
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Define and classify the different types of bariatric surgery
- Describe the complications that are associated with bariatric surgery
- Anesthetic management of a patient undergoing bariatric surgery
Definition and classification
- Bariatric or weight loss surgery limits the amount of food a patient can comfortably eat or decreases the absorption of food and calories
- It is used as a later treatment option for obesity and helps to improve obesity-related conditions
- Hypertension
- Hyperglycemia
- Diabetes mellitus type 2
- Hypercholesterolemia
- Cardiovascular disease and stroke
- Kidney disease
- Obstructive sleep apnea
- Osteoarthritis
- Non-alcohol-related fatty liver disease
Classification
- Adjustable gastric band: Placement of an inflatable silicone band around the top portion of the stomach
- Gastric bypass surgery (e.g., Roux-en-Y gastric bypass): The stomach is divided into a small upper pouch and a much larger lower “remnant” pouch, and the small intestine is rearranged to connect to both
- Sleeve gastrectomy or gastric sleeve (irreversible): The stomach is reduced to 15% of its original size via surgical removal of a large portion of the stomach along the greater curvature
Working mechanism
Each procedure exerts its effects through at least one of the three mechanisms → procedures often affect several of these mechanisms
- Restricting: Restricting food intake (e.g., gastric sleeve)
- Reduce the size of the stomach that is available to hold a meal
- Filling the stomach faster enables the individual to feel more full after a smaller meal
- Blocking: Decreasing nutrient absorption (e.g., Roux-en-Y gastric bypass)
- Reduce the amount of intestine that the food passes through
- Reduces the ability of the intestines to absorb nutrients from the food
- Mixed: Affecting cell signaling pathways
- Alter hormones responsible for hunger (e.g., ghrelin) and satiety (e.g., leptin)
Patient characteristics
- Any age
- Males and females equally affected
- Increased incidence of
- Diabetes mellitus
- Cardiovascular disease
- Respiratory disease
- Sleep apnea syndrome
Complications
