Learning objectives
- Identify conditions requiring a tracheostomy
- Management of a tracheostomy
Definition and mechanism
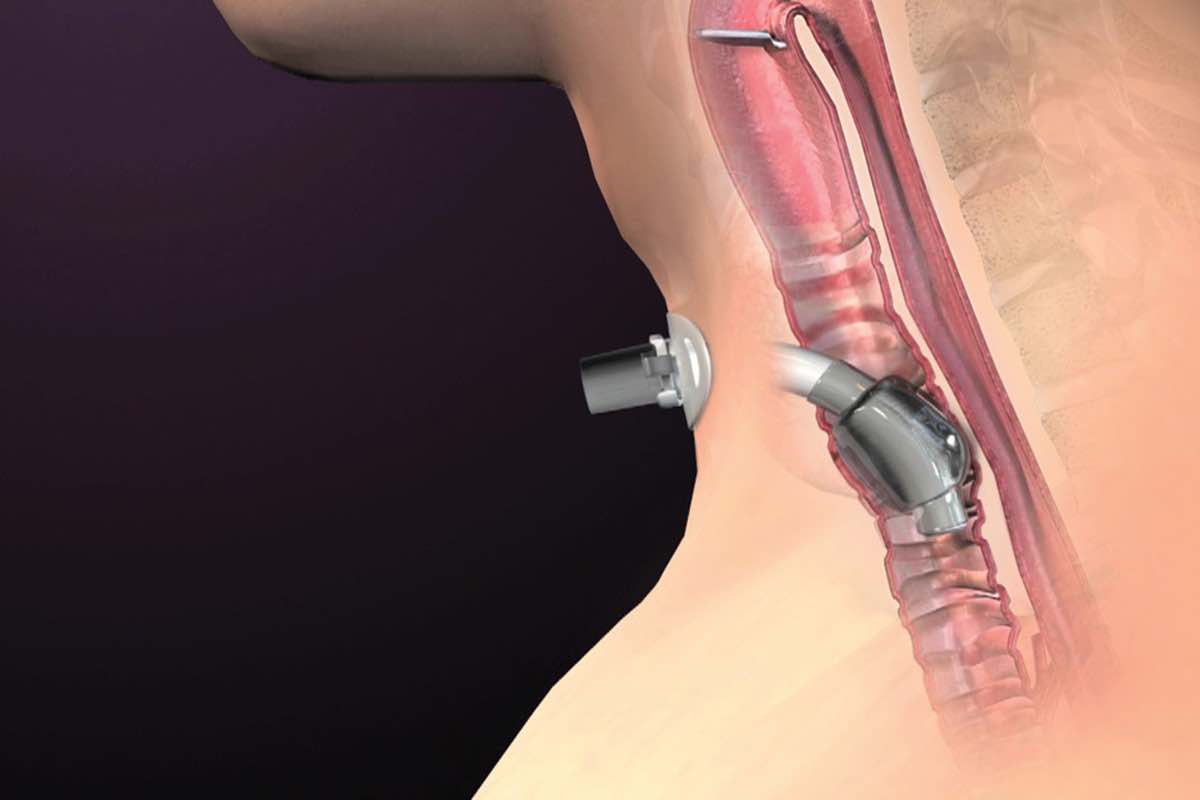
- Surgical incision into the trachea that forms a temporary or permanent opening, when intubation is expected to last > 1-2 weeks
- Very short and wide tube directly place into trachea → decreased risk of pneumonia
- Commonly performed in the OR under general anesthesia
- Create access to remove secretions from the lungs
- Often needed when health problems require long-term use of a machine (ventilator) to help you breathe
- Emergency tracheostomy is performed when the airway is suddenly blocked due to a traumatic injury to the face or neck
- Patients with a tracheostomy can be weaned from a ventilator faster than patients with a ETT
- Consider: shared airway, difficult airway
- Close communication with surgeon, backup plan discussed
Indications
- Prolonged mechanical ventilation
- Pulmonary toilet
- Airway protection
- Part of a surgical procedure
- Upper airway obstruction
- Aspiration risk
Conditions requiring a tracheostomy
- Congenital abnormalities of the airway
- Airway burns from the inhalation of corrosive material
- Obstruction of the airway by a foreign object
- Obstructive sleep apnea
- Injury to the larynx
- Severe neck or mouth injuries
- Bilateral vocal cord paralysis
- Facial burns or surgery
- Chronic lung disease
- Anaphylaxis
- Coma
- Cancers that affect the head and neck
- Infection
- Neck tumors
- Paralysis of the muscles used in swallowing
- Injury to the chest wall
- Dysfunction affecting the diaphragm
Complications
| Early | Short-term | Long-term |
