Surgical procedures in patients with chronic kidney disease (CKD) present unique challenges, particularly concerning anesthetic management. Neuromuscular blocking agents (NMBAs) are essential in modern anesthesia, but their pharmacokinetics can be drastically altered in patients with impaired renal function.
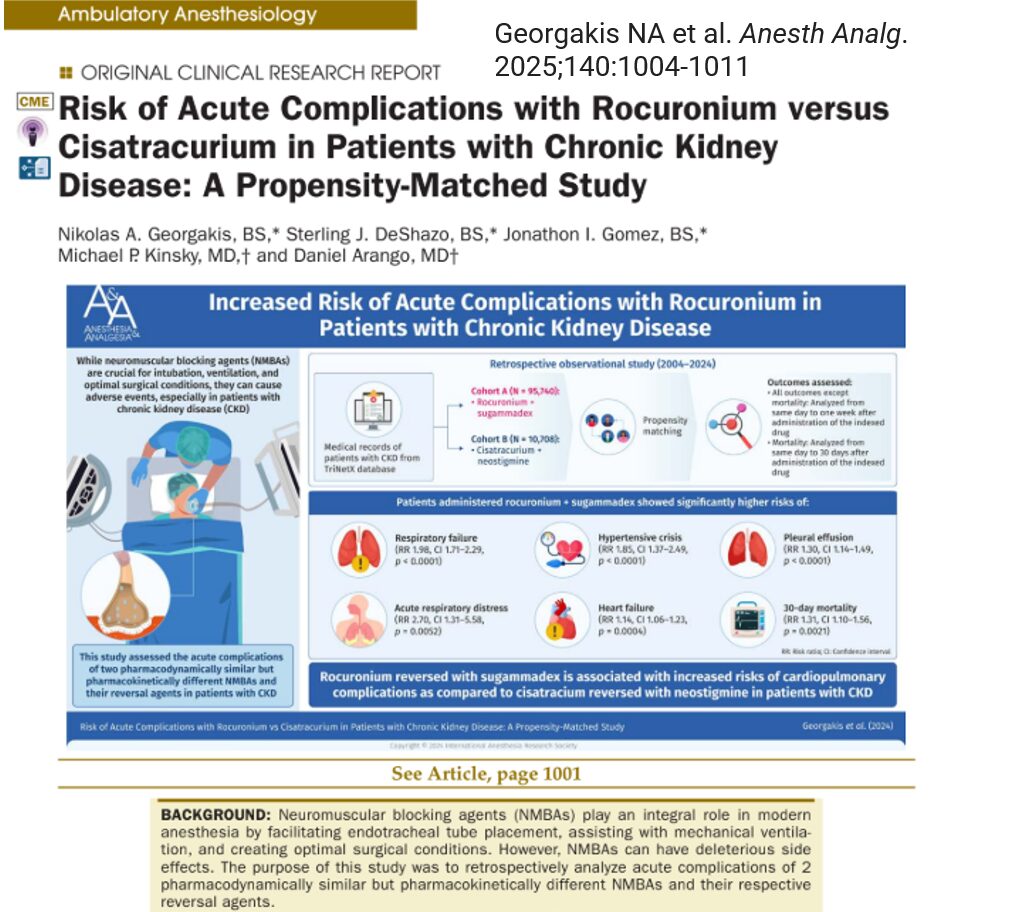
A study published in the May 2025 issue of Anesthesia & Analgesia by Georgakis et al. analyzed the comparative safety profiles of two widely used NMBAs, rocuronium and cisatracurium, in patients with CKD. This research is the first large-scale retrospective analysis to explore this topic, offering essential insights for anesthesiologists and perioperative care teams.
