Learning objectives
- Recognize the risk factors for PDPH
- Recognize signs and symptoms of PDPH
- Take measures to reduce the risk of PDPH
- Make diagnostic assessments for PDPH
- Manage PDPH occurrence
Definition & mechanisms
- Post-dural puncture headache (PDPH) is a headache occurring within 5 days of a dural puncture, caused by cerebrospinal fluid leakage through the puncture
- It is usually accompanied by neck stiffness and/or subjective hearing symptoms
- PDPH usually remits spontaneously within 2 weeks
Risk factors
- Patient-related:
- Age: Uncommon in patients less than 10 years of age; peak incidence is in the teens and early 20s
- Gender: Nonpregnant females have twice the risk compared to age-matched men
- Equipment related:
- Needle gauge (larger > smaller)
- Needle tip design (cutting > noncutting)
Risk management after accidental dural puncture
- Stylet Replacement
- Subarachnoid Saline
- Intravenous Cosyntropin
- Limiting/Avoiding Pushing during labor
- Intrathecal Catheters
- Epidural Saline
- Epidural Opiates
- Prophylactic Epidural Blood Patch
Signs & symptoms
- Most cases of PDPH will be typical in
- Onset—often delayed, but within 48 hours
- Presentation—symmetric, bilateral headache
- Associated symptoms—more likely with severe headache
- Symptoms:
- Headache accompanied by at least one of these symptoms:
- Neck stiffness
- Tinnitus
- Hypoacusia
- Photophobia
- Nausea
Diagnosis
- PDPH diagnosis remains a diagnosis of exclusion, it is critical to rule out other etiologies
- Benign etiologies
- Nonspecific headache
- Exacerbation of chronic headache (e.g., tension-type headache)
- Hypertensive headache
- Pneumocephalus
- Sinusitis
- Drug-related side effect
- Spontaneous intracranial hypotension
- Other
- Benign etiologies
-
- Serious etiologies
- Meningitis
- Subdural hematoma (SDH)
- Subarachnoid hemorrhage
- Preeclampsia/eclampsia
- Intracranial venous thrombosis (ICVT)
- Other
- Serious etiologies
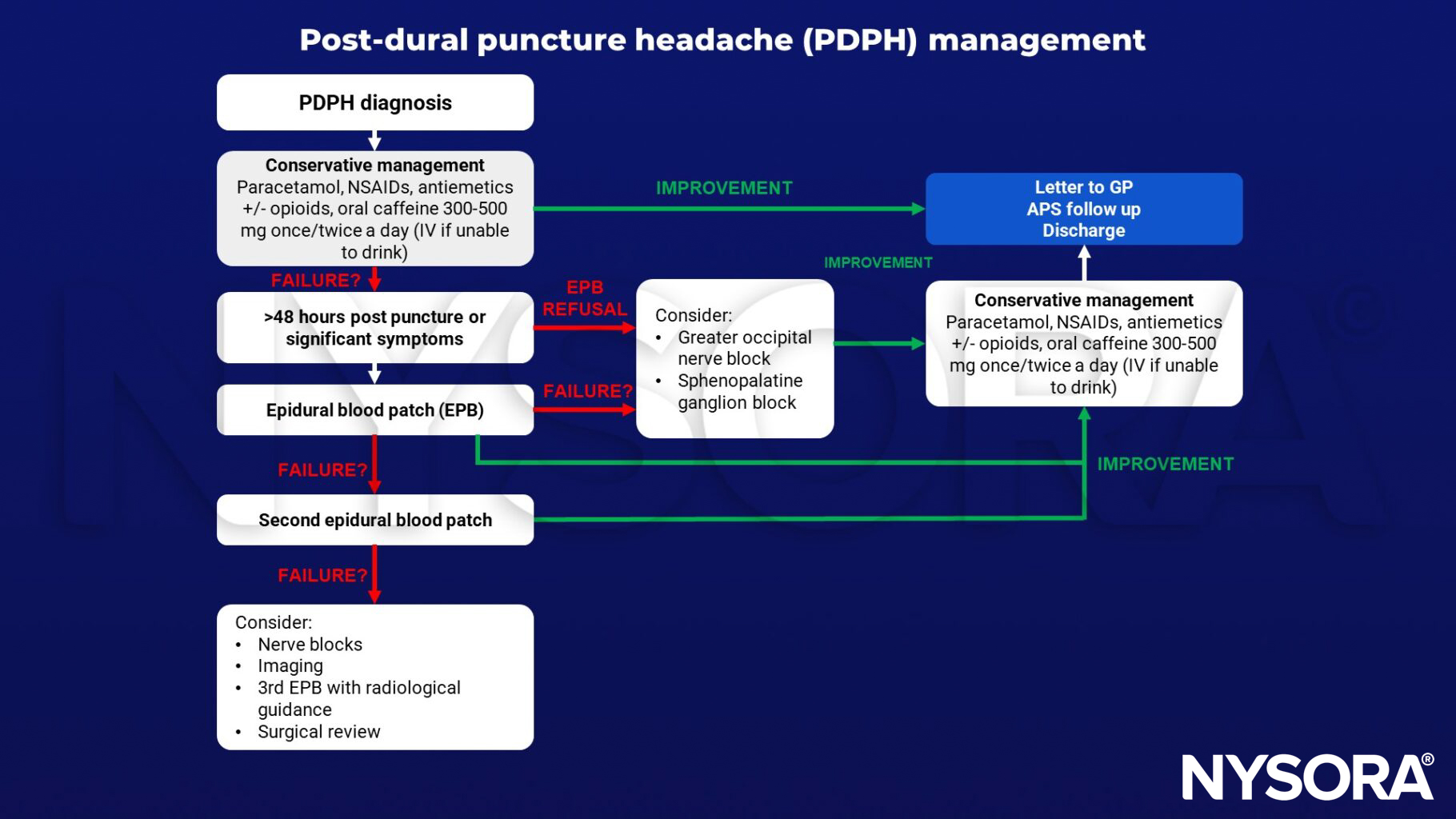
Management
Keep in mind
- There is no evidence to support the common practice of recommending bed rest and aggressive hydration in the prevention of PDPH
- PDPH may carry a risk of medicolegal liability
- ADP may result in chronic headache and back pain
- Anesthetic procedures with risk of PDPH require proper informed consent
Suggested reading
- Statement on post-dural puncture headache management. American Society of Anesthesiologists (ASA). https://www.asahq.org. Published October 13, 2021. Accessed December 14, 2022.
