Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About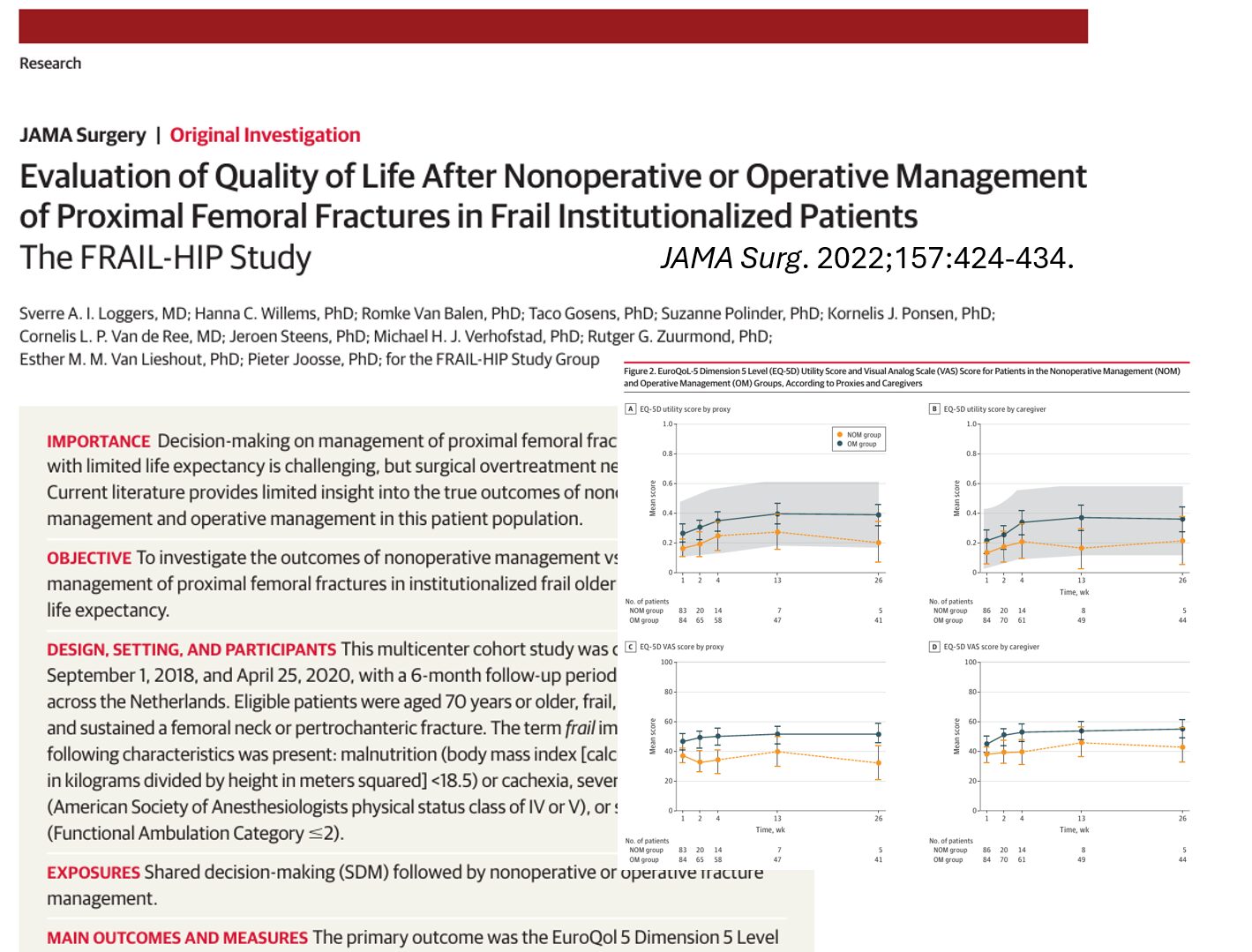





Introduction: rethinking hip fracture management in the frail elderly
Hip fractures are a serious, often terminal event in the lives of frail older adults. Traditionally, the medical standard has leaned heavily toward surgical intervention. Yet, for institutionalized patients with limited life expectancy, this one-size-fits-all model may not be optimal. A pivotal 2022 study published in JAMA Surgery, the FRAIL-HIP study, challenges this convention by rigorously comparing nonoperative and operative treatments in a unique patient group.
Understanding the FRAIL-HIP study
What was the purpose of the study?
The FRAIL-HIP study aimed to evaluate whether nonoperative management of proximal femoral fractures in frail, institutionalized older patients was a noninferior alternative to surgery in terms of health-related quality of life (HRQoL).
Who was included?
The study enrolled 172 institutionalized patients aged 70 and older with:
- Proximal femoral fractures (femoral neck or pertrochanteric).
