Airway management in neonates and infants is a critical aspect of pediatric anesthesia and emergency medicine. Due to their unique anatomical and physiological characteristics, neonates and infants are at higher risk for adverse airway events, especially during surgery, resuscitation, and intensive care.
To address this, the ESAIC and BJA have released the first evidence-based, consensus-driven guidelines focusing specifically on this vulnerable age group (BJA, 2024). These guidelines represent a collaborative effort from 23 global experts in pediatric airway management, aiming to provide structured, clinically applicable recommendations.
Why are these guidelines important?
- High complication rates: Neonates and infants show a significantly higher incidence of difficult airway events compared to older children and adults.
- Lack of pediatric-specific equipment and training: Most airway tools and protocols have been developed for adults.
- Anatomical complexity: Large tongues, high larynx, short necks, and narrow airways complicate both visualization and intubation.
Key areas of focus
The guidelines address seven critical domains of neonatal and infant airway management:
- Preoperative assessment and preparation
- Medication use
- Intubation techniques and algorithms
- Difficult airway identification and management
- Tracheal intubation confirmation
- Safe tracheal extubation
- Human factors and training
Recommendations at a glance
Top 10 clinical recommendations:
- Use medical history and physical examination to identify difficult airways.
- Ensure adequate sedation or general anesthesia.
- Administer neuromuscular blockers if spontaneous breathing is not needed.
- Use a videolaryngoscope with an age-adapted blade as a first-line intubation technique.
- Apply apnoeic oxygenation during tracheal intubation.
- Consider supraglottic airway devices (SGAs) for failed intubation scenarios.
- Limit tracheal intubation attempts to reduce trauma and hypoxia.
- Use a stylet for hyperangulated blades or anterior larynx positions.
- Confirm intubation with clinical assessment and end-tidal CO₂ monitoring.
- Post-extubation, apply HFNO, CPAP, or NIPPV if needed.
Step-by-Step
Preoperative phase
Preoperative Airway Assessment
- Recommendation: Use the patient’s medical history and a physical exam to predict difficult airway.
- Assess for:
- Craniofacial abnormalities
- Limited mouth opening
- Cervical spine issues
- Be especially vigilant in patients with airway-challenging syndromes such as:
Pharmacological Preparation
- Adequate sedation or general anesthesia is essential.
- Neuromuscular Blocking Agents (NMBAs) are recommended unless spontaneous breathing is required.
- These improve intubation success and reduce risk of laryngospasm.
- Rocuronium, at a dose of ~0.2 mg/kg, is effective in improving first-pass success.
Intraoperative phase
Tracheal Intubation Techniques
- Videolaryngoscopy (VL) is the preferred first-choice technique:
- Improves glottic view and success rate.
- Ideal for training and use in OR, ICU, or ED.
- Apneic oxygenation is recommended during intubation to prevent desaturation.
Difficult Airway Management
Anticipated Difficult Airway:
- Have the following ready:
- Videolaryngoscope (VL)
- Flexible bronchoscope
- Supraglottic airway (SGA)
- Limit the number of intubation attempts.
- If failure occurs, change technique or switch operator.
Unanticipated Difficulties:
- Use a standardized algorithm or cognitive aid to guide management.
Rescue Oxygenation:
- Strongly recommend the use of SGAs if mask ventilation or intubation fails.
Confirmation of Tracheal Intubation
Primary Methods:
- Bilateral chest auscultation
- End-tidal CO₂ waveform
Supplementary Tools:
- Videolaryngoscopy or ultrasonography for confirmation
Tube Placement Confirmation:
- Chest X-ray is the gold standard.
- Ultrasound is increasingly popular for real-time verification.
Postoperative phase
Post-Extubation Strategies
Respiratory Support Options:
- High-Flow Nasal Oxygen (HFNO)
- Continuous Positive Airway Pressure (CPAP)
- Nasal Intermittent Positive Pressure Ventilation (NIPPV)
Extubation Timing
- Awake Extubation: Preferred in high-risk patients to minimize complications such as laryngospasm.
- Deep Extubation: Should only be performed by experienced providers with immediate reintubation capabilities.
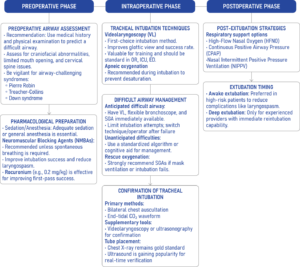
Airway management algorithm for neonates and infants.
Human factors and training
Effective airway management isn’t just technical—it’s cognitive and collaborative. Errors are often linked to:
- Inexperience
- Communication breakdowns
- Fixation errors (e.g., focusing solely on intubation instead of oxygenation)
Training recommendations:
- Establish a pediatric airway curriculum
- Use simulation-based training regularly
- Encourage multidisciplinary team debriefs after complex cases.
Special considerations
Difficult airway equipment checklist:
- Multiple videolaryngoscope types
- Supraglottic airway devices (SGA)
- Flexible and rigid bronchoscopes
- Stylets and bougies
Emergency surgical access:
- Cricothyrotomy is contraindicated in neonates.
- Surgical tracheostomy is the preferred life-saving airway access.
- ECMO may be considered in extreme scenarios.
Conclusion
The 2024 guidelines mark a significant advancement in the field of pediatric airway management. By tailoring strategies to neonates and infants, and emphasizing training, safety, and multidisciplinary teamwork, these guidelines provide a robust foundation for improved clinical outcomes.
Hospitals, training programs, and clinicians are encouraged to adapt and integrate these guidelines into their local protocols and curricula. The health and safety of our smallest patients depend on it.
For more information, refer to the full article in BJA.
Disma N et al. Airway management in neonates and infants: European Society of Anaesthesiology and Intensive Care and British Journal of Anaesthesia joint guidelines. Br J Anaesth. 2024;132:124-144.
Learn more about neonatal airway management in NYSORA’s Airway management updates!