Median sternotomy remains the primary access for cardiac surgery, but it comes at a price: intense anterior chest pain that can limit coughing, deep breathing, and early mobilization. Up to half of patients report severe sternal pain at rest and nearly 80% during coughing on postoperative day 1. Uncontrolled pain is not just uncomfortable—it impairs respiratory mechanics, slows recovery, and may contribute to chronic sternal pain months later.
Multimodal, opioid-sparing strategies are now standard in enhanced recovery pathways, but systemic adjuncts such as NSAIDs, gabapentinoids, and dexmedetomidine carry hemodynamic, renal, or neurocognitive baggage that is especially relevant in cardiac patients. Fascial plane blocks have therefore gained traction as a low-risk way to target sternotomy pain directly.
Superficial parasternal intercostal plane (SPIP) blocks target the anterior cutaneous branches of T2–T6 and have been shown to reduce acute post-sternotomy pain. Single-injection SPIP is simple, superficial, and generally safe—but limited by duration, while sternotomy pain often persists for 48 hours or longer. Catheter-based continuous SPIP seems like the logical “next step”: prolong the block, smooth the pain curve, and potentially improve recovery and reduce opioids.
Whether that extra complexity and resource use actually translates into better patient outcomes has remained unclear. This randomized controlled trial tested whether continuous SPIP infusion via parasternal catheters provides superior sternal pain relief at 24 hours compared with single-injection SPIP alone in patients undergoing cardiac surgery with full median sternotomy.
Study objective and methods
The primary objective was to determine whether a continuous SPIP block reduces sternal pain on coughing at 24 hours after sternotomy compared with a single-injection SPIP.
- Design: Single-center, randomized, parallel-arm, double-blind, superiority trial.
- Setting: Tertiary academic cardiac center, Vancouver, Canada.
- Population: 80 English-speaking adults undergoing scheduled cardiac surgery via full median sternotomy.
- Exclusions included: Emergency surgery, significant coagulopathy, major organ failure, opioid tolerance, weight < 60 kg, anticipated therapeutic anticoagulation within 48 h, and technical barriers to catheter placement.
- Interventions (both groups):
- Bilateral SPIP catheters placed within 4 h of ICU admission under ultrasound guidance (T6 → T2 parasternal trajectory).
- Initial bolus: 20 mL 0.2% ropivacaine through each catheter (total 40 mL) – effectively a single SPIP block for all patients.
- Continuous infusion for 48 h at 3 mL/h per catheter of:
- Intervention group: 0.2% ropivacaine.
- Control group: Normal saline.
All patients received standardized multimodal analgesia with scheduled acetaminophen and IV hydromorphone (PCA after extubation); other adjuncts (NSAIDs, gabapentinoids, etc.) could be added as clinically indicated.
Outcomes
- Primary outcome: NRS (0–10) sternal pain during standardized coughing at 24 h after “time zero” (initial catheter bolus).
- Secondary outcomes: NRS sternal pain (rest and coughing) from 8–48 h; cumulative opioid consumption (oral morphine equivalents) at 0–24 h and 24–48 h; QoR-15 at 48 h; nausea/vomiting within 48 h; chronic sternal pain at 3 months; and safety outcomes including suspected or confirmed LAST, infection, resternotomy, reintubation, delirium, and death.
