

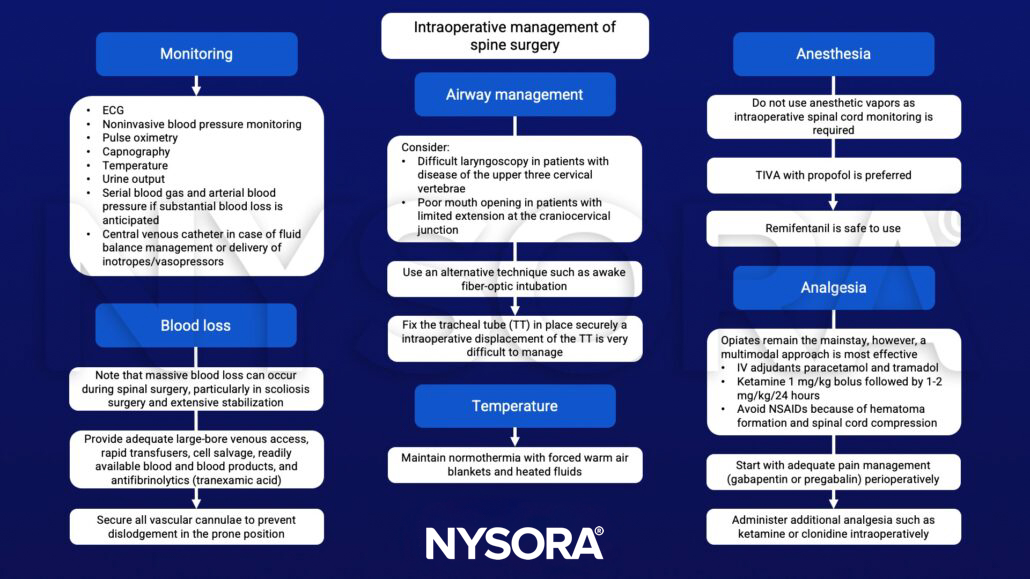
Learning objectives
- Anesthetic management of spine surgery
Definition and mechanisms
- The scope of spine surgery is vast
- Patients usually present with one of five pathologies at any site from cervical to lumbosacral:
- Major spinal surgery is often associated with major bleeding, infection, and postoperative respiratory complications
- 1% incidence of spinal cord damage
Surgical approach
- The majority of spinal procedures are performed in the prone position
- Exceptions: anterior cervical surgery, thoracic discectomies
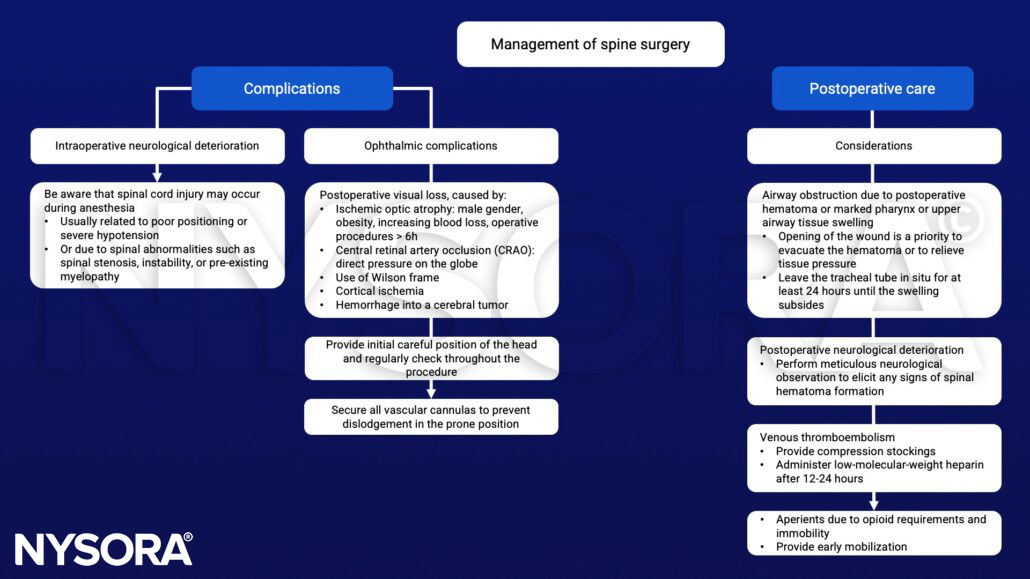
- Complications of the prone position:
- Accidental extubation
- Ophthalmic complications (corneal abrasions, postoperative visual loss)
- Peripheral nerve injury (ulnar nerve at the elbow, brachial plexus)
- Pressure injuries (skin necrosis, breast/genital injury)
- Abdominal compression (venous congestion in epidural veins, organ ischemia, impaired ventilation, lower limb thrombosis, and reduced cardiac output)
- Support the patient with pillow, gel pads, and foam bolsters to ensure that:
- The abdomen is free
- The head is at or above the level of the heart in a neutral position using a headrest or a Mayfield head fixator
- The eyes are taped closed, without padding, and free from external pressure, regularly checking them where possible
