Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About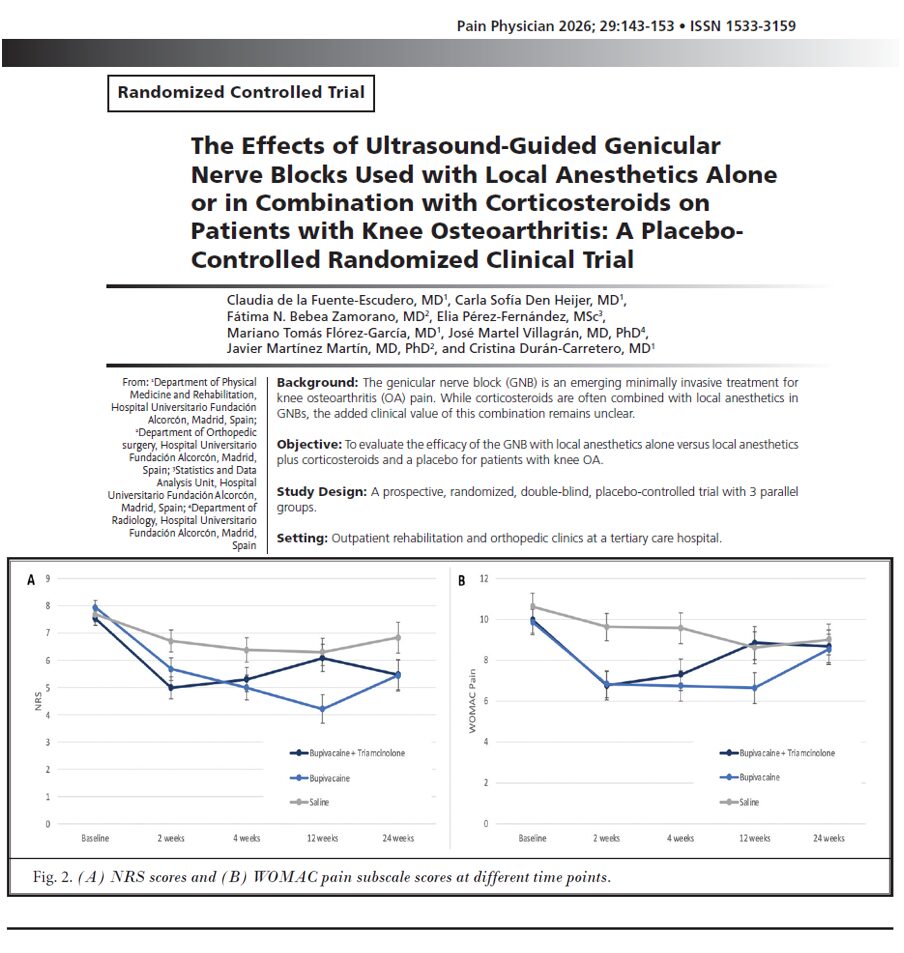

Knee osteoarthritis (OA) remains one of the leading causes of chronic pain and disability worldwide. Millions of patients struggle with persistent knee pain, reduced mobility, stiffness, sleep disruption, and decreased quality of life.
A newly published randomized clinical trial by de la Fuente-Escudero et al. in Pain Physician evaluated whether adding corticosteroids to ultrasound-guided genicular nerve blocks (GNBs) actually improves outcomes in patients with symptomatic knee OA. The findings suggest that local anesthetic alone may provide comparable, and in some cases superior, pain relief without the added risks associated with corticosteroids.
What is a genicular nerve block?
A genicular nerve block is a minimally invasive interventional pain procedure targeting the sensory nerves that innervate the knee joint capsule.
