
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Recognize the signs and symptoms of strabismus
- Describe the risk factors of strabismus
- Anesthetic management for patients undergoing strabismus surgery
Definition and mechanisms
- Strabismus surgery is surgery of the extraocular muscles (tightening, lengthening, transposing, or shortening the eye muscles) to correct strabismus, the misalignment of the eyes
- It is the most common ophthalmic surgery in pediatric patients
- Strabismus occurs in 3-5% of children worldwide
- Strabismus results from an imbalance in extraocular muscle function → two different images (one from each eye) are transmitted to the brain, resulting in loss of visual depth → in children, the brain may suppress the image from the weaker eye, impairing visual development and leading to amblyopia (decreased vision in a normal healthy eye; lazy eye)
- The prognosis is good if the correction is performed as early as possible (before the child reaches the age of 8 years)
Signs and symptoms
- Strabismus may involve one or both eyes
- The affected eye can deviate outward (exotropia), inward (esotropia), upward (hypertropia), or downward (hypotropia)
- The deviation may be intermittent or constant, large magnitude (large angle) or small magnitude (small angle)
- Diplopia (double vision)
- Loss of stereopsis
- Headache
- Inability to read comfortably
- Fatigue when reading
- Amblyopia (loss of visual acuity)
- Psychosocial issues (interferes with normal eye contact with others)
Risk factors
- Premature birth
- Low birth weight
- Smoking during pregnancy
- Family history
- Down syndrome (29%)
- Cerebral palsy (53%)
- Syndromes with craniofacial dysostosis (up to 90%)
Patient characteristics
- Infantile strabismus needs early surgery (6-12 months) for the best visual outcome
- Rare association with primary muscle diseases and malignant hyperthermia
- Associated syndromes: Apert syndrome, Cri du chat syndrome, Crouzon syndrome, Down syndrome, Goldenhar syndrome, Marfan syndrome, Moebius syndrome, Stickler syndrome, Turner syndrome
Problems
- Airway not accessible because of the microscope’s position
- Avoid suxamethonium
- Can trigger malignant hyperthermia in susceptible patients
- Can cause tonic contracture of extraocular muscles, interferes with forced duction test
- Oculocardiac reflex
- Topical adrenaline is often used to reduce bleeding and may be absorbed systemically, watch dose in small children
- High incidence of postoperative nausea and vomiting (PONV)
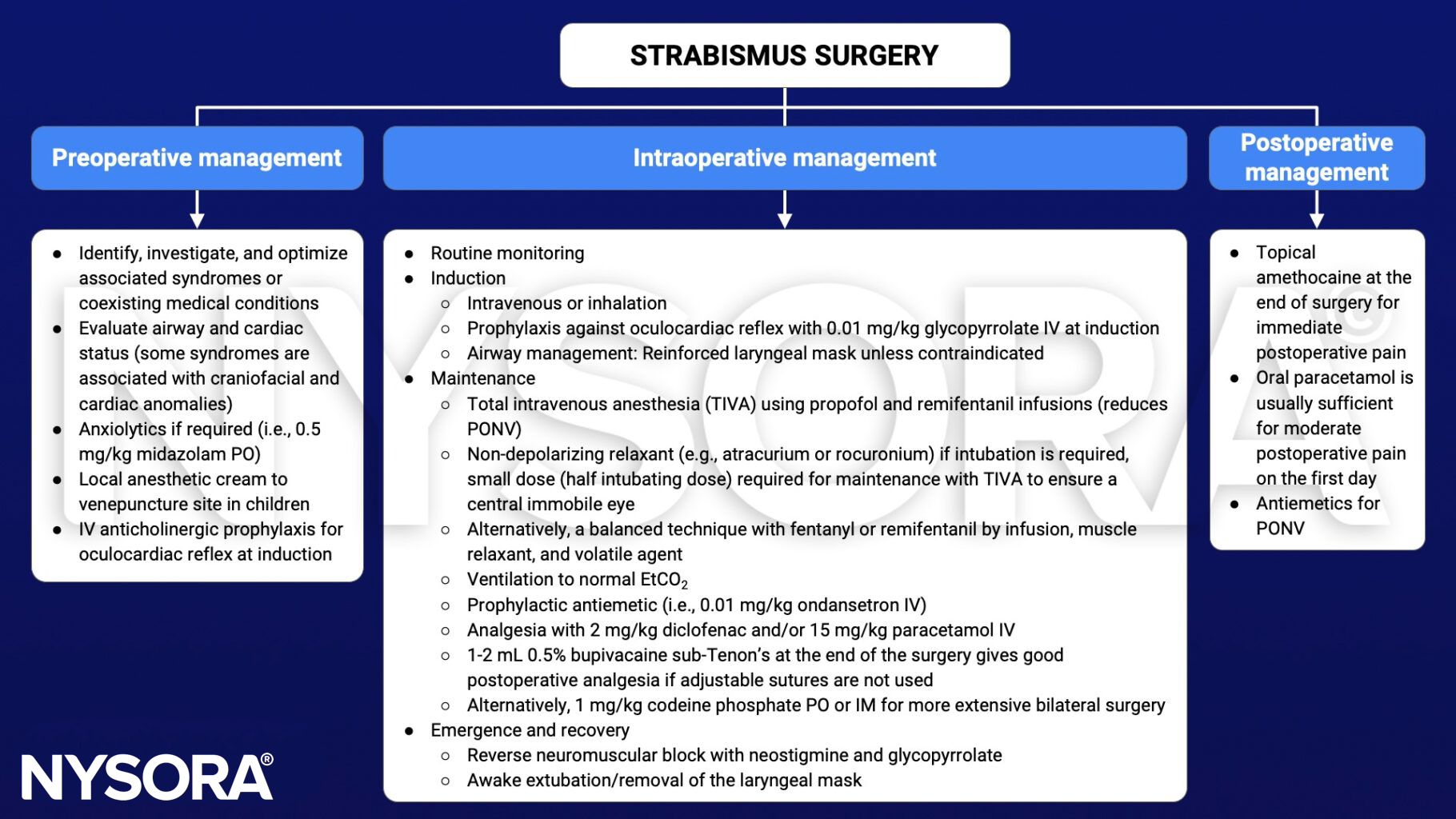
Management
Suggested reading
- Lewis H, James I. Update on anaesthesia for paediatric ophthalmic surgery. BJA Educ. 2021;21(1):32-38.
- Chua AW, Chua MJ, Leung H, Kam PC. Anaesthetic considerations for strabismus surgery in children and adults. Anaesthesia and Intensive Care. 2020;48(4):277-288.
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 18 Ophthalmic surgery, Slater RM.