- Excess skin folds
- Malabsorption and malnutrition (e.g., vitamin and mineral deficiencies)
- Bile reflux
- Gallstones
- Kidney stones
- Blood clots in the leg (i.e., deep vein thrombosis) or lungs (i.e., pulmonary embolism)
- Infection
- Hernias
- Small bowel obstruction
- Anastomotic leaks
- Dumping syndrome
- Hypoglycemia
- Ulcers
- Vomiting
- Gastroesophageal reflux disease
- Metabolic bone disease (e.g., osteopenia and secondary hyperparathyroidism)
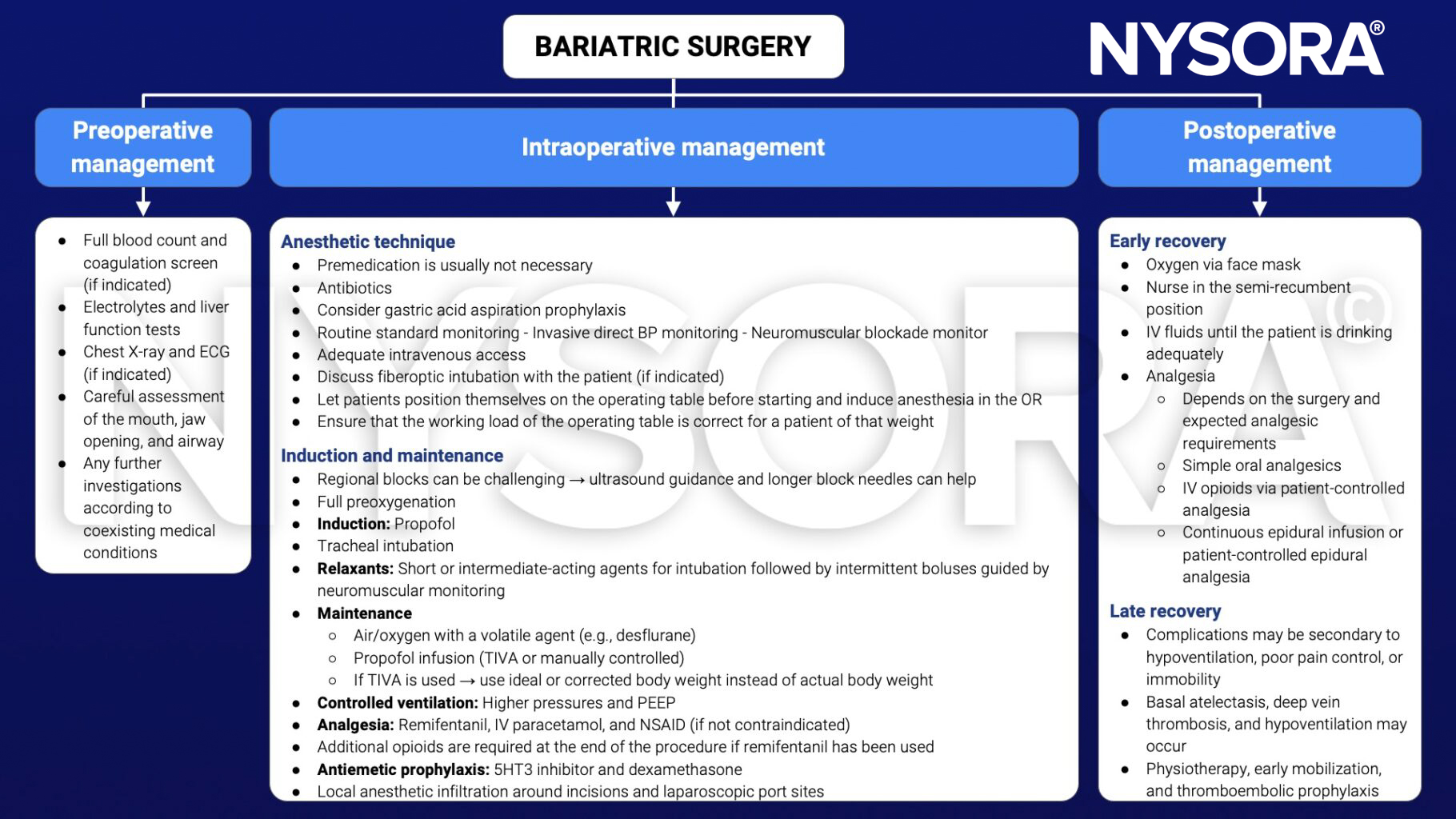
Management
See also obesity considerations
Suggested reading
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 10 Abdominal surgery.
Clinical updates
Ajetunmobi et al. (A&A, 2025) report in a double-blind RCT of 120 morbidly obese adults with OSA undergoing bariatric surgery that sugammadex (2 mg/kg) did not shorten recovery versus neostigmine 2.5 mg + glycopyrrolate 0.4 mg, with similar median OR discharge times and no meaningful differences in extubation time, early recovery milestones, or perioperative complications. This implies that routine reversal can remain neostigmine-based (given similar outcomes and much lower cost), while sugammadex is best reserved for specific scenarios (e.g., deeper blockade, rapid/“rescue” reversal needs, or when anticholinesterase side effects are a concern), ideally with quantitative neuromuscular monitoring to minimize residual blockade.
- Read more about this study HERE.
Debel et al. (EJA, 2026) provide updated PROSPECT recommendations for laparoscopic sleeve gastrectomy, identifying an evidence-based, opioid-sparing analgesic regimen. In addition to paracetamol and NSAIDs/COX-2 inhibitors, the update now recommends bilateral ultrasound- or laparoscopic-guided TAP blocks and port-site local anesthetic infiltration, plus a single intra-operative dose of IV dexamethasone, while gabapentinoids are no longer advised because of side effects. Opioids should be reserved for rescue analgesia, and techniques such as QLB, ESP blocks, opioid-free anaesthesia, dexmedetomidine, magnesium, and ketamine are not recommended due to unfavourable risk–benefit profiles or insufficient evidence.











