

Learning objectives
- Describe the common indications for pituitary surgery
- Manage patients undergoing pituitary surgery
Background
- Pituitary adenomas are common in clinical practice
- Pituitary adenomas can be classified as either functioning or nonfunctioning, depending on whether they are hormone-secreting
- Patients with functioning adenomas frequently present with symptoms of hormone excess
- Patients with nonfunctioning adenomas often present later and have symptoms resulting from the mass effect of the tumor (headache, visual loss due to compression of the optic chiasm, hypopituitarism due to compression of the anterior pituitary)
- Common clinical conditions resulting from pituitary adenomas: Cushing’s disease, acromegaly, prolactin overproduction, panhypopituitarism
- Surgical resection has become the primary therapy when medical therapy fails with transsphenoidal pituitary surgery being the most common technique
- Transsphenoidal pituitary surgery presents unique challenges for anesthesia due to both the endocrine and neurosurgical management
Preoperative assessment
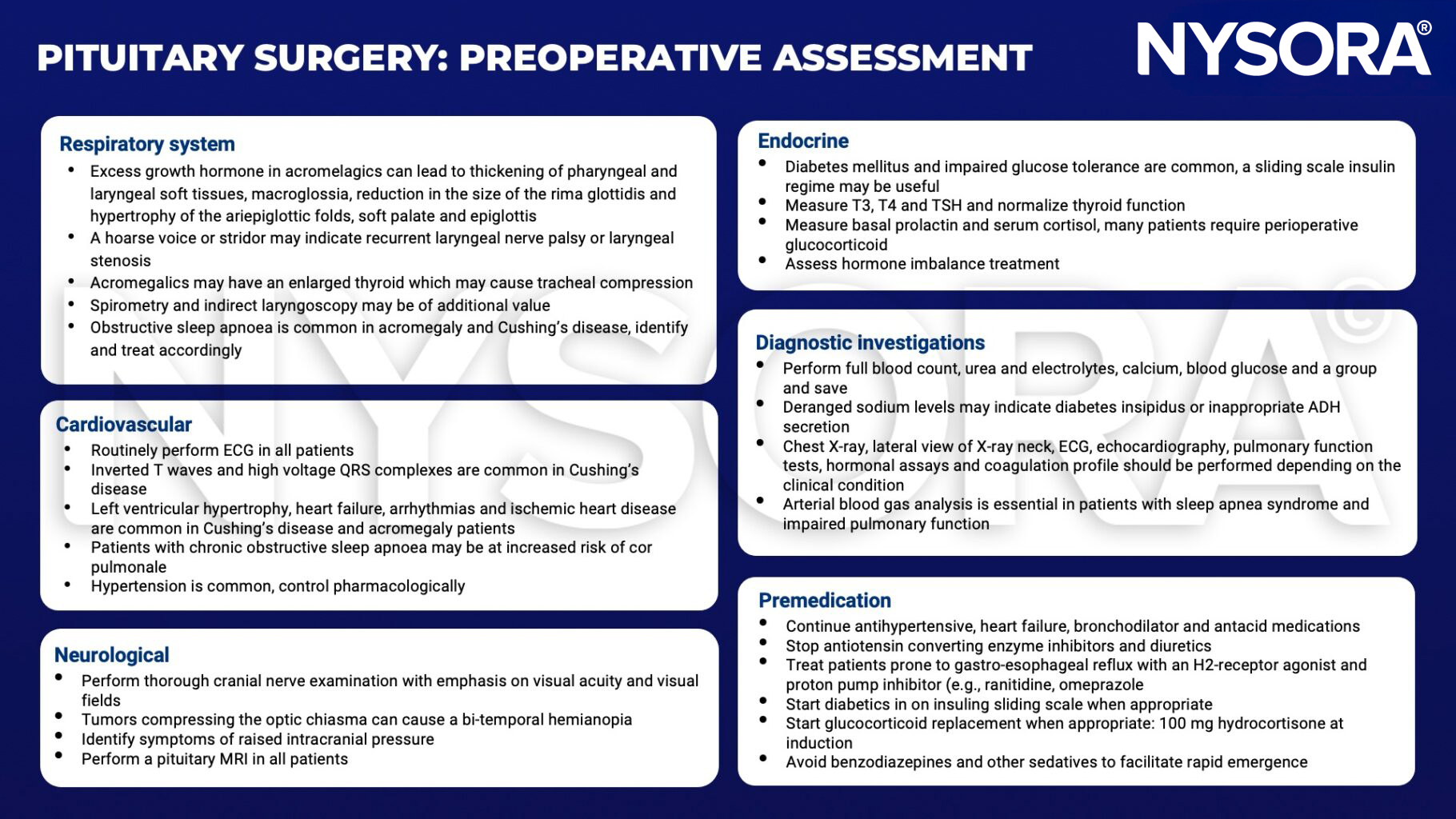
T3, triiodothyronine; T4, thyroxine; TSH, thyroid-stimulating hormone; ADH, antidiuretic hormone
