
In workshops, the lung sliding of healthy models is rather easy to study. In the critically ill, because either exacerbated but parasited by severe dyspneas or made too subtle by deep sedations, its study needs the consideration of adapted signs.
The normal lung surface is defined by the association of A-lines and lung sliding. At the anterior chest wall in a supine patient, this is the A-profile. Detecting lung sliding is the first step of the BLUE-protocol. Lung sliding is a physiological phenomenon that anyone can easily detect using appropriate tools. In the critically ill, because either dyspneic or ventilated, different phenomena occur. For describing them scientifically, several points must be specified, and this deserves a full chapter. Like any vital organ, the lung moves from our birth to our death without interruption. Lung sliding is a kind of dynamic (sparkling, twinkling, glittering, shimmering, and “ant’s walk” are suitable terms too) arising from the pleural line. The pleural line is built by two layers: the parietal pleura, always motionless, and the visceral pleura, only when the lung is at the chest wall, moving or not. The sliding of the visceral pleura against the parietal pleura creates this sparkling at the pleural line. Lung sliding indicates that, first, the lung is at the chest wall and, second, this lung works. “Lung sliding” is a euphonic locution; read Anecdotal note 1. Our 5 MHz micro convex probe is ideal for this part of lung investigation. Using our technique (which can be summarized as withdrawing any kind of filter), it makes a work similar (if not superior) to the usual vascular probes advocated by some.
1. LUNG SLIDING: A NEW SIGN, A NEW ENTITY IN THE RESPIRATORY SEMIOLOGY
Lung sliding indicates a physiological reality, the descent of the lung toward the abdomen. Is it a valuable sign? How to assess it? Not clinically of course; we don’t benefit from any specific sign from the father of lung semiology [1] . So with what? Fluoroscopy? It is a too imperfect tool. Lung sliding should be considered as a new sign which speaks for itself and does not need any gold standard. Those who denied the reality of lung ultrasound were maybe in lack of a gold standard [2]. Some would have appreciated a tool allowing to better understand the lung physiology [3].
Since when is ultrasound able to detect this fine movement? From our eyes, since at least 1982, but it is obvious that the antique, pantographic systems of the 1960s were able to demonstrate this dynamic, using M-mode.
2. NORMAL LUNG SLIDING IN THE HEALTHY SUBJECT, A RELATIVE DYNAMIC: THE SEASHORE SIGN
The lung works like a craniocaudal piston. Lung sliding is more easy to detect using longitudinal scans; this is one of the reasons why we advise them. We now define lung sliding as a homogeneous sparkling of the whole of the Merlin’s space, i.e., beginning at the very pleural line, not one mm above, not one mm below. This dynamic is relative, a critical notion since a diffuse dynamic of the whole image is unavoidable. First, the patient as well as the doctor are still alive, both generating minute movements. Second, there is a minute background noise. Yet these dynamics are diffuse, whereas lung sliding begins at the very pleural line. The M-mode appears to be insensitive to the background noise; this is why it displays a sandy pattern exactly at and below the pleural line. We called this pattern the seashore sign (Fig. 1). The use of the M-mode perfectly highlights the relativity between lung sliding and motionless wall.
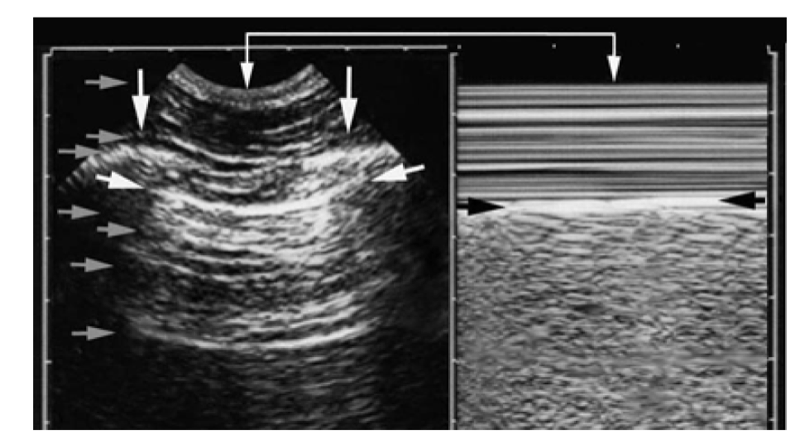
Fig. 1 The seashore sign. The present figure is crowded with arrows. Left, real-time image. The simple (isolated) vertical arrows show the ribs. The white horizontal arrows show the pleural line, clearly defined by the bat sign. Gray horizontal arrows show some of the numerous horizontal lines which should not be confused with the pleural line. They indicate, from top to bottom, the skin, some aponeuroses, a rib, minor air reflections below the pleural line called sub-A-lines and ( lower gray arrow ) an A-line. Right: M-mode. A marked change appears between Keye’s space, here “quiet” above the black arrows, and the space below, called M-Merlin’s space or again MM-space. The black arrows indicate precisely the pleural line, with no space for confusion. Look at the upper coupled, vertical white arrows, indicating how finely real-time and M-mode are tuned together: this allows the immediate location of the pleural line in any circumstance, a critical point in extreme emergencies. Keye’s space displays something like quiet waves. The space below (MM-space) shows a homogeneous, sandy pattern, generated by the lung when sliding against the chest wall. This is the seashore sign. No need for video, this figure allows to identify a lung sliding without any confusion.