- Russell R, Laxton C, Lucas DN, Niewiarowski J, Scrutton M, Stocks G. Treatment of obstetric post-dural puncture headache. Part 2: epidural blood patch. Int J Obstet Anesth. 2019;38:104-118
Clinical updates
Uppal et al. (Reg Anesth Pain Med, 2024) present multisociety evidence-based guidelines on postdural puncture headache (PDPH), issuing 50 graded recommendations covering risk factors, prevention, diagnosis, and management, and emphasizing routine use of non-cutting spinal needles and narrower gauge cutting needles to reduce PDPH risk (Grade A). They conclude that prophylactic epidural blood patch and routine bed rest are not recommended due to insufficient or low-certainty evidence, while intrathecal catheter placement after inadvertent dural puncture may be considered but lacks definitive evidence for PDPH prevention, underscoring persistent gaps in high-quality data.
- Read more about the study HERE.
Thon et al. (Current Opinion in Anesthesiology, 2024) review contemporary evidence on postdural puncture headache (PDPH) management and reaffirm that epidural blood patch (EBP) remains the therapeutic gold standard for disabling or refractory symptoms, with high effectiveness, and should not be unnecessarily delayed. Newer data suggest that intrathecal catheter placement after accidental dural puncture may reduce the subsequent need for EBP, but evidence remains largely retrospective and insufficient to support routine prophylactic use. The review highlights growing but still limited evidence for noninvasive therapeutic local anesthetic strategies (e.g., greater occipital nerve block and sphenopalatine ganglion block) as bridging or alternative options when EBP is contraindicated, and emphasizes the need for improved patient selection and mechanistic research.
- Read more about the study HERE.
Schyns-van den Berg et al. (Best Practice & Research Clinical Anaesthesiology, 2024) challenge the traditional CSF-loss–only model of postdural puncture headache (PDPH), highlighting roles for cerebral vasodilation, trigeminovascular activation with CGRP release, autonomic dysfunction, and substance P alterations, and emphasizing that orthostatic headache can occur without demonstrable CSF leak. They reinforce evidence-based guidance favoring pencil-point spinal needles, note insufficient evidence for routine intrathecal catheters or sphenopalatine ganglion blocks, detail limited complete success rates of epidural blood patch after obstetric accidental dural puncture (≈33% in EPiMAP), and call for standardized definitions, multicenter registries, and multidisciplinary research to address long-term sequelae and optimize management.
- Read more about the study HERE.