Intraoperative management

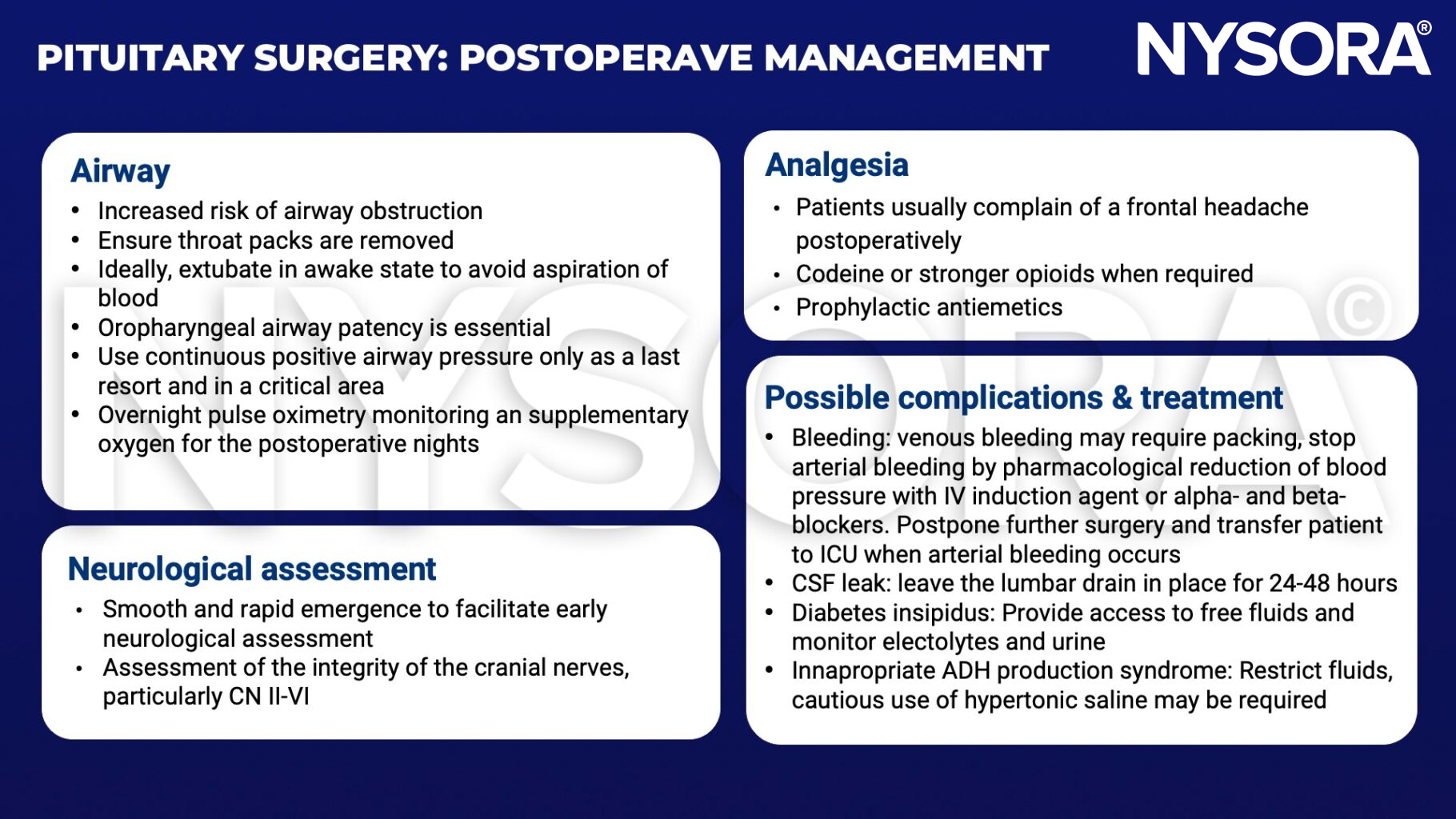
Postoperative management
Suggested reading
- Dunn LK, Nemergut EC. Anesthesia for transsphenoidal pituitary surgery. Curr Opin Anaesthesiol. 2013;26(5):549-554.
- Griffiths S, Perks A. The Hypothalamic Pituitary Axis Part 2: Anaesthesia For Pituitary Surgery. WFSA. Published July 26, 2010. Accessed January 19, 2023. https://resources.wfsahq.org/atotw/the-hypothalamic-pituitary-axis-part-2-anaesthesia-for-pituitary-surgery/
Clinical updates
Esfahani et al. (Current Opinion in Anesthesiology, 2021) emphasize that endoscopic transsphenoidal surgery is now preferred for most pituitary tumors, with anesthetic management focused on careful hemodynamic control (avoiding aggressive controlled hypotension due to potential cerebral ischemia), selective use of arterial lines, and smooth emergence using remifentanil or dexmedetomidine to reduce coughing and CSF leak risk. They highlight that routine lumbar drains are not clearly beneficial, dexamethasone is generally avoided due to suppression of postoperative cortisol assessment, and multimodal analgesia (e.g., scheduled acetaminophen and NSAIDs) significantly reduces postoperative opioid use and PONV.












