Learning objectives
- Describe the indications and risks for cervical cerclage
- Manage patients presenting for cervical cerclage
Background
- Cervical cerclage is performed as an attempt to prolong pregnancy in women who are at high risk of preterm delivery due to cervical insufficiency
- Suturing of the cervix to prevent rupture of fetal membranes
Risk factors for cervical insufficiency
- Prior cervical procedures or trauma:
- Loop electrode excisional procedure
- Cone biopsy
- Prior cervical lacerations
- Repetitive cervical dilation and/or pregnancy terminations
- Maternal connective tissue diseases or abnormalities
- Congenital Mullerian anomalies
- Maternal exposure in utero to diethylstilbestrol
Indications
- History-indicated: One or more second-trimester pregnancy losses related to painless cervical dilation and in the absence of labor or abruptio placentae, or prior cerclage placed due to cervical insufficiency in the second trimester
- Ultrasound-indicated: History of spontaneous loss or preterm birth at less than 34 weeks if the cervical length in a current singleton pregnancy is less than 25 mm before 24 weeks of gestation
- Rescue cerclage: Singleton pregnancy at less than 24 weeks with advanced cervical dilation in the absence of contractions, intraamniotic infection, or placental abruption
- Not recommended in pregnancies of multiple gestations
Technique
- Transvaginal
- McDonald method: Simple purse-string suture at the cervicovaginal junction
- Shirodkar method: Suturing anterior-posterior and posterior-anterior after an incision of the mucosa of the anterior cervix, with the aid of an Allis clamp
- Transabdominal
- Remove sutures between weeks 36-38 in women anticipating vaginal delivery:
- McDonald cerclage requires no anesthesia
- Shirodkar requires anesthesia (spinal, epidural)
- Highly epithelialized sutures may require Cesarean section
Risks
- Rupture of fetal membranes
- Infection or sepsis
- Lacerations at the surgical site
- Anesthesia-related complications
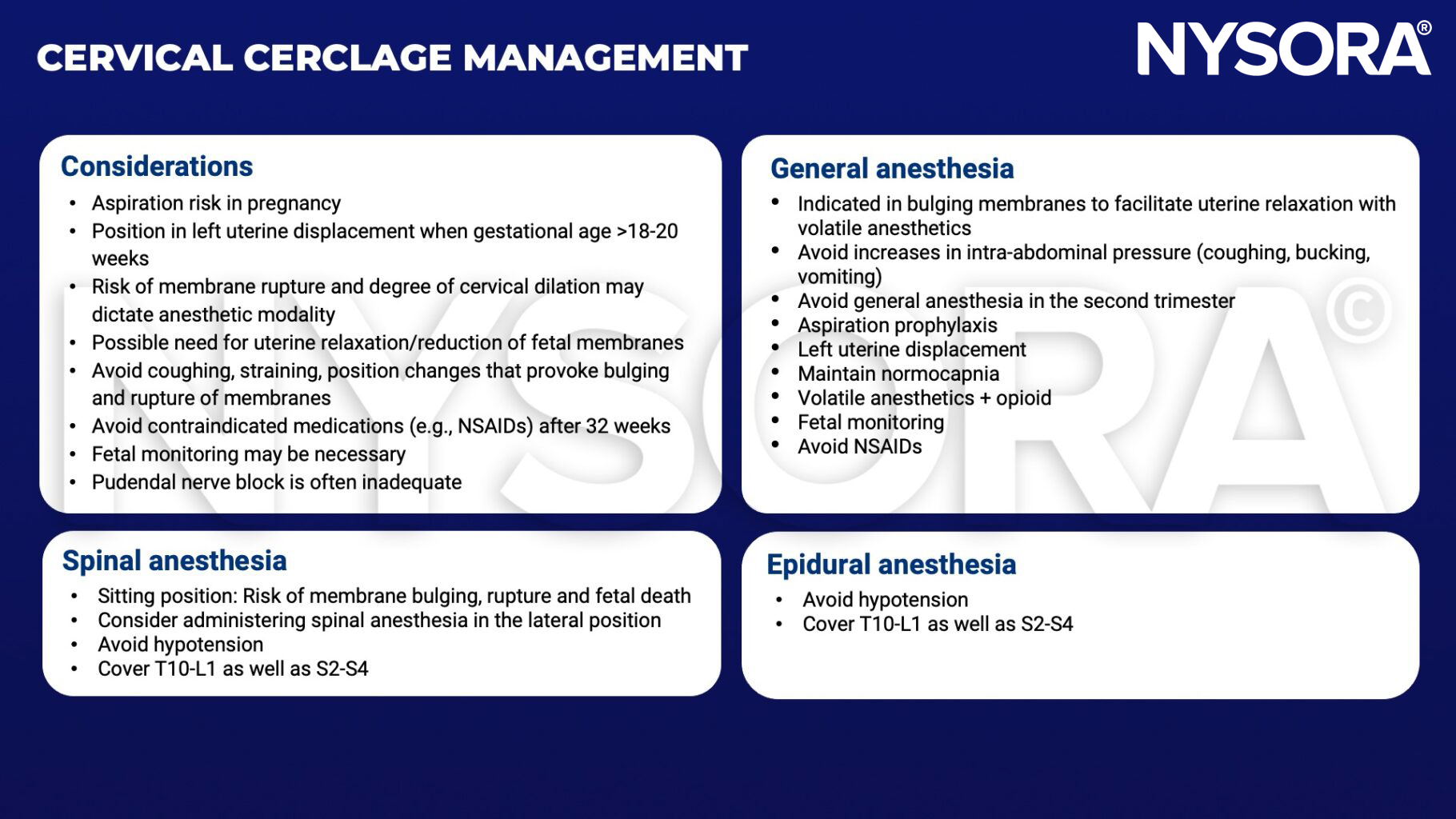
Management
Suggested reading
- Bieber KB, Olson SM. Cervical Cerclage. [Updated 2022 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560523/
- Shennan, A, Story, L, Jacobsson, B, Grobman, WA; the FIGO Working Group for Preterm Birth. FIGO good practice recommendations on cervical cerclage for prevention of preterm birth. Int J Gynecol Obstet. 2021; 155: 19– 22.