Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About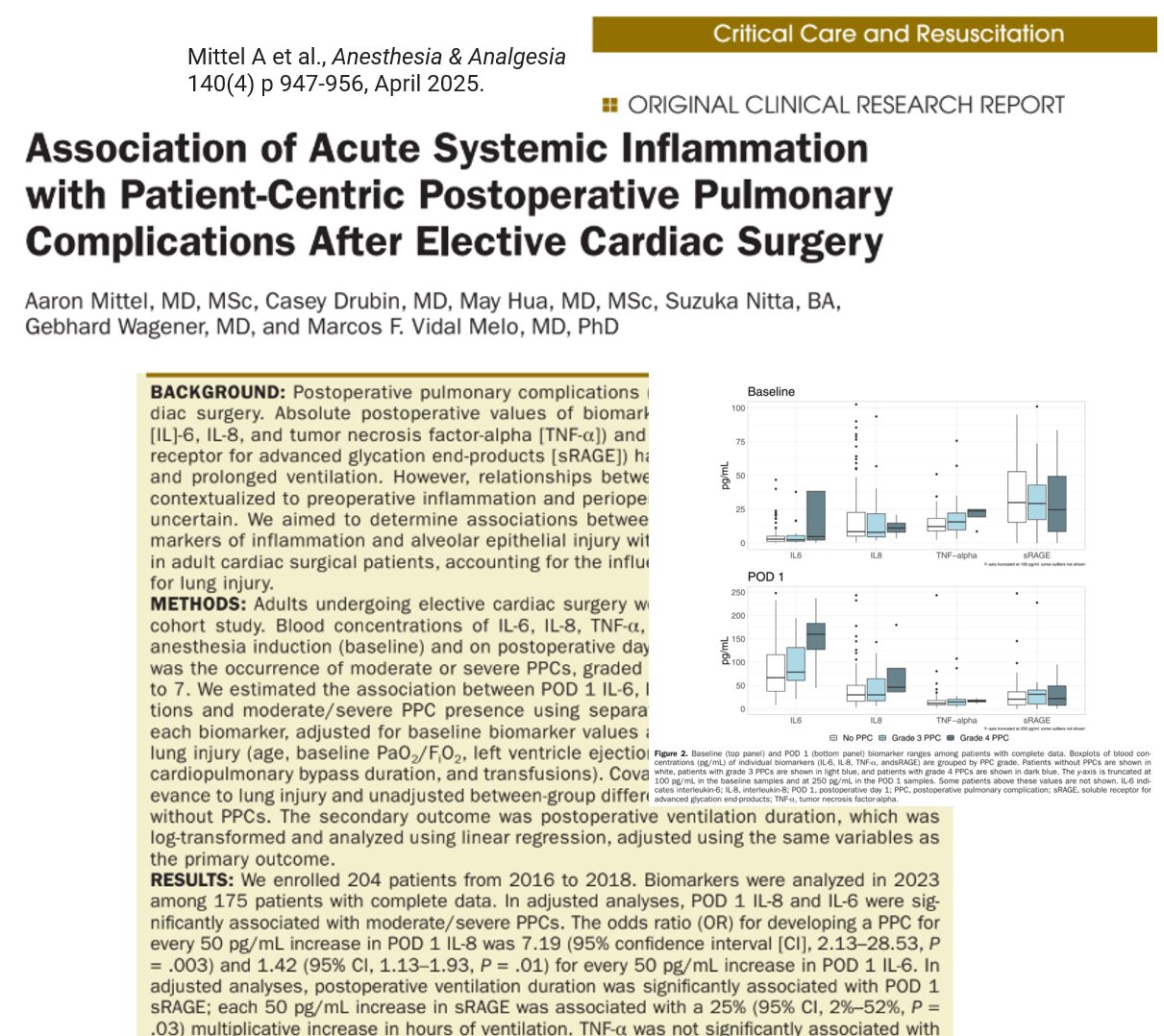
A groundbreaking study published in the April 2025 issue of Anesthesia & Analgesia reveals compelling evidence that acute systemic inflammation after elective cardiac surgery significantly increases the risk of postoperative pulmonary complications (PPCs). Conducted at Columbia University Irving Medical Center, this large-scale observational study offers new perspectives on how cytokine activity and lung epithelial injury biomarkers can predict respiratory outcomes after surgery.
Background
Postoperative pulmonary complications are a leading cause of morbidity following cardiac surgery. These include:
- Pneumonia
- Pleural effusions requiring drainage
- Reintubation or prolonged mechanical ventilation
- Use of noninvasive respiratory support (BiPAP, HFNC)
Despite their frequency, effective predictors and interventions remain elusive.
Key research question:
Can increases in inflammation-related biomarkers post-surgery predict the likelihood of PPCs, when accounting for preoperative conditions and surgical factors?
Methods in brief
Biomarkers measured:
- IL-6 (Interleukin-6)
- IL-8 (Interleukin-8)
- TNF-α (Tumor Necrosis Factor-alpha)
- sRAGE (Soluble Receptor for Advanced Glycation End-products)
Timing of measurements:
- Baseline – After anesthesia induction, before surgery
- POD 1 – Postoperative Day 1 (18–24 hours after surgery start)
Complication assessment:
- Used a graded PPC scale from 0 to 5
- Focused on moderate (Grade 3) and severe (Grade 4) complications
Major findings
-
Inflammatory cytokines and PPC risk
The study found that elevated levels of inflammatory cytokines on postoperative day 1 (POD 1), particularly IL-6 and IL-8, were significantly associated with an increased risk of moderate-to-severe PPCs. For every 50 pg/mL increase in IL-8, the odds of developing a PPC rose more than sevenfold. Similarly, a 50 pg/mL increase in IL-6 was linked to a 42% higher risk. In contrast, TNF-α and sRAGE levels were not significantly associated with PPC risk. These findings suggest that IL-6 and IL-8 are strong independent predictors of PPCs, even after controlling for patients’ baseline inflammatory status and perioperative variables.
-
sRAGE and ventilation duration
- Every 50 pg/mL increase in sRAGE was linked to a 25% increase in mechanical ventilation time.
- IL-6, IL-8, and TNF-α did not significantly correlate with ventilation time.
Clinical relevance
This study underscores that:
- Post-CPB inflammation, especially increases in IL-6 and IL-8, may directly contribute to PPCs.
- Alveolar epithelial damage, as indicated by sRAGE, prolongs the need for ventilation.
These biomarkers could guide early risk stratification and personalized interventions post-cardiac surgery.
Implications for future practice
- These findings open the door to targeted anti-inflammatory therapies post-surgery.
- IL-6 and IL-8 could become routine postoperative biomarkers in high-risk cardiac surgery patients.
- sRAGE may help forecast patients who will need prolonged ventilatory support.
Reference: Mittel A et al., Association of Acute Systemic Inflammation with Patient-Centric Postoperative Pulmonary Complications After Elective Cardiac Surgery, Anesthesia & Analgesia, 2025;140:947-956.
For more information on inflammation and postoperative complications, check out Anesthesia Updates on the NYSORA Anesthesia Assistant App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.