The procedure is commonly performed under ultrasound guidance and involves injection around the:
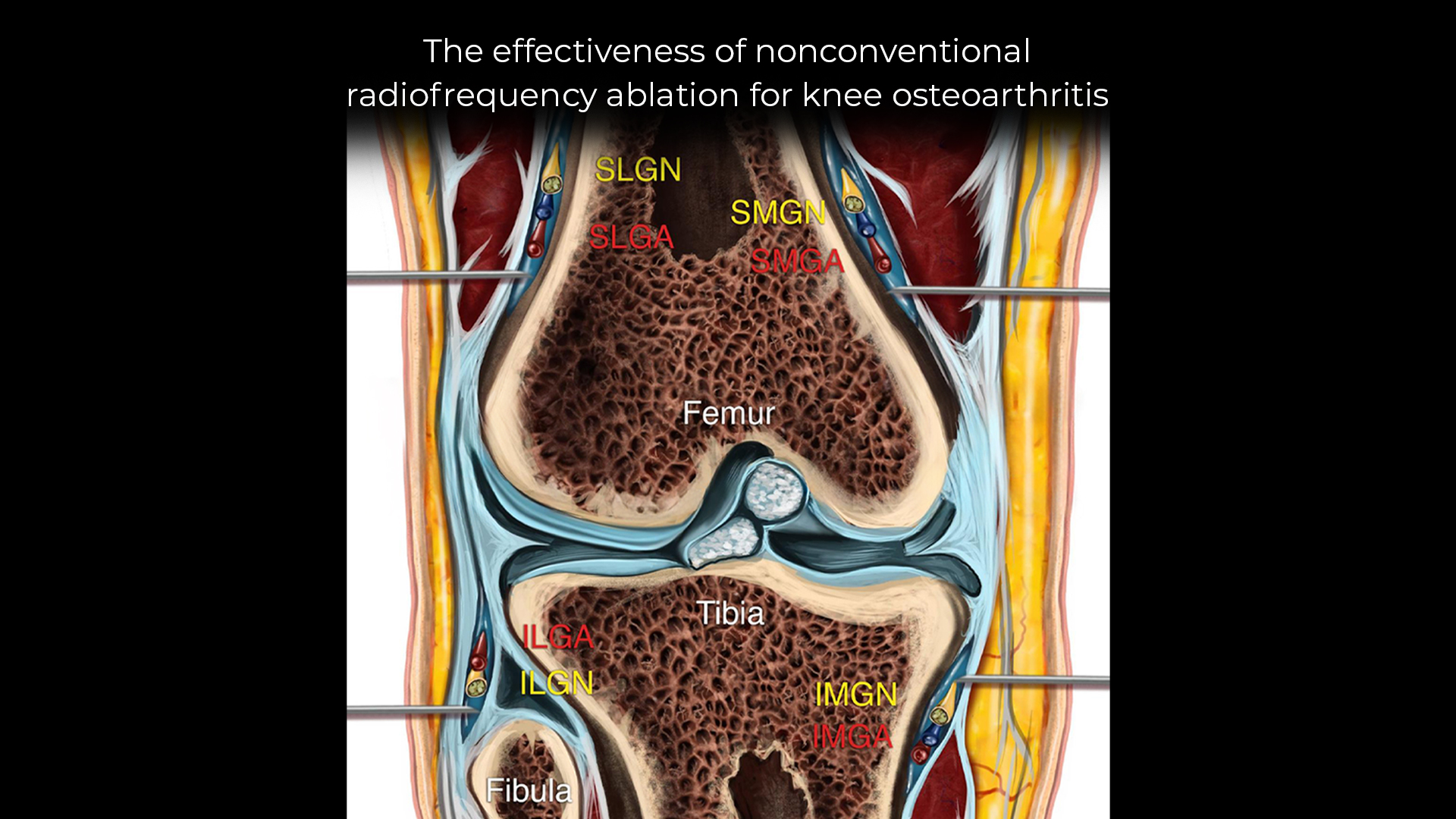
- Superomedial genicular nerve
- Inferomedial genicular nerve
- Superolateral genicular nerve
These nerves transmit pain signals from the osteoarthritic knee joint to the central nervous system. Blocking them can reduce pain and improve function.
Why this study matters
Corticosteroids are often combined with local anesthetics during GNBs due to their anti-inflammatory effects. However, steroids also carry potential adverse effects, including:
- Hyperglycemia
- Immunosuppression
- Local tissue degeneration
- Cartilage toxicity
- Systemic metabolic complications
The investigators sought to determine whether corticosteroids provide meaningful clinical benefit when combined with local anesthetics in knee OA nerve blocks.
Study design
Researchers conducted a prospective, randomized, double-blind, placebo-controlled study.
The study included 102 patients with symptomatic knee osteoarthritis treated at a tertiary care hospital in Spain between April 2023 and January 2024.
Treatment groups
Patients were randomized into three parallel groups:
- BC group
- 0.5% bupivacaine + 20 mg triamcinolone
- B group
- 0.5% bupivacaine alone
- S group
- Saline placebo
All procedures were ultrasound-guided.
Demographics
The average participant age was 70 years.
Additional baseline characteristics included:
- 72.5% female
- Nearly half classified as obese
- Most patients had pain for longer than 12 months
- More than 90% required analgesic medications
- Many had previously undergone interventional knee procedures
Importantly, all groups were comparable at baseline, improving the reliability of the findings.
