

Learning objectives
- Define and classify the different types of bariatric surgery
- Describe the complications that are associated with bariatric surgery
- Anesthetic management of a patient undergoing bariatric surgery
Definition and classification
- Bariatric or weight loss surgery limits the amount of food a patient can comfortably eat or decreases the absorption of food and calories
- It is used as a later treatment option for obesity and helps to improve obesity-related conditions
- Hypertension
- Hyperglycemia
- Diabetes mellitus type 2
- Hypercholesterolemia
- Cardiovascular disease and stroke
- Kidney disease
- Obstructive sleep apnea
- Osteoarthritis
- Non-alcohol-related fatty liver disease
Classification
- Adjustable gastric band: Placement of an inflatable silicone band around the top portion of the stomach
- Gastric bypass surgery (e.g., Roux-en-Y gastric bypass): The stomach is divided into a small upper pouch and a much larger lower “remnant” pouch, and the small intestine is rearranged to connect to both
- Sleeve gastrectomy or gastric sleeve (irreversible): The stomach is reduced to 15% of its original size via surgical removal of a large portion of the stomach along the greater curvature
Working mechanism
Each procedure exerts its effects through at least one of the three mechanisms → procedures often affect several of these mechanisms
- Restricting: Restricting food intake (e.g., gastric sleeve)
- Reduce the size of the stomach that is available to hold a meal
- Filling the stomach faster enables the individual to feel more full after a smaller meal
- Blocking: Decreasing nutrient absorption (e.g., Roux-en-Y gastric bypass)
- Reduce the amount of intestine that the food passes through
- Reduces the ability of the intestines to absorb nutrients from the food
- Mixed: Affecting cell signaling pathways
- Alter hormones responsible for hunger (e.g., ghrelin) and satiety (e.g., leptin)
Patient characteristics
- Any age
- Males and females equally affected
- Increased incidence of
- Diabetes mellitus
- Cardiovascular disease
- Respiratory disease
- Sleep apnea syndrome
Complications
- Excess skin folds
- Malabsorption and malnutrition (e.g., vitamin and mineral deficiencies)
- Bile reflux
- Gallstones
- Kidney stones
- Blood clots in the leg (i.e., deep vein thrombosis) or lungs (i.e., pulmonary embolism)
- Infection
- Hernias
- Small bowel obstruction
- Anastomotic leaks
- Dumping syndrome
- Hypoglycemia
- Ulcers
- Vomiting
- Gastroesophageal reflux disease
- Metabolic bone disease (e.g., osteopenia and secondary hyperparathyroidism)
Management
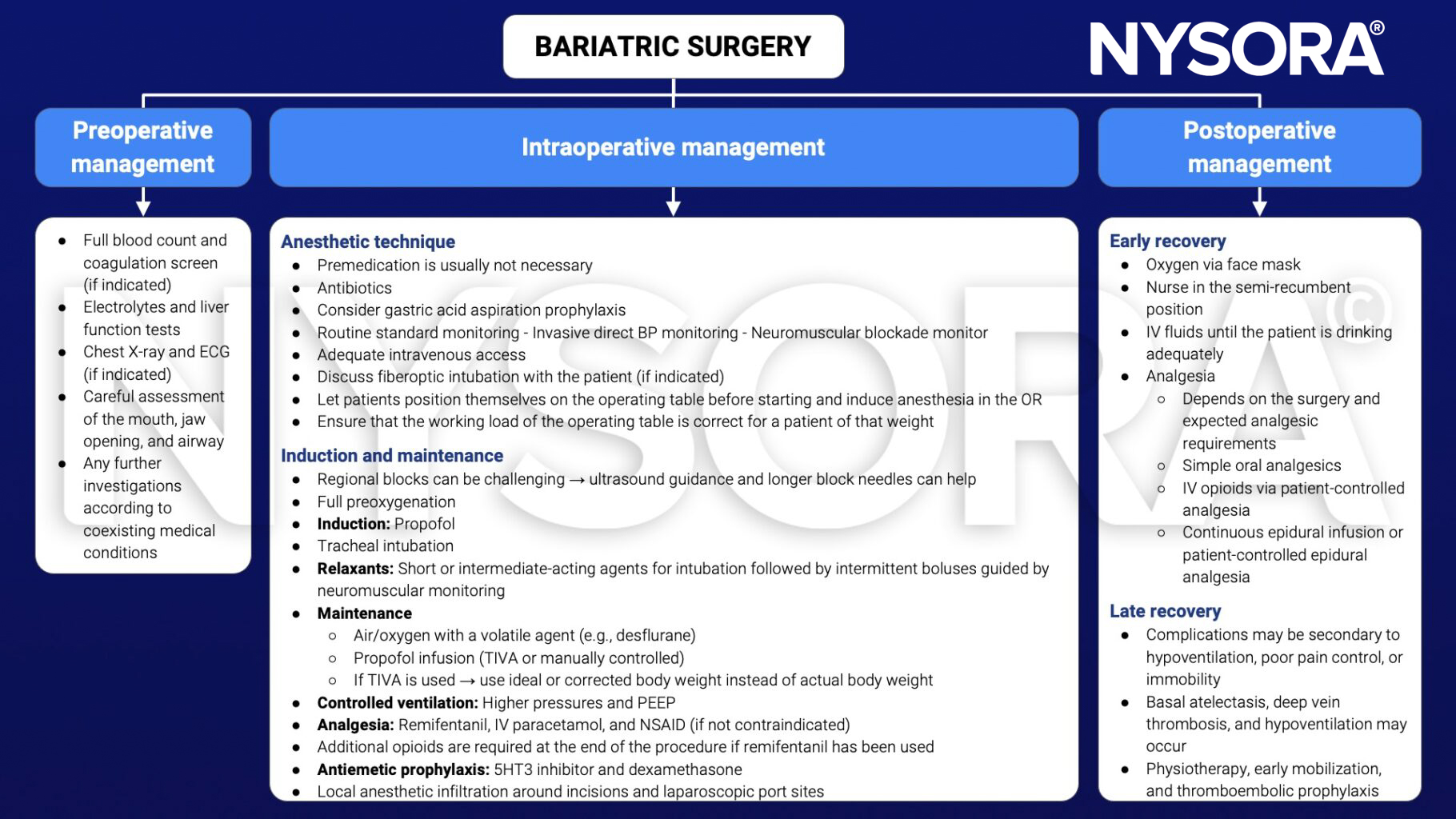
See also obesity considerations
Suggested reading
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 10 Abdominal surgery.
Clinical updates
Ajetunmobi et al. (A&A, 2025) report in a double-blind RCT of 120 morbidly obese adults with OSA undergoing bariatric surgery that sugammadex (2 mg/kg) did not shorten recovery versus neostigmine 2.5 mg + glycopyrrolate 0.4 mg, with similar median OR discharge times and no meaningful differences in extubation time, early recovery milestones, or perioperative complications. This implies that routine reversal can remain neostigmine-based (given similar outcomes and much lower cost), while sugammadex is best reserved for specific scenarios (e.g., deeper blockade, rapid/“rescue” reversal needs, or when anticholinesterase side effects are a concern), ideally with quantitative neuromuscular monitoring to minimize residual blockade.
- Read more about this study HERE.
Debel et al. (EJA, 2026) provide updated PROSPECT recommendations for laparoscopic sleeve gastrectomy, identifying an evidence-based, opioid-sparing analgesic regimen. In addition to paracetamol and NSAIDs/COX-2 inhibitors, the update now recommends bilateral ultrasound- or laparoscopic-guided TAP blocks and port-site local anesthetic infiltration, plus a single intra-operative dose of IV dexamethasone, while gabapentinoids are no longer advised because of side effects. Opioids should be reserved for rescue analgesia, and techniques such as QLB, ESP blocks, opioid-free anaesthesia, dexmedetomidine, magnesium, and ketamine are not recommended due to unfavourable risk–benefit profiles or insufficient evidence.