The M-mode is useful for understanding lung sliding. The whole of Merlin’s space twinkles, creating this seashore sign. The physicians able to interpret a posteriori a frozen M-mode image prove that they master lung ultrasound. They won’t need videos. Yet one point is of prime importance: the operator’s eye should recognize lung sliding through a real-time image before using M-mode. This must be a habit. One main reason is explained in the SESAME-protocol (cardiac arrest), where there is no time for starting the M-mode.
The M-mode is practical for data recording; it is easier to insert an image in a medical file. In the LUCIFLR project, one image is taken after any thoracic procedure and must show the bat sign at the left, the seashore sign at the right, and a mention where it was taken (e.g., upper BLUE-point, supine patient): this replaces (to advantage!) the chest radiography
Lung sliding is suppressed by many conditions. Apart from them, it is present in eupnea and dyspnea, in spontaneous as well as conventional mechanical ventilation. It is visible in skinny and bariatric patients. It is present in bronchial emphysema. In giant emphysema bulla, in our observations, a minute lung sliding (or equivalents, see below) is usually detected. Lung sliding is visible at any age, from the first second of extrauterine life to the dying breath.
3. LUNG SLIDING, ALSO A SUBTLE SIGN WHICH CAN BE DESTROYED BY INAPPROPRIATE FILTERS OR SO-CALLED FACILITIES. THE IMPORTANCE OF MASTERING DYNAMICS AND BYPASSING THESE FACILITIES
Simple clues will optimize the analysis of lung sliding. We face a dynamic feature. Therefore, the physician must control the dynamic dimension, i.e., suppressing, or understanding, all other dynamics.
A dynamic coming from the physician must be suppressed by any means. Only the patient is allowed to move. The operator’s hand must be fully standstill (Fig. 2).
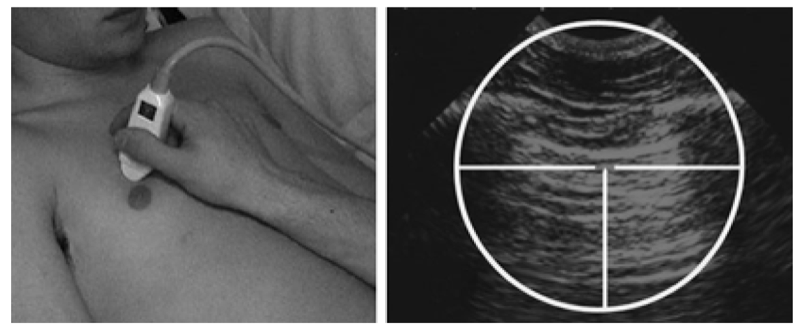
Fig. 2 Mastery of dynamics. As far as possible (setting permitting), the hand of the operator must be completely motionless and be able to wait for hours, without moving and without fatigue, like a sniper. Nonsteady hand is a key for failure. Only the patient is expected to move.
- Our small microconvex probe, easy to handle like a pen, favors this standstillness. Ecolight is a non-slippery product, and energy devoted for keeping the probe stable is spared. Once the operator gets the best image of the bat sign, he/she stops any movement and “quietly” watches at the pleural line, like a sniper.
