
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the posterior fossa
- Describe the indications for posterior fossa surgery
- Manage patients undergoing posterior fossa surgery
Background
- The posterior fossa is the deepest cranial fossa
- Surrounded by:
- Anteriorly: The dorsum sellae and basilar portion of the occipital bone (clivus)
- Laterally: The petrosal and mastoid components of the temporal bone
- Superiorly: The dural layer (tentorium cerebelli), and posteriorly and
- Inferiorly and posteriorly: The occipital bone
- Contains many important structures: the brainstem, cerebellum and lower cranial nerves
- The cerebrospinal fluid pathway is very narrow through the cerebral aqueduct and any obstruction can cause hydrocephalus which can result in a significant increase in intracranial pressure
Pathologies
- Tumors are the most common pathologies of the posterior fossa
- Pathologies which require surgical intervention:
| Tumors | Axial tumors | Medulloblastoma (most common) |
| Cerebellar astrocytoma | ||
| Brainstem glioma | ||
| Ependymoma | ||
| Choroid plexus papilloma | ||
| Dermoid tumours | ||
| Hemangioblastoma | ||
| Metastatic tumours | ||
| Cerebellopontine angle tumours | Schwannoma | |
| Meningioma | ||
| Acoustic neuroma | ||
| Glomus jugulare tumour | ||
| Vascular malformations | Posterior cerebellar artery aneurysm | |
| Vertebral/vertebrobasillar aneurysm | ||
| Basillar tip aneurysm | ||
| AV malformations | ||
| Cerebellar hematoma | ||
| Cerebellar infarction | ||
| Cysts | Epidermoid cyst | |
| Arachnoid cyst | ||
| Cranial nerve lesions | Trigeminal neuralgia (cranial nerve V) | |
| Hemifacial spasm (cranial nerve VII) | ||
| Glossopharyngeal neuralgia (cranial nerve IX) | ||
| Craniocervical abnormalities | Atlanto-occipital instability | Congenital |
| Acquired | ||
| Atlanto-axial instability | Congenital | |
| Acquired | ||
| Arnold–Chiarri malformation |
Management
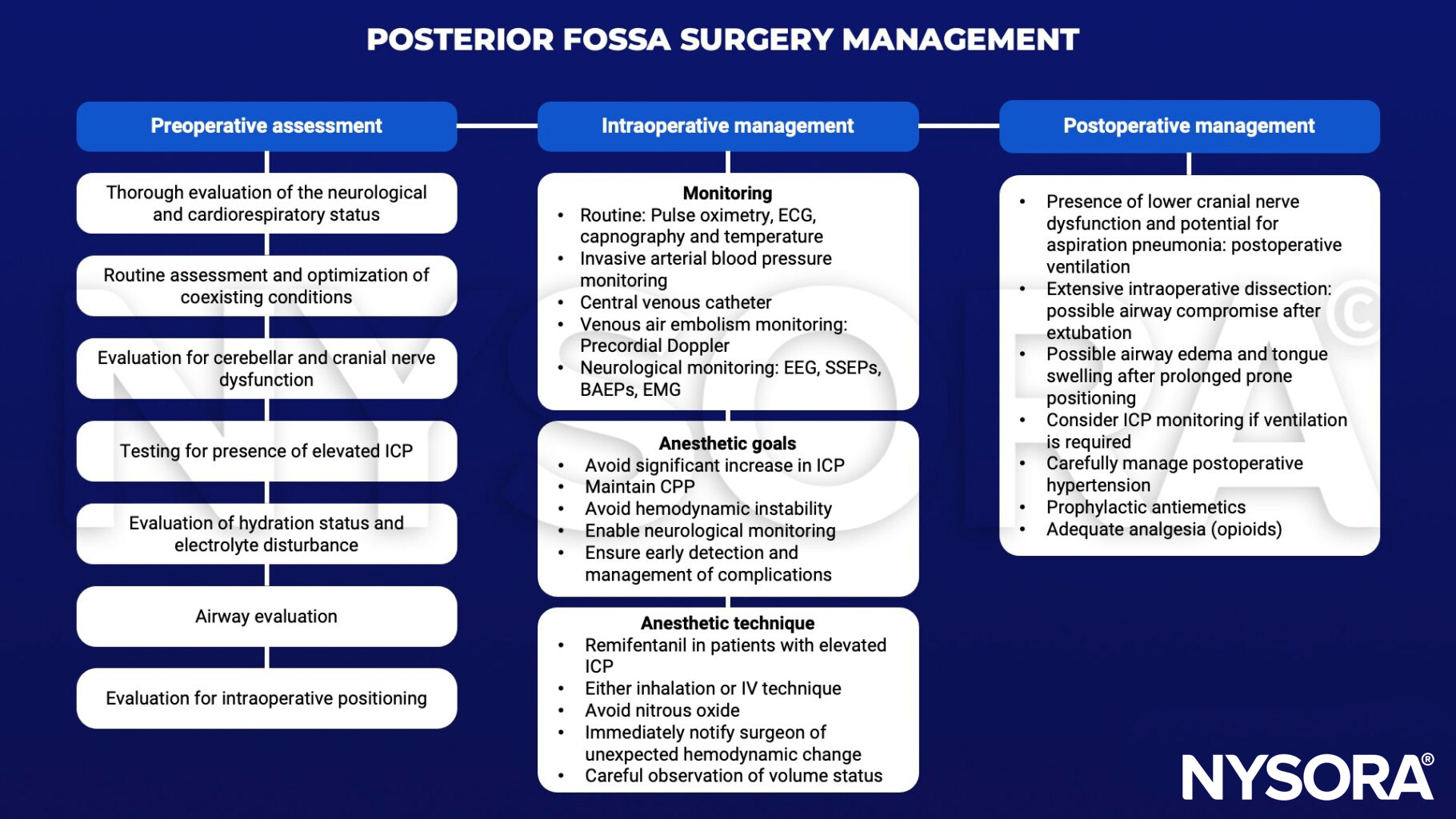
ICP, intracranial pressure; ECG, electrocardiography; EEG, electroencephalography; SSEP, somatosensory evoked potential; BAEP, brainstem auditory evoked potential; EMG, electromyography; CPP, cerebral perfusion pressure
Keep in mind
- Maintain consistent and modest levels of inhalation or IV anesthetic agents to minimize interference during SSEP monitoring
- Avoid neuromuscular blocking agents
- Use total IV anesthesia during motor evoked potential monitoring
- Intraoperative positioning
- The sitting position improves surgical access to the posterior fossa, but is associated with several potential complications:
| Complication | Management |
|---|---|
| Cardiovascular instability | Notify the surgeon of their proximity to vital structures |
| Venous air embolism | Administer high-concentration oxygen, discontinue nitrous oxide, maintain cardiovascular stability, central venous catheter to aspirate air from right atrium, immediate initiation of chest compression in the event of a massive air embolism with cardiac arrest |
| Pneumocephalus | High-flow oxygen, burr hole and aspiration of air in severe cases |
| Macroglossia | Ensure airway clearance |
| Quadriplegia | Avoid this complication by paying close attention to positioning and avoiding prolonged hypotension |
Suggested reading
- Sandhu K, Gupta N. Chapter 14 – Anesthesia for Posterior Fossa Surgery. In: Prabhakar H, editor. Essentials of Neuroanesthesia: Academic Press; 2017. p. 255-76.
- Jagannathan S, Krovvidi H. Anaesthetic considerations for posterior fossa surgery. Continuing Education in Anaesthesia Critical Care & Pain. 2014;14(5):202-6.











