Cesarean delivery is now one of the most frequently performed surgical procedures worldwide. As cesarean section rates continue to rise, anesthesiologists are increasingly focused on improving perioperative pain management while minimizing opioid exposure and maternal adverse effects.
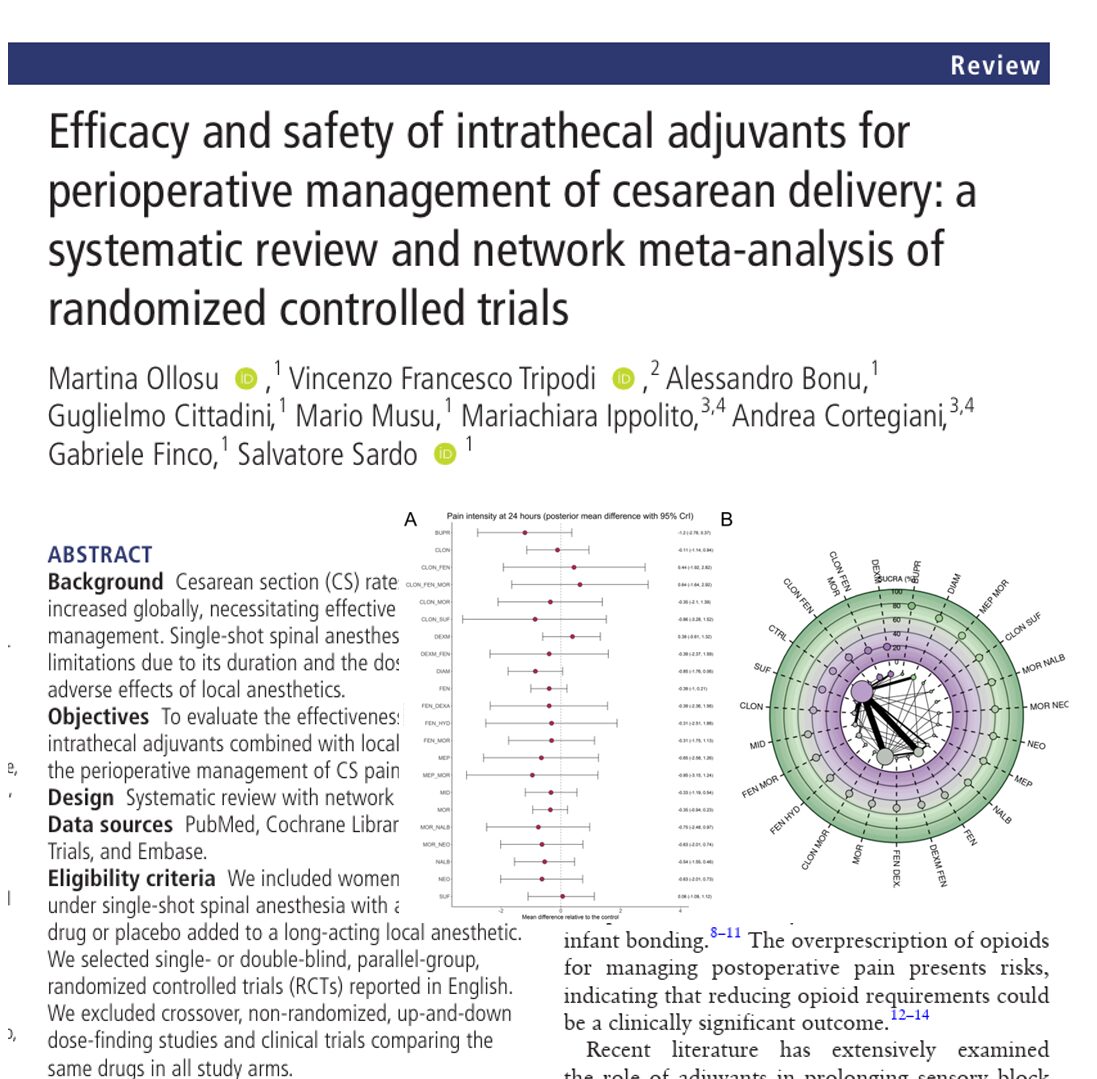
A major 2026 systematic review and network meta-analysis published in Regional Anesthesia & Pain Medicine evaluated the efficacy and safety of intrathecal adjuvants added to spinal anesthesia during cesarean delivery. The study analyzed 166 randomized controlled trials involving 14,925 patients and compared 32 different interventions.
The findings provide one of the most comprehensive comparisons to date of opioids, alpha-2 agonists, benzodiazepines, neostigmine, ketamine, dexamethasone, and combination therapies used during spinal anesthesia for cesarean section.
Why intrathecal adjuvants matter in cesarean anesthesia
Single-shot spinal anesthesia remains the preferred anesthetic technique for cesarean delivery because it:
- Avoids airway manipulation
- Reduces fetal drug exposure
- Allows maternal awareness during birth
- Facilitates immediate maternal-infant bonding
However, local anesthetics such as bupivacaine have limitations:
- Short duration of action
- Dose-dependent hypotension
- Limited postoperative analgesia
- Need for rescue opioid administration
Intrathecal adjuvants are therefore added to spinal anesthetic solutions to:
- Prolong sensory blockade
- Extend postoperative analgesia
- Reduce systemic opioid requirements
- Improve patient comfort
- Preserve early mobilization
The new review sought to determine which agents provide the best balance between analgesic efficacy and safety.