Key findings
-
No reduction in cough pain at 24 hours
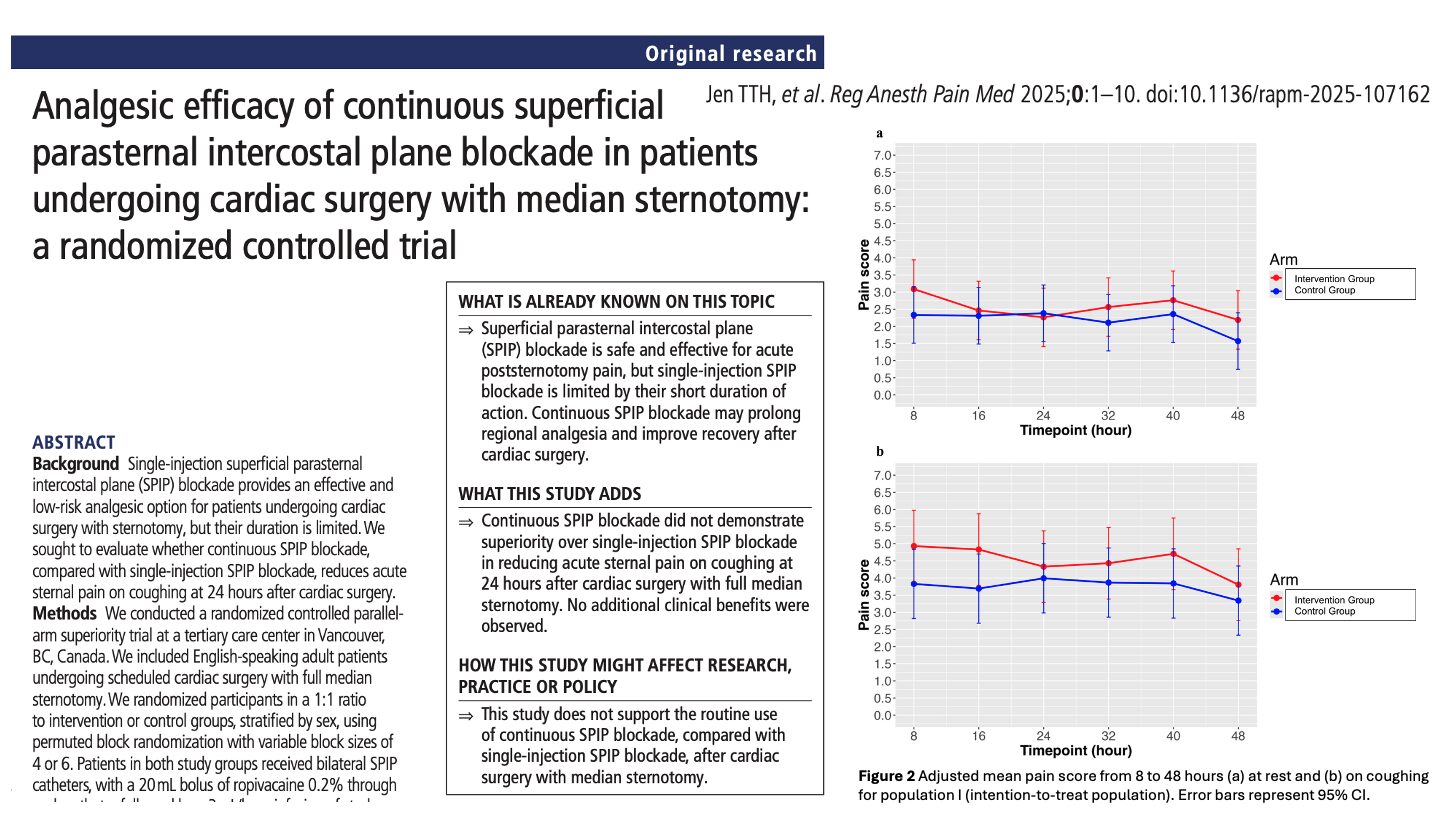
Continuous SPIP infusion did not improve sternal pain during coughing—the primary endpoint. Pain scores were nearly identical between groups at 24 hours (4.0 vs 3.9), and the adjusted mean difference showed no clinically or statistically meaningful benefit. This indicates that extending analgesia via continuous infusion did not improve the effect already provided by the initial SPIP bolus.