- A dynamic impaired by filters must be recognized by any means, and these filters must be suppressed. All factors making lung ultrasound more difficult must be destroyed. The problem is simple: they have conceived sophisticated programs which slightly improve tissular imaging (a minor benefit for us) and deeply worsen lung imaging, the most critical. See the sections below, widely dealing with this issue.
- A dynamic created by the critically ill patient, either exacerbated by dyspnea or decreased by mechanical ventilation. This dynamic cannot be suppressed; one must work with it. It will generate difficulties. These difficulties will be mastered. This also deserves a special section.
4. THE VARIOUS DEGREES OF LUNG SLIDING, CONSIDERING CARICATURALLY OPPOSED STATES
Lung sliding is naturally weaker at the apex, a kind of starting block. Lung sliding is naturally weaker in quiet ventilation. We can therefore imagine two situations: Studying the lower BLUE-point of a hyperventilating, dyspneic patient will show a frank lung sliding but associated with parasite noise. Studying the upper BLUE-point of a deeply sedated patient will not show any parasite dynamic but will show an extremely weak lung sliding. Note: one can be very dyspneic on mechanical ventilation. For mastering lung sliding in these extreme, but daily, situations, we should master the real time/M-mode harmony, as well as all filters. This proves highly useful when there is too much dynamic or not enough dynamic. For making all this clear, we will ask a healthy volunteer to show us various degrees of breathing. These experiments will be done just for simplifying the concept, but the whole of the observations can be found in our critically ill patients.
5. LUNG SLIDING IN THE DYSPNEIC PATIENT. THE MAXIMAL TYPE. CRITICAL NOTIONS REGARDING THE MASTERY OF THE B/M-MODE
A severe dyspnea generates uncontrolled movements of the patient, at the highest degree of anxiety. This patient tries to survive by any means, futile such as opening the window, useful such as recruiting the accessory respiratory muscles.
Observing the fine dynamic of lung sliding in such a “messy” environment may appear challenging, an equivalent of shooting from a mobile point toward a mobile target, obeying to the hectic rules of dogfights. All patients of the BLUE- protocol had a severe dyspnea, generating a parasite dynamic above the pleural line that we called muscular sliding on real-time. Users may be unable to locate whether the dynamic comes from the pleural line or above. Here, the M-mode has a critical relevance. The rules of lung ultrasound make no space for approximation: a “sand” arising above the pleural line, even a few mm above, does not come from the lung. Any sandy phenomenon which arises above the pleural line cannot be labeled a “seashore sign.”
6. DYSPNEA AND THE KEYES’ SIGN
Take our healthy volunteer and lock him up in a confined room. You create a “pure” dyspnea (on healthy lungs) which gradually worsens (Technical note 1). Then analyze the lower BLUE-point or more caudal, where lung amplitude is maximal. Such a dyspnea will create two conflicting dynamics (apart from the body agitation due to uncontrolled anxiety).
A. The dyspnea creates an increase of the tidal volume. The amplitude of lung sliding is increased, resulting in a marked seashore sign.
B. The dyspnea recruits accessory muscles. This generates perturbations above the pleural line. The real-time (bat sign) locates the pleural line in any circumstances, allowing to define Keye’s space on M-mode. A Keye space full of accidents instead of the regular stratified image has the meaning of a severe dyspnea and was coined Keye’s sign Keyes’ sign describes with no space for confusion these parasite dynamic phenomena occurring above the pleural line. And now, we have all elements for defining the seashore sign. The seashore must arise from the pleural line, always, i.e., the lower limit of Keye’s space (defined using real-time first, reminder).
For recognizing a lung sliding within Keye’s sign and getting rid of any trouble, we use several successive approaches.
1. The first to do is to focus on the real-time image. Some patterns are disturbing when seen only on M-mode, especially when there is a permanent Keye’s sand (we called them the Nogu-Armandariz sign, from spanish Ceurfers), but can be much easier to analyze on real-time, allowing often to distinguish the muscular sliding from the lung sliding. Think “M like Moderate.”
2. If the first approach does not work, sometimes muscular sliding and lung sliding are not perfectly synchronized. This makes transitory but sufficient instants where the seashore sign can be recognized, distinct from stratospheric pattern above. These subtle signs remind how ventricular tachycardia is diagnosed (Anecdotal note 2).