Exercise therapy was included
Every participant also completed a standardized quadriceps-strengthening exercise program three times weekly.
The researchers emphasized that exercise remains a cornerstone of knee OA treatment and likely contributed to functional improvements across all groups.
Main findings
Significant pain reduction with active treatment
Both active treatment groups experienced greater pain reduction than the placebo group.
At 4 weeks:
- BC group pain reduction:
- 2.24 points on the Numeric Rating Scale (NRS)
- B group pain reduction:
- 2.94 points
- Saline group pain reduction:
- 1.29 points
Benefits persisted up to 24 weeks
The analgesic effect continued for up to six months in both active treatment groups.
However, the bupivacaine-only group demonstrated a more sustained improvement trajectory over time compared with the steroid-containing group.
Functional improvement outcomes
Researchers assessed physical function using several validated instruments:
- WOMAC
- KOOS
- Kujala score
WOMAC function improved
The WOMAC physical function subscale showed statistically significant improvement in the bupivacaine-only group.
KOOS and Kujala scores
No statistically significant differences were observed among groups for:
- KOOS
- Kujala scale
- WOMAC stiffness scores
Mood outcomes
Researchers also evaluated mood changes using the Escala de Valoración del Estado de Ánimo (EVEA).
No meaningful differences emerged between groups regarding:
- Sadness
- Anxiety
- Hostility
- Happiness
Safety profile
The procedure appeared highly safe overall.
No serious adverse events
No participants experienced severe complications or discontinued treatment due to adverse effects.
Minor side effects reported
Nine patients experienced mild transient complications:
- Temporary knee pain
- Injection-site hematoma
- Brief instability sensation
- Temporary toe hypoesthesia
Interestingly, adverse events occurred more often in the bupivacaine-only group than placebo, although events remained minor and self-limited.
Why avoiding steroids could be important
The study’s most clinically relevant finding was that corticosteroids did not appear to improve outcomes beyond the local anesthetic alone.
This may influence future interventional pain management strategies because avoiding steroids could reduce risks in patients with:
- Diabetes mellitus
- Obesity
- Immunosuppression
- Osteoporosis
- Cardiovascular disease
Understanding the mechanism
Bupivacaine is a long-acting local anesthetic that selectively blocks sensory nerve conduction.
The investigators noted that genicular nerve blocks may also:
- Facilitate rehabilitation
- Improve participation in strengthening exercises
- Reduce opioid use
- Delay surgery in some patients
Clinical implications
The findings challenge a common assumption in interventional pain medicine that steroids necessarily enhance peripheral nerve block efficacy.
Potential implications include:
- Simplified injection protocols
- Lower systemic corticosteroid exposure
- Reduced metabolic complications
- Safer treatment for high-risk patients
- Cost reduction
Limitations of the study
The authors acknowledged several limitations:
- Single-center design
- Modest sample size
- Six-month follow-up only
- Exercise adherence is not systematically tracked
- Treating physicians could not be blinded
Larger multicenter trials are still needed.
Key takeaways
- Genicular nerve blocks significantly reduced knee OA pain
- Bupivacaine alone performed as well as or better than steroid-containing injections
- Benefits persisted up to six months
- Functional improvement was observed
- Serious adverse events were absent
- Avoiding corticosteroids may improve safety
Future directions
Future studies may explore:
- Longer follow-up durations
- Repeated injection protocols
- Combination with supervised rehabilitation
- Comparison with radiofrequency ablation
- Head-to-head comparisons with hyaluronic acid or platelet-rich plasma
Conclusion
This randomized placebo-controlled trial provides important evidence supporting the use of ultrasound-guided genicular nerve blocks with local anesthetic alone for symptomatic knee osteoarthritis.
The addition of corticosteroids did not improve outcomes and may be unnecessary for many patients. As clinicians increasingly seek effective non-surgical and opioid-sparing therapies for knee OA, steroid-free genicular nerve blocks may become an increasingly attractive option.
For more information, refer to the full article in Pain Physician.
de la Fuente-Escudero C, Den Heijer CS, Zamorano FNB, et al. The Effects of Ultrasound-Guided Genicular Nerve Blocks Used with Local Anesthetics Alone or in Combination with Corticosteroids on Patients with Knee Osteoarthritis: A Placebo-Controlled Randomized Clinical Trial. Pain Physician. 2026;29(2):143-153.
Explore the newly released Deluxe Edition of the Ultrasound-Guided Interventional Pain Procedures Manual for expert guidance on genicular nerve blocks, ultrasound anatomy, and evidence-based pain interventions.