Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the causes and consequences of ASD
- Recognize risk factors for ASD
- Diagnose ASD
- Anesthetic management of patients with ASD
Definition & mechanisms
- Atrial septal defect (ASD) is one of the most common types of congenital heart defects, occurring in about 25% of children
- Failure to close the septum between the right and left atria
- Small defects usually close spontaneously during childhood
- Large defects that do not close spontaneously may require percutaneous or surgical intervention
- Blood flows from the left atrium to the right atrium causing a left-to-right shunt
- Increase in pulmonary vascular resistance due to chronic volume overload, resulting in pulmonary hypertension
- Once pulmonary pressures equal systemic pressures, the shunt across the ASD reverses, and deoxygenated blood flows into the left atrium and systemically (Eisenmenger syndrome)
- Other complications:
- Atrial dysrhythmias
- Right-sided congestive heart failure
- Transient ischemic attack/stroke
Risk factors
| Secondary to inherited disorder | Down syndrome |
| Treacher-Collins syndrome | |
| Thrombocytopenia-absent radii syndrome | |
| Turner syndrome | |
| Noonan syndrome | |
| Maternal exposures | Rubella |
| Alcohol | |
| Drugs, e.g., cocaine |
ASD types
- Ostium secundum defect: Increased reabsorption of the septum primum in the atrium’s roof, or the septum secundum does not occlude the ostium secundum
- Ostium primum defect: Failure of the septum primum to fuse with the endocardial cushions
- Sinus venosus defect: Superior and inferior defects occur, and neither involves the true membranous septum:
- Superior defect: The orifice of the superior vena cava overrides the atrial septum above the oval fossa and drains both the left and right atria
- Inferior defect: The orifice of the inferior vena cava overrides both atria
- Coronary sinus defect: A defect or hole in the common wall between the left atrium and the coronary sinus creates a communication between the right and left atria
Diagnosis
- Transthoracic echocardiogram (gold standard diagnostic imaging modality)
- Cardiac CT and MRI
- Exercise testing can help determine the reversibility of shunt flow and the response of patients with pulmonary artery hypertension to activity
- Cardiac catheterization is contraindicated in young patients who present with small, uncomplicated ASDs.
- Differential diagnosis:
- Atrioventricular septal defect
- Ventricular septal defect
- Cyanotic congenital heart disease (sinus venosus defects and coronary sinus defects)
- Total anomalous pulmonary venous return
- Pulmonary stenosis
- Truncus arteriosus
- Tricuspid atresia
Management
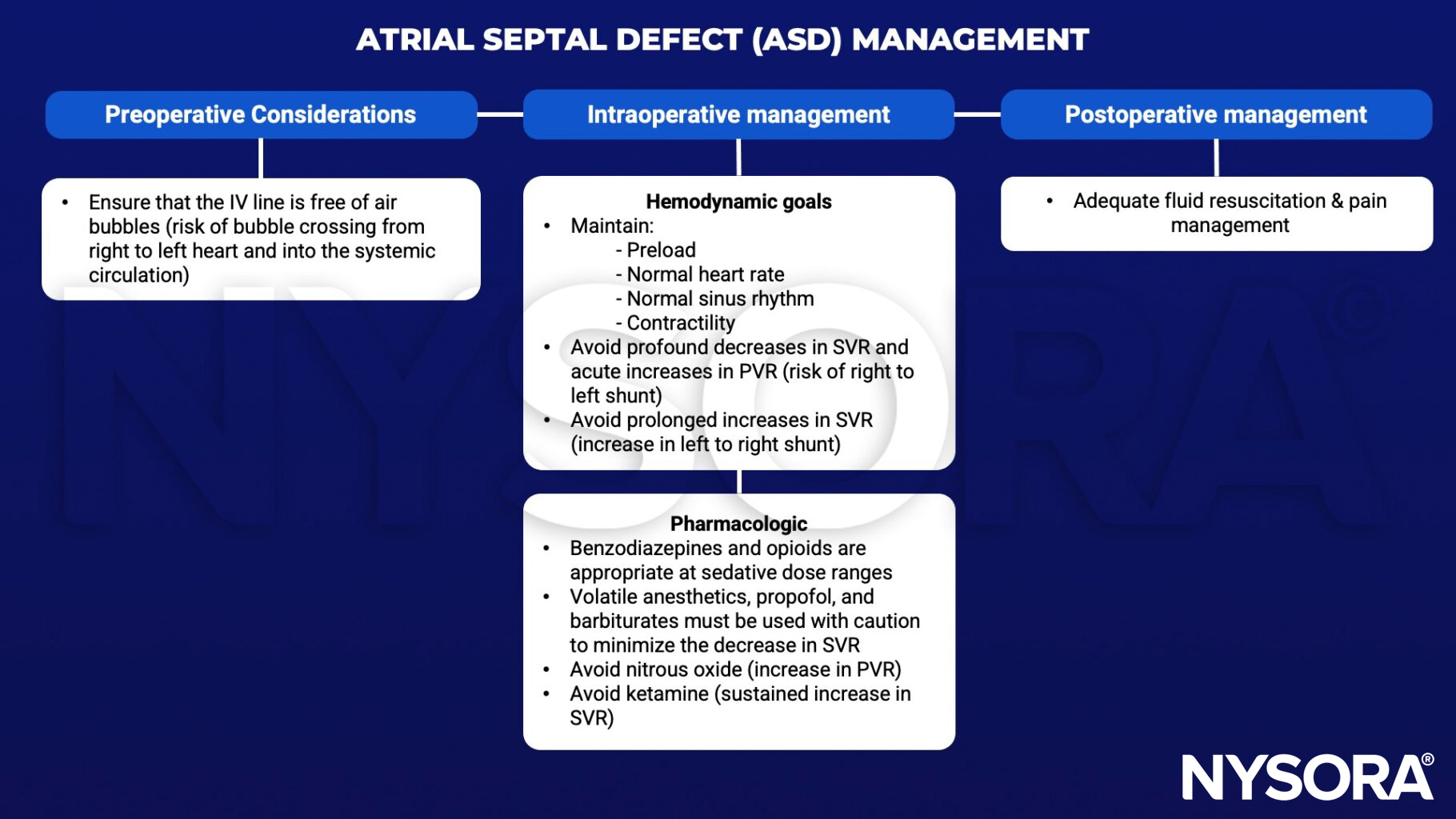
SVR, systemic vascular resistance; PVR, pulmonary vascular resistance
Suggested reading
- Menillo AM, Lee LS, Pearson-Shaver AL. Atrial Septal Defect. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535440/
- Yen P. ASD and VSD Flow Dynamics and Anesthetic Management. Anesth Prog. 2015;62(3):125-130.
- Calvert PA, Klein AA. Anaesthesia for percutaneous closure of atrial septal defects. Continuing Education in Anaesthesia Critical Care & Pain. 2008;8(1):16-20.