- The arms are in a natural position no more than 90° abduction with slight internal rotation paying particular attention to the ulnar nerve at
- the elbow
- Specific devices are available to facilitate proning: Montreal mattress, Jackson operating table, Wilson Frame, and the Andrews operating table
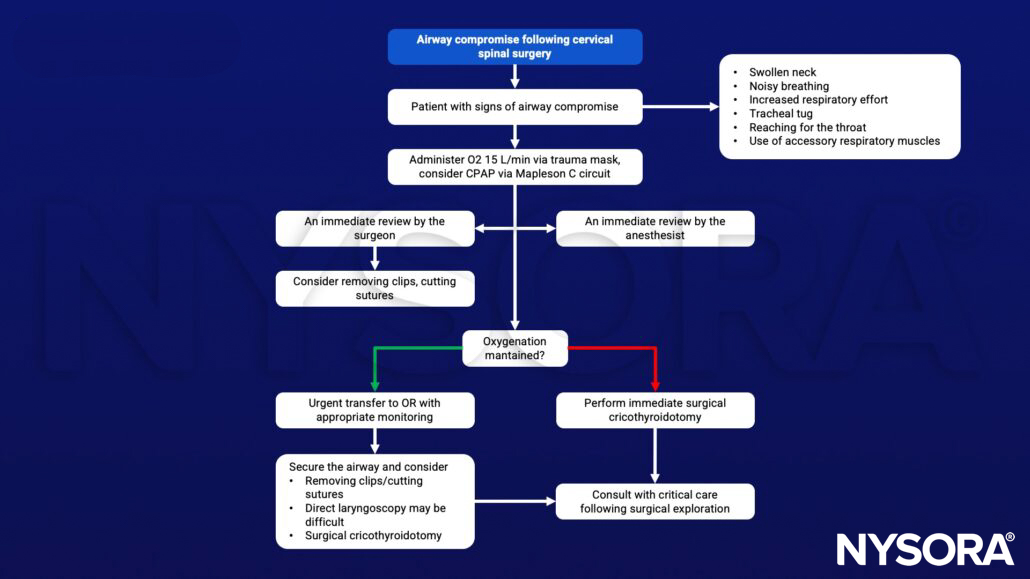
Management
Management of airway compromise following cervical spinal surgery
Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Nowicki R. 2014. Anaesthesia for major spinal surgery. Continuing Education in Anaesthesia Critical Care & Pain. 14;4:147-152.
Clinical updates
Schwenk et al. (Regional Anesthesia & Pain Medicine, 2025) report that intravenous acetaminophen offers no analgesic, opioid-sparing, or recovery advantage over oral acetaminophen in patients undergoing ambulatory lumbar spine surgery. In this randomized controlled trial, 24-hour opioid use, pain scores, quality of recovery, PACU length of stay, and PONV were equivalent between groups, despite IV acetaminophen being substantially more expensive. These findings support routine use of oral acetaminophen as a cost-effective component of multimodal analgesia in outpatient spine surgery, reserving IV administration for patients unable to tolerate oral intake.
- Read more about this topic HERE.