Study design and methodology
The investigators performed a systematic review and Bayesian network meta-analysis using data from:
- PubMed
- Embase
- Cochrane Library
Included studies involved pregnant women undergoing cesarean delivery with spinal anesthesia using:
- Bupivacaine
- Levobupivacaine
- Ropivacaine
The primary outcome was:
Pain intensity at 24 hours
Secondary outcomes included:
- Duration of effective analgesia
- Postoperative opioid consumption
- Duration of motor block
- Adverse events
The analysis incorporated:
- 166 randomized controlled trials
- 14,925 patients
- 32 treatment interventions
Most studies evaluated adjuvants combined with intrathecal bupivacaine.
Key findings
1. No adjuvant significantly reduced 24-hour pain scores
One of the most surprising findings was that no intrathecal adjuvant significantly reduced pain intensity at 24 hours compared with control.
The highest-ranked treatments were:
- Buprenorphine
- Diamorphine
- Meperidine plus morphine
However, the differences were not statistically significant.
What this means clinically
Although several adjuvants improved analgesic duration and reduced opioid use, none produced a clearly meaningful reduction in overall 24-hour pain scores.
This suggests that:
- Multimodal analgesia remains essential
- Intrathecal additives alone are insufficient
- Postoperative pain pathways are multifactorial
Why morphine performs well intrathecally
Morphine is hydrophilic, which means it:
- Spreads more extensively in cerebrospinal fluid
- Produces prolonged spinal receptor exposure
- Generates longer-lasting analgesia
Compared with lipophilic opioids such as fentanyl or sufentanil:
- Onset is slower
- Duration is much longer
- Cephalad spread is greater
This pharmacokinetic profile explains why intrathecal morphine remains the gold standard for post-cesarean analgesia.
3. Several adjuvants reduced postoperative opioid consumption
Reducing opioid requirements is increasingly important because excessive postoperative opioid prescribing contributes to:
- Maternal sedation
- Nausea and vomiting
- Delayed mobilization
- Risk of persistent opioid use
The study found major opioid-sparing effects with:
- Meperidine + morphine
- Diamorphine
- Diamorphine + fentanyl
- Morphine
- Morphine + neostigmine
The largest reduction occurred with meperidine plus morphine, which reduced oral morphine equivalents by more than 140 mg.
Morphine alone reduced opioid use by approximately 65 mg morphine equivalents.
Dexmedetomidine emerged as a powerful prolonger of spinal block
Dexmedetomidine has gained major attention in regional anesthesia over the past decade.
In this review, intrathecal dexmedetomidine:
- Significantly prolonged motor block
- Extended analgesia duration
- Reduced opioid consumption
However, prolonged motor blockade may delay:
- Early ambulation
- Maternal mobility
- Enhanced recovery pathways
This creates an important tradeoff between analgesic duration and postoperative function.
Mechanism of dexmedetomidine
Dexmedetomidine is an alpha-2 adrenergic receptor agonist.
Its analgesic effects include:
- Inhibition of nociceptive transmission
- Enhancement of descending inhibitory pathways
- Reduced neurotransmitter release in the dorsal horn
Because dexmedetomidine is not FDA-approved for intrathecal administration, its use remains off-label.
Safety findings
The overall safety profile was reassuring
The investigators found that most intrathecal adjuvants did not significantly increase severe complications.
Importantly:
- No significant increase in respiratory depression was identified
- Bradycardia rates were not significantly elevated
- Sedation and dizziness were generally not increased
However, certain adverse effects were associated with specific agents.
Adverse events linked to specific drugs
Meperidine
Associated with increased vomiting risk.
Buprenorphine
Associated with increased postoperative nausea and vomiting.
Sufentanil
Strongly associated with pruritus.
Clonidine
Associated with hypotension, especially when combined with neostigmine.
These findings emphasize that clinicians must balance analgesic efficacy against maternal tolerability.
Most important clinical takeaways
Intrathecal morphine still dominates
Morphine remains the most reliable intrathecal adjuvant for cesarean delivery because it:
- Prolongs analgesia substantially
- Reduces postoperative opioid requirements
- Maintains acceptable safety
Combination therapies may become more important
Several combinations outperformed single agents, including:
- Morphine + neostigmine
- Morphine + epinephrine
- Morphine + nalbuphine
- Meperidine + morphine
Future protocols may increasingly rely on multimodal intrathecal combinations.
Dexmedetomidine is promising but requires caution
Dexmedetomidine appears highly effective but raises concerns regarding:
- Prolonged motor block
- Delayed ambulation
- Off-label intrathecal administration
Further large-scale safety studies are still needed.
Conclusion
This landmark network meta-analysis provides the most comprehensive evaluation to date of intrathecal adjuvants used during cesarean delivery.
However, evidence quality remains limited, and more rigorous randomized trials are urgently needed before definitive clinical recommendations can be made.
For now, the study reinforces the central role of carefully selected intrathecal opioid-based strategies within multimodal enhanced recovery pathways for cesarean delivery.
Reference: Ollosu M et al. Efficacy and safety of intrathecal adjuvants for perioperative management of cesarean delivery: a systematic review and network meta-analysis of randomized controlled trials. Reg Anesth Pain Med. 2026;51:385-403.
Simulate your cases and access essential anesthesia knowledge, drug information, and perioperative guidance with the Anesthesia Assistant App.