The role of NMBAs in anesthesia
Neuromuscular blocking agents are vital for:
- Facilitating smooth endotracheal intubation
- Enhancing mechanical ventilation
- Ensuring muscle relaxation for optimal surgical conditions
There are two main categories of NMBAs:
- Depolarizing agents (e.g., succinylcholine)
- Non-depolarizing agents (e.g., rocuronium, cisatracurium)
Non-depolarizing NMBAs are preferred due to fewer severe side effects. However, they differ in how the body metabolizes and excretes them, a critical consideration in CKD.
Study objectives and design
Objective
To determine whether rocuronium (with sugammadex) poses a higher risk of acute complications in CKD patients compared to cisatracurium (with neostigmine).
Methods
- Data Source: TriNetX database (over 93 million patients)
- Study period: April 2004 – April 2024
- Study type: Retrospective observational study
- Population: CKD patients aged 18–80 years
- Cohorts:
- Cohort A: Rocuronium + sugammadex
- Cohort B: Cisatracurium + neostigmine
Matching criteria
- Demographics: Age, sex, ethnicity, race
- Comorbidities: Atherosclerosis, COPD, pulmonary fibrosis, cardiomyopathy, peripheral vascular disease
- CKD stages 1–5 and end-stage renal disease (ESRD)
Key findings
After propensity matching:
- Each cohort included 10,675 patients
- Cohort A (rocuronium group) showed significantly higher risks for multiple adverse outcomes:
- Respiratory failure
- Acute respiratory distress
- Hypertensive crisis
- Heart failure
- Pleural effusion
- 30-day mortality
- Other outcomes, like cardiac arrhythmias and acute kidney injury, did not show significant differences.
Pharmacological comparison: rocuronium vs. cisatracurium
Rocuronium
- Metabolism: Liver and kidneys
- Excretion: Partially renal
- Reversal agent: Sugammadex
- Dosing: 0.6–1.2 mg/kg; short duration of action
- Concerns in CKD: Potential for accumulation, inflammatory effects
Cisatracurium
- Metabolism: Enzymatic hydrolysis and Hofmann elimination (independent of renal function)
- Reversal agent: Neostigmine
- Dosing: 0.15–0.2 mg/kg; longer duration of action
- Advantages in CKD: Safer metabolic pathway, fewer proinflammatory effects
Understanding the risk: how rocuronium may cause harm in CKD
Rocuronium, once bound by sugammadex, forms a complex that must be excreted renally. In CKD patients, this can lead to:
- Delayed clearance
- Higher systemic exposure
- Prolonged drug action
Rocuronium may also trigger immune responses, increasing C-reactive protein and promoting mast cell degranulation. Conversely, cisatracurium exhibits anti-inflammatory effects and does not require renal excretion.
Practical steps for anesthetic care in CKD patients
- Assess CKD stage and overall renal function preoperatively.
- Consider non-renal pathways for drug metabolism when choosing NMBAs.
- Monitor for delayed recovery from neuromuscular blockade.
- Evaluate the need for postoperative respiratory support more carefully in high-risk patients.
- Stay informed about ongoing trials comparing NMBAs in special populations.
Conclusion
This landmark study reveals that CKD patients given rocuronium reversed with sugammadex face higher rates of cardiopulmonary complications compared to those given cisatracurium with neostigmine. The differences are likely due to metabolic and inflammatory effects, coupled with delayed drug clearance in compromised renal function.
Although cisatracurium may be the safer option, clinical decisions must be individualized. Further research, especially randomized trials, is necessary to validate these findings and guide best practices in anesthetic care for CKD patients.
Reference:Georgakis NA et al. Risk of Acute Complications with Rocuronium versus Cisatracurium in Patients with Chronic Kidney Disease: A Propensity-Matched Study. Anesth Analg. 2025;140:1004-1011.
For more information on NMBAs, check out Anesthesia Updates on the NYSORA Anesthesia Manual App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.
AI on call: Case of the week
A 66-year-old female with stage 4 chronic kidney disease is scheduled for elective abdominal surgery under general anesthesia. Her medical history includes hypertension and heart failure with preserved ejection fraction.
Here’s what the Anesthesia Manual App recommends doing: