Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About- The “erector spinae” comprises a group of muscles including the iliocostalis, longissimus, and spinalis muscles.
- They run bilaterally from the skull to the pelvis and sacral region, and from the spinous to the transverse processes, extending to the ribs.
- The muscles change their size and profile during their craniocaudal course alongside the spine. As part of the “core” muscles, one of their main functions is to stabilize the spine.
The erector spinae plane nerve block (ESPB) is a recently introduced technique, and clear indications are still not well defined. Likewise, the mechanism of action is not fully understood; some studies suggest that an anterior diffusion of the local anesthetic into the paravertebral space could be one of the explanations, although an interfascial spread toward the posterior rami of spinal nerves is probably the main mechanisms of action.
Technique
- SCANNING TECHNIQUE
After selecting the target transverse process for the nerve block, place the transducer in a paramedian sagittal orientation, approximately 2cm away from the midline (spinous processes), and try to vizualize the transverse process.
At higher thoracic levels, e.g., above T5; trapezius, rhomboid major and erector spinae muscles can be identified as three layers superficial to the transverse processes. In the lower and mid-thoracic levels, only the trapezius and erector spinae muscles can be seen.
From the Compendium of Regional Anesthesia: Cognitive priming for an erector spinae plane block.
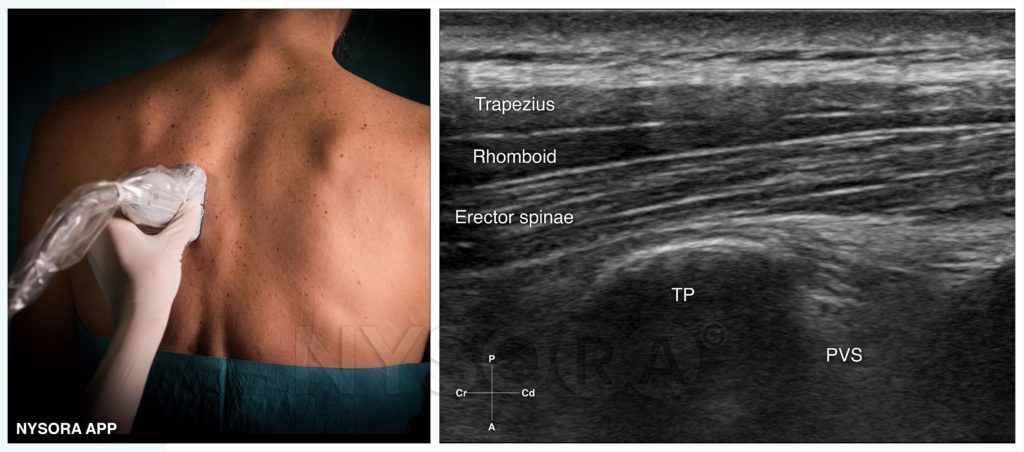
Probe position and ultrasound image for an erector spinae nerve block at the level of T5. Typically the rib-transverse process complex should be identified as a flat squared hyperechoic line with an acoustic shadow behind. Note that the pleura should not be visualized at the level where the nerve block is performed. TP, transverse process; PVS, paravertebral space; Cr, cranial, Cd, caudad; A, anterior; P, posterior.
- If the transducer is placed too medial, the thoracic laminae will be visualized as flat hyperechoic lines.
To fix: Slowly slide the transducer laterally. - When the transducer is placed too lateral, ribs will be visualized as rounded acoustic shadows with an intermediate hyperechoic pleural line.
To fix: Slowly slide the transducer medially.
- If the transducer is placed too medial, the thoracic laminae will be visualized as flat hyperechoic lines.

NYSORA‘s COMPENDIUM OF REGIONAL ANESTHESIA

Step-by-step techniques instructions for 60 nerve blocks

Custom illustrations, animations and clinical videos

Community for sharing real-life clinical tips

Access via desktop platform or mobile app

Infographics for exam preparation (e.g. EDRA)

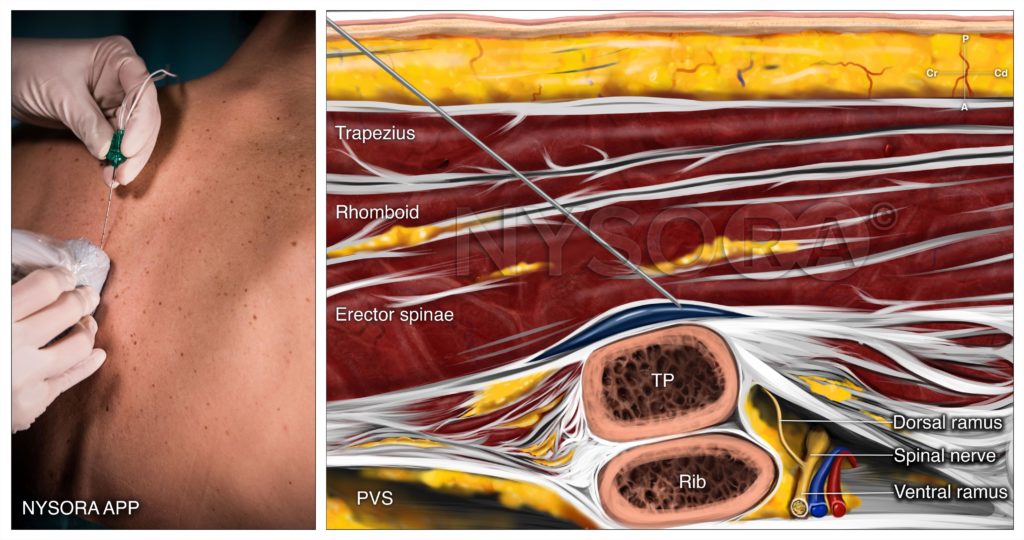
- INJECTION PROCEDURE
- Insert the needle in-plane from a cranial to caudad direction until the needle tip contacts the transverse process.
- Inject 1-3 mL of local anesthetic to confirm proper injection plane by visualization of a spread deep to the erector spinae muscles and superficial to the transverse process.
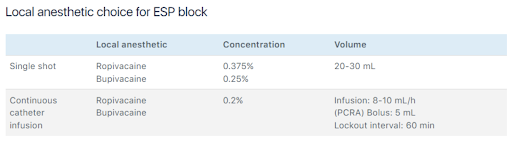
- Complete the nerve block with 20-30 mL of local anesthetic.

Reverse ultrasound anatomy of an ESPB with needle insertion in-plane from a cranial to caudad direction. The spinal nerve is exiting the paravertebral space (PVS) with the dorsal ramus branching and traveling posterior to innervate the posterior back muscles. TP, transverse process; PVS, paravertebral space. Cr, cranial, Cd, caudad; A, anterior; P, posterior.

The ESPB is a fascial plane block; therefore, success depends on the volume of local anesthetic injected between the muscle and transverse process. Long-acting local anesthetics or continuous infusions through catheters have been typically used.