-
Pain trajectories over 48 hours remained unchanged
Pain assessments from 8 to 48 hours, both at rest and with coughing, showed no advantage for the continuous-infusion group. Mixed-effects modeling and AUC analysis confirmed that overall pain burden was similar between groups. The continuous SPIP block did not modify the pattern, severity, or duration of postoperative sternal pain.
-
Opioid use and recovery metrics were not improved
Cumulative opioid consumption at 24 and 48 hours did not differ between groups, and key recovery measures—including incidence of nausea/vomiting, QoR-15 scores, and chronic pain at 3 months—were also similar. The absence of opioid-sparing or recovery-enhancing effects suggests that continuous SPIP did not offer any additional functional benefit.
-
Safety outcomes showed no meaningful advantage
Although complication rates were low and similar between groups, one suspected case of local anesthetic systemic toxicity occurred in the continuous-infusion arm. No reduction in wound issues or other postoperative complications was observed. Given no measurable clinical benefit, any added procedural or safety risk may be harder to justify.
-
The initial SPIP bolus likely provided sufficient analgesia
Both groups received the same 40 mL ropivacaine bolus before infusion, and the prolonged effect—potentially enhanced by routine dexamethasone use—may have covered the critical first 24 hours. This likely minimized any difference between groups and suggests that the single-injection SPIP alone provides adequate sternotomy analgesia in most patients.
Conclusion
In adults undergoing cardiac surgery via full median sternotomy, adding 48-hour continuous SPIP infusion through parasternal catheters did not reduce sternal pain on coughing at 24 hours compared with a single-injection SPIP block, nor did it improve opioid use, QoR, PONV, or chronic pain. With one suspected case of LAST and no clinical upside, the study does not support routine continuous SPIP catheter use in this setting.
For most patients in a modern, multimodal pathway, a well-executed single-injection SPIP appears to be sufficient.
Future research
- Optimize infusion strategies: Test higher-volume or programmed intermittent bolus regimens (balanced against LA toxicity risk), possibly with plasma level monitoring.
- Refine patient selection: Identify phenotypes (very high pain burden, limited systemic analgesic options, complex re-ops) who might genuinely benefit from catheters.
- Map pain generators: Better disentangle the relative contribution of sternum, pleura, IM harvest, and drains—and tailor blocks accordingly.
- Compare regional “packages”: SPIP alone vs PIFB, vs combinations (e.g., SPIP + parasternal or rectus sheath) with hard outcomes like mobilization milestones, pulmonary complications, and chronic pain.
Clinical implications
For centers already performing SPIP blocks as part of ERAS-style cardiac pathways, this trial suggests that routine continuous SPIP catheters are unlikely to provide added value over a single-injection block plus multimodal systemic analgesia.
Catheters demand extra time, hardware, dressing care, and safety vigilance (infection, dislodgement, LAST) without demonstrated improvements in pain, opioids, or recovery in this context. The results support a simplified approach:
- Make single-injection SPIP high-quality and consistent.
- Layer in non-opioid systemic analgesia.
- Reserve more complex catheter strategies for carefully selected situations rather than default use.
Clinical pearls
- Single-injection SPIP already provides effective sternotomy analgesia when combined with multimodal care.
- Continuous SPIP infusion (0.2% ropivacaine at 3 mL/h per side) did not lower cough pain at 24 h.
- No differences in opioids, QoR-15, PONV, or chronic sternal pain were seen.
- One suspected LAST case highlights that catheters do increase systemic LA exposure.
Practical tip: For most median sternotomy cases, prioritize a well-placed single-injection SPIP, along with robust multimodal analgesia, and reserve continuous SPIP catheters for highly selected patients rather than routine use.
For more detailed information, refer to the full article in RAPM.
Jen TTH. et al. Analgesic efficacy of continuous superficial parasternal intercostal plane blockade in patients undergoing cardiac surgery with median sternotomy: a randomized controlled trial. Reg Anesth Pain Med. Published online November 5, 2025.
Download the Nerve Blocks App HERE for in-depth insights on the parasternal block. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!