3. If the first two approaches do not work, we use a sign not yet labeled. It requires full understanding of Keye’s space. When the column of sand from above the pleural line (the dyspnea) undergoes a change, even slight, when crossing the pleural line, it is possible to affirm that lung sliding is present (Fig. 3).

Fig. 3 Dyspnea and Keye’s sign. Left, real-time. The black arrow shows an intermuscular aponeurosis. The white arrow shows the pleural line. R, shadow of ribs. Right, M-mode. This image may appear as a stormy sea. The muscular contraction (indicating major dyspnea) has generated a sandy pattern beginning ( from top ) at the area of the black horizontal arrow, i.e., above the pleural line. Is this dyspnea due to a pneumothorax? The vertical white arrows (inserted at a distance of the event) clearly display an area of typical seashore sign with a short zone of preserved Keye’s space. This is sufficient. The diagnosis of pneumothorax can be excluded. This 55-year-old lady suffered from a severe asthma. The location of the real-time and M-mode images at the same horizontal level makes easy the distinction between pleural line and muscular lines – in time-dependent settings. Would such an area not be displayed, subtle eyes may observe a fine change when the column of sand arising from the horizontal black arrow crosses the pleural line at the horizontal white arrow. Here, lung sliding has been identified as present.
Note (this can help) that the “sand” of the Keyes’ sign is a bit different from the seashore sign of lung sliding. It is stretched, not as punctiform as the genuine seashore sign.
7. CONFUSING CONFIGURATIONS
Correctly designed machines locate the real-time and M-mode images exactly side by side. Not “side by side.” Exactly side by side. Now an issue has to be known. Most laptop machines, from cheap to costly, display the M-mode with a lag when compared to the real-time image. This will prevent to locate immediately the pleural line with confidence in acute situations, when stress does not help.
We see two options. In one, the real-time image comes upstairs, small, with a large M-mode image downstairs; one must extrapolate, with haste, where the real pleural line is (Fig. 4).

Fig. 4 One configuration of M-mode. Example of a nonsuitable setting for lung ultrasound. The image quality of the upper image prevents from locating the pleural line with accuracy (cardiac probe). Since the real-time image is not located at the left of the M-mode image, the pleural line cannot be rapidly and confidently located; the user must guess or extrapolate. The “seashore” pattern comes maybe from the pleural line, maybe from a more superficial structure. Please see Fig. 5, even more pernicious. Lung sliding in a ventilated neonate.
In another, both images are displayed apparently side by side, but not exactly side by side (Fig. 5).
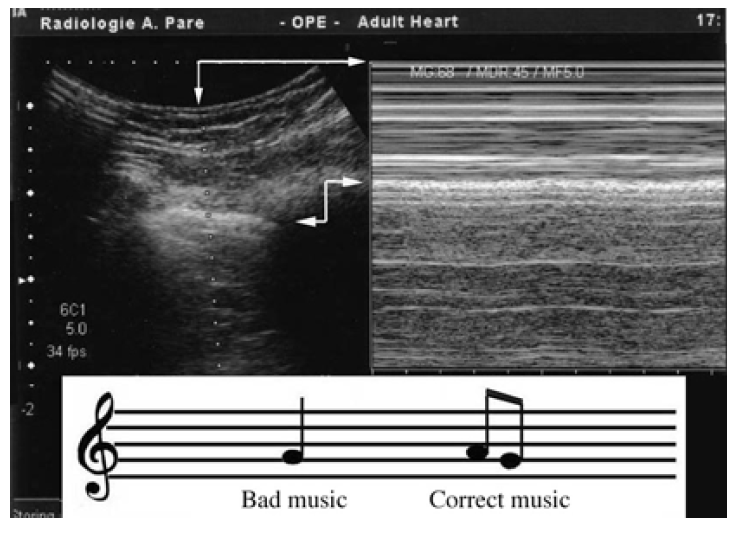
Fig. 5 M-mode and a wrong note. The arrows indicate the misconception. In very widespread machines, for unknown reasons, real time and M-mode are not exactly side by side. By bad providence, the lag corresponds to the intercostal muscle. In dyspneic patients, “sand” can be displayed from this level, i.e., above the pleural line. This will make more complex a diagnosis (pneumothorax) which asks to be, and is, simple – yet lung ultrasound does not need superimposed complexity. At the bottom is a musical score. The left note is ill defined, and the composer’s intentions are unclear. The notes at the right are perfectly defined; anyone can play them.
