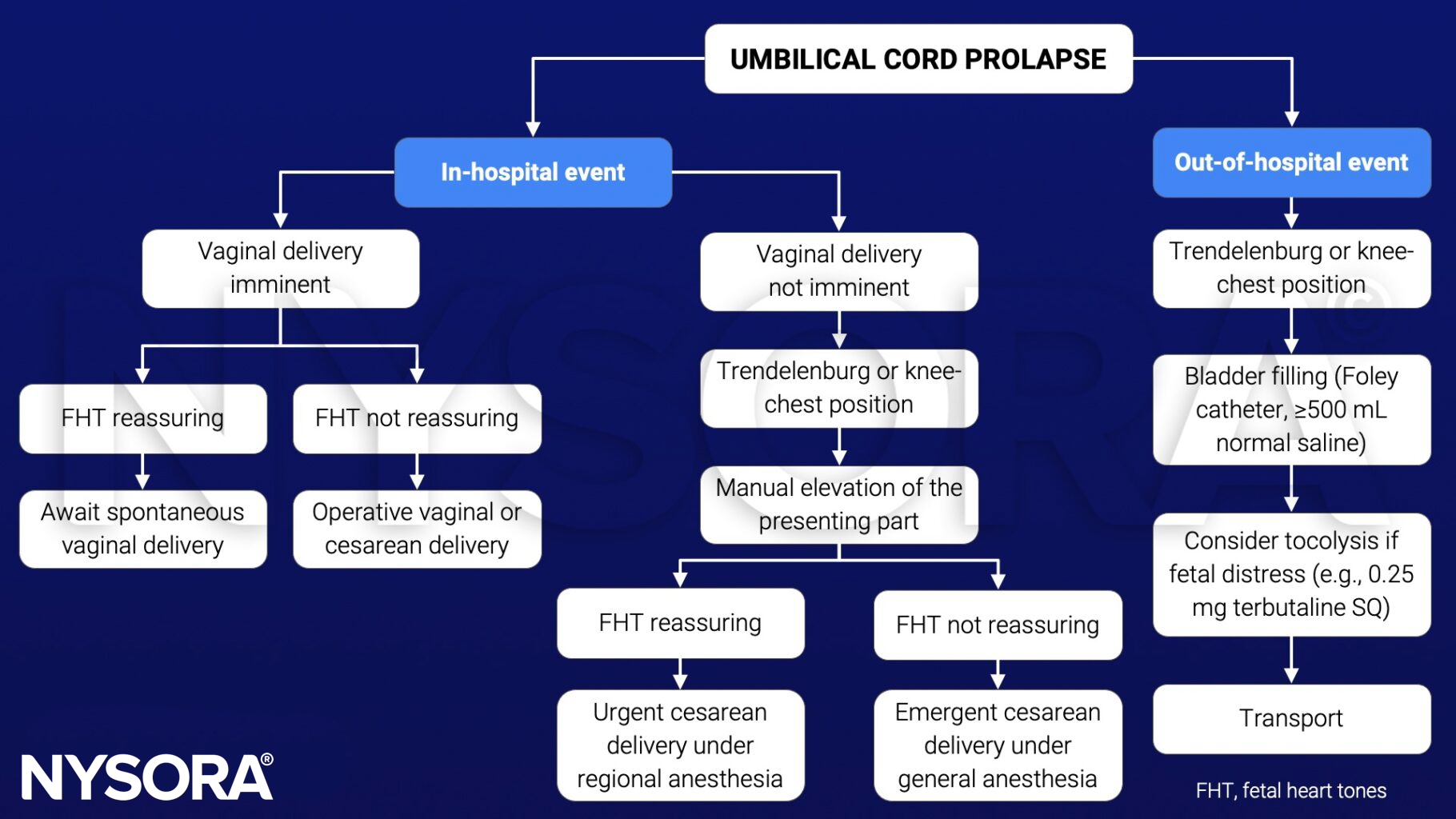
Management
Goal: Avoid cord compression and vasospasm
- Call for help
- Establish an intravenous line (if not already placed)
- Ensure continuous fetal monitoring
- Administer oxygen via a face mask (if needed)
- Administer aspiration prophylaxis
- Umbilical cord prolapse is an acute obstetric emergency requiring immediate delivery of the baby, usually via cesarean section
- Allow instrumental/vaginal delivery if considered quicker
- Inform the anesthesiologist, pediatrician, and OR staff
- Patient consent
- Funic decompression: Elevating the fetal presenting part to aid cord decompression
- Two fingers/hand in the vagina – manual elevation of the presenting part
- Steep Trendelenburg or knee-chest position, lying on the left side is preferred
- Bladder filling with a Foley catheter (≥500 mL of normal saline)
- Funic reduction (rarely used): Replacement of the umbilical cord into the uterus
- Tocolysis in case of fetal distress or if prolonged interval to delivery is expected
- Keep the cord warm and moist if it is protruding from the vagina and delivery is not imminent
- Avoid aortocaval compression
- Minimize handling of the cord outside of the vagina to prevent vasospasm
See also cesarean section considerations
Suggested reading
- Boushra M, Stone A, Rathbun KM. Umbilical Cord Prolapse. [Updated 2022 Jun 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK542241/
- Sayed Ahmed WA, Hamdy MA. Optimal management of umbilical cord prolapse. Int J Womens Health. 2018;10:459-465.
Clinical updates
Galvan et al. (2024, BJA Education) emphasize that umbilical cord prolapse remains a time-critical obstetric emergency, with fetal heart rate abnormalities present in up to 60% of cases, requiring simultaneous cord decompression maneuvers and preparation for urgent delivery. The review reinforces that cesarean section is the preferred mode of delivery unless vaginal birth is immediately imminent, and highlights the anesthetist’s key role in early risk stratification, neuraxial readiness, and rapid escalation to general anesthesia to achieve optimal decision-to-delivery intervals.