|---|---|---|
| Hemorrhage | Blockage | Tracheomalacia |
| Aspiration | Tube displacement | Tracheal stenosis |
| Pneumothorax | Pneumothorax | Tracheocutaneous fistula |
| Failure of procedure | Surgical emphysema | Decannulation problems |
| Infection | ||
| Delayed hemorrhage | ||
| Tracheal necrosis | ||
| Tracheo-arterial fistula |
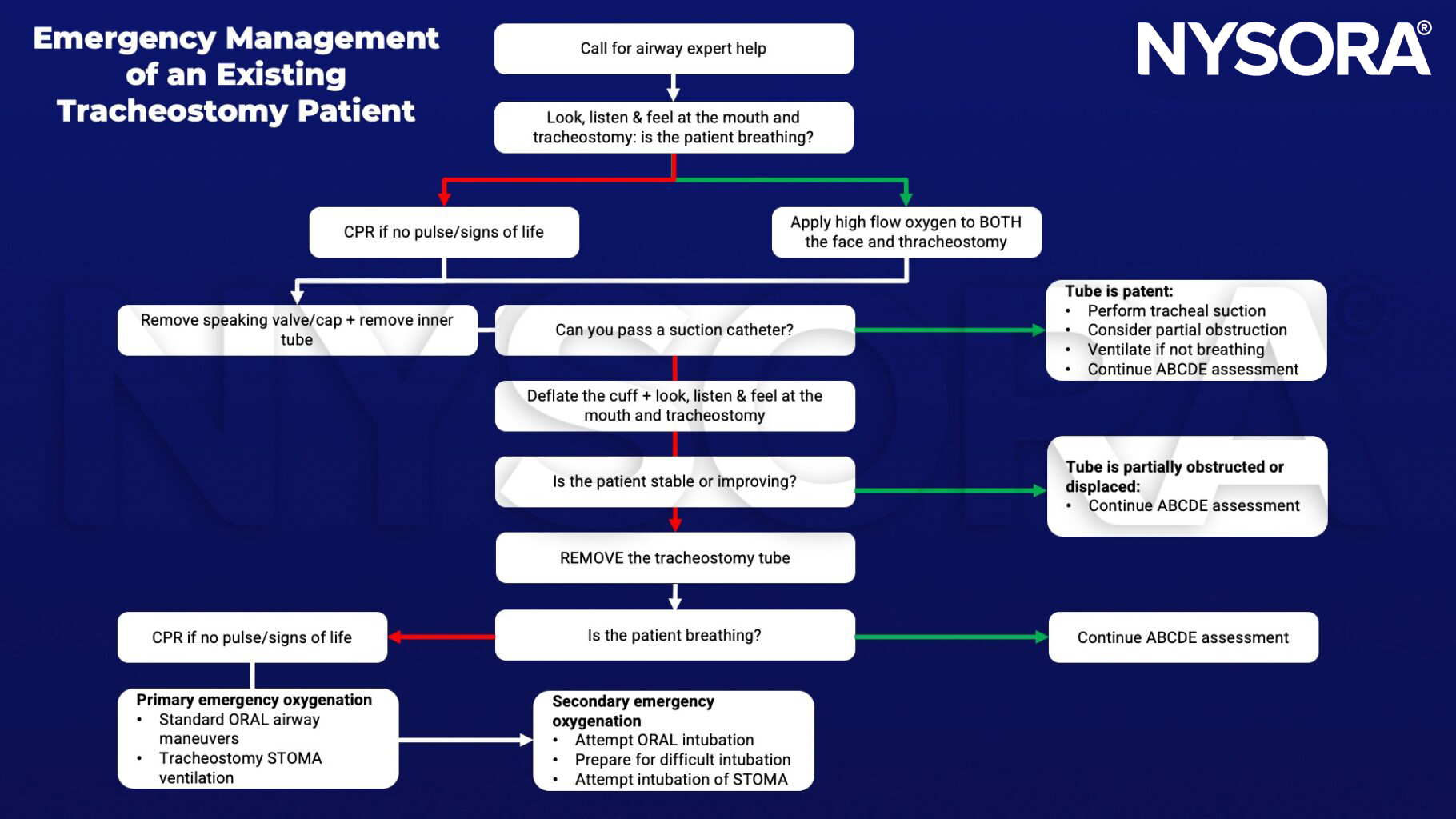
Management
- High-flow nasal oxygen therapy to slow the time to desaturation where intubation or face-mask ventilation is difficult/impossible
- Risk on fire as FiO2 is close to 1.0 if diathermy is used
- Check the position and size of the tracheostomy tube with a combination of capnography + endoscopy + cuff pressure
- The tube is too short: the cuff may herniate up into the superior larynx (within the vocal cords) thereby causing reduced pulmonary compliance, persistent cuff leaks, or tracheal damage
- Tube too long: risk of endobronchial tube placement
Keep in mind
- A laryngectomy tube can be used instead of a tracheostomy tube for intraoperative ventilation of the lungs during surgery
- Difficult BMV & supraglottic device ventilation (air leak)
- Dangerous placement of ETT (direct vision preferred)
- Comorbid disease:
- ICU patient with multi-organ failure, sepsis, lung injury, etc
- Neuromuscular disorders, chronic high spinal cord injury
- Ensure emergency tracheostomy equipment is available: various sizes of cuffed/uncuffed tracheostomy tubes, suction catheters, graspers, Ambu bags & ties
Suggested reading
- Rosero EB, Corbett J, Mau T, Joshi GP. Intraoperative Airway Management Considerations for Adult Patients Presenting With Tracheostomy: A Narrative Review. Anesth Analg. 2021;132(4):1003-1011.
- Lewith H, Athanassoglou V. Update on management of tracheostomy. BJA Educ. 2019;19(11):370-376.
Clinical updates
Kristensen et al. (Current Opinion in Anesthesiology, 2025) highlight that head and neck surgical patients have a significantly increased risk of airway compromise, with tracheostomy often required either electively or emergently. The review emphasizes early identification of patients at high risk for airway obstruction and recommends considering planned awake tracheostomy under local anesthesia in selected cases rather than risking failed intubation after induction. Clear criteria for front-of-neck access (eFONA) must also be part of every airway plan. Importantly, the authors stress multidisciplinary preoperative planning and structured postoperative airway management, as airway edema and bleeding may necessitate delayed extubation or conversion to tracheostomy.
- Read more about this study HERE.
Granell Gil et al. (Current Opinion in Anaesthesiology, 2026) highlight updated EACTAIC thoracic guidelines emphasizing tailored airway strategies in patients with altered tracheobronchial anatomy, including those with existing tracheostomies. In such patients, bronchial blockers are preferred over double-lumen tubes to facilitate lung isolation while minimizing airway trauma and accommodating distorted anatomy. For tracheostomy patients undergoing thoracic surgery, individualized planning and device selection are key to ensuring effective one-lung ventilation and reducing perioperative airway complications.
- Read more about this study HERE.