The perfect configuration we had in our 1982 ADR-4000 and our 1992 Hitachi 405, which both display both images exactly side by side, with no space for confusion, was not used again by the modern manufacturers, who, for incomprehensible reasons, display a gap, a lag. And nothing to rectify it. This lag corresponds roughly, bad luck, to the thickness of the intercostal muscle or more. The operator must guess the pleural line location with extreme haste (when there is no time for guesses) or, worse, risks to believe that the right image corresponds to the left one. Therefore, the unexperienced operator will think that the M-mode pleural line is this line at the level of the real-time pleural line; confusing the pleura with an aponeurosis will confuse the sand arising above the pleural line with a lung sliding, conclude “lung sliding present,” and miss the pneumothorax.
This configuration where both images are roughly but not exactly side by side is the worst. These concepts are not suitable for optimal lung ultrasound. They have been built by manufacturers unaware of the existence of lung ultrasound. This adds complexity in a field which is simple but not that simple, so let’s not add more.
This is not the last surprise. Some 2014 machines coming from self-proclaimed leaders in critical ultrasound display the M-mode at the detriment of the real time: once the M-mode is activated, the realtime image is frozen. The operator suddenly flies in the fog and loses control of lung ultrasound. One last pitfall: beginning by M-mode (first mistake) and for no reason increasing the gain. These wrong notes are easy to avoid (read Technical note 2).
8. LUNG SLIDING IN THE VENTILATED PATIENT. THE MINIMAL TYPE. CRITICAL NOTIONS REGARDING THE MASTERY OF THE FILTERS
Take our healthy volunteer out of the confined room once the first demonstration is done, and now intubate him, sedate him deeply, curarize him, and apply a low tidal volume and a low frequency. You create a quiet bradypnea. Then analyze the upper BLUE-point (or more cephalad), where the lung sliding amplitude is naturally minimal.
In these pure conditions, Keye’s space is absolutely homogeneous, without any sign of dyspnea, but lung sliding will appear very discrete and quite abolished. Lung ultrasound is a standardized field. For facing this apparent issue, we have to describe the variants of minimal lung sliding. First, understand that the slightest filter, in this setting, will completely obliterate a minimal lung sliding.
The up-to-date, sophisticated machines are rich in facilities which can deeply impair the detection of minimal lung sliding. Some have disastrous effects on this subtle dynamics. All filters must be disactivated. Take major care on this. Any filter attacking time is not compatible with critical ultrasound. The “instant response” technology was available in 1978. In most up-to-date machines, the computer works on the image before restoring it, hence an irreversible mode which creates a time lag, a destructive mode which is not compatible with a real-time discipline where every tenth of a second makes the difference for understanding the disease. Lung ultrasound requires natural images, showing the dynamic and the artifacts.
The less the filters, the easiest is lung ultrasound. The persistence filter, average filter, temporal averaging, dynamic noise filter, summation filter, etc., make lung ultrasound more difficult. Average filters give a soft image, nice to look at, at the very detriment of the dynamic. Repeat: these filters yield flattering images, which mask the true content, like a makeup. Precisely, we want to see the wrinkles. Compound, harmonics seem to be a powerful destructor of LUCI.
Now that this technical moment is over, we describe variants more or less intricated that we can also simplify in one sentence: “The slightest phenomenon arising at the pleural line and spreading below mean that the pleural line includes not only the parietal but also the visceral pleura.”
Some maneuvers can help. Sometimes, decreasing the gain makes more visible a discrete lung sliding. Sometimes, lung sliding is more visible just near the ribs than at the middle of the pleural line (the Mezire sign). Very importantly, there is an interdependency between lung sliding and lung artifacts: when Merlin’s space displays B-lines (not yet described, hence a didactic challenge), those vertical artifacts move like pendulums, and this greatly helps in detecting a minimal lung sliding. When they are absent, replaced by A-lines, the challenge is to recognize the minimal lung sliding. A-lines and B-lines are a function of the underlying disease (pulmonary edema, COPD, etc.). Mainly, the mastery of the filters and wise use of the M-mode will demonstrate the extreme variants of minimal lung sliding.
9. VARIANT 1: THE MANGROVE VARIANT