- Evidence of frailty, including:
- Malnutrition (BMI < 18.5).
- Severe comorbidities (ASA class IV or V).
- Significant mobility impairments (FAC ≤ 2).
Study design highlights:
- Multicenter prospective cohort across 25 Dutch hospitals.
- Treatment selected via structured shared decision-making (SDM).
- Primary outcome: EQ-5D utility score measured by proxies/caregivers.
- Follow-up at 1, 2, 4 weeks, and 3 and 6 months.
Shared decision-making: a cornerstone of patient-centered care
The study emphasized a formal SDM process, a collaborative discussion involving:
- Trauma surgeons.
- Geriatricians.
- Elder care physicians.
- Proxies or family members.
This approach ensured that treatment choices were aligned with patient values, including the option to choose comfort-focused care over aggressive surgical interventions.
Comparative results: surgery vs nonoperative management
Quality of life (primary outcome)
- EQ-5D utility scores in the nonoperative group stayed within the pre-specified noninferiority margin of 0.15 compared to the operative group.
- At week 4, scores were:
- Nonoperative: 0.24
- Operative: 0.34
Pain and comfort
- Initial pain was higher in the nonoperative group during week 1:
- 88% experienced pain vs 67% in the surgical group.
- By week 2, pain levels were similar (~55% in both).
- Nonoperative patients required higher morphine doses.
Adverse events (AEs)
- Fewer AEs in nonoperative patients:
- Nonoperative: 67 events.
- Operative: 167 events.
- Surgical patients had:
- More delirium (32%).
- More infections and transfusions.
- 6% required reoperations.
Mortality rates
- 30-day mortality:
- Nonoperative: 83%
- Operative: 25%
- 6-month mortality:
- Nonoperative: 94%
- Operative: 48%
- Median time to death:
- 7 days for nonoperative.
- 29 days for the operative group.
Functional outcomes
- Only 29% of surgical patients regained preinjury mobility.
- 89% of nonoperative patients remained bedbound.
- ADL dependency remained high across both groups.
Treatment satisfaction
- Proxies rated satisfaction high in both groups.
- Median score: 8/10.
- Quality of dying rated “good–almost perfect” by:
- 51% in the nonoperative group.
- Only 4% rated it “poor”.
Interpreting the findings
Does nonoperative care mean inferior quality of life?
No. Despite higher early mortality, nonoperative care yielded similar HRQoL scores and high satisfaction, aligning better with palliative care goals.
What about mobility and recovery?
Surgical patients had a slightly higher chance of regaining mobility, but overall functional recovery was limited in both groups, reflecting the severity of frailty.
How should clinicians interpret the high mortality?
This population already had a limited life expectancy. The fracture was often a marker of decline, not the sole cause of death.
When to consider nonoperative treatment
Use these 5 clinical steps:
- Assess frailty: Identify markers like BMI < 18.5, ASA IV/V, or severe mobility loss.
- Initiate shared decision-making by engaging proxies and interdisciplinary teams.
- Discuss realistic outcomes by using data from FRAIL-HIP to set expectations
- Implement comfort-focused care by ensuring robust pain control and palliative protocols.
- Evaluate outcomes: Monitor HRQoL, symptom relief, and family satisfaction.
Implications for policy and clinical practice
- The study recommends integrating SDM tools into guidelines for hip fracture treatment.
- Training clinicians in palliative decision-making and communication is essential.
- Long-term care facilities should establish advance care planning protocols for residents at high fracture risk.
Final thoughts
The FRAIL-HIP study introduces a paradigm shift: nonoperative management of proximal femoral fractures can be a rational, compassionate, and evidence-based choice in specific frail populations. Surgery should not be the default, especially when quality of life and dignity in dying are prioritized.
Clinicians, caregivers, and healthcare systems must adopt individualized care rooted in patient values, balancing life-prolonging interventions with comfort, autonomy, and realistic outcomes.
Reference: Loggers SAI et al. Evaluation of Quality of Life After Nonoperative or Operative Management of Proximal Femoral Fractures in Frail Institutionalized Patients: The FRAIL-HIP Study. JAMA Surg. 2022;157:424-434.
For more information on managing hip fractures in frail elderly patients, check out Anesthesia Updates on the NYSORA Anesthesia Manual App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.
AI On Call: Case of the Week
Patient: Female, 89 years old
History: Advanced dementia, non-verbal, bedbound in a long-term care facility
Comorbidities: Severe frailty, chronic kidney disease stage 4, malnutrition
Event: Sustained a low-impact fall, diagnosed with a displaced proximal femoral fracture
Would you recommend surgery?
The NYSORA Anesthesia Manual App recommends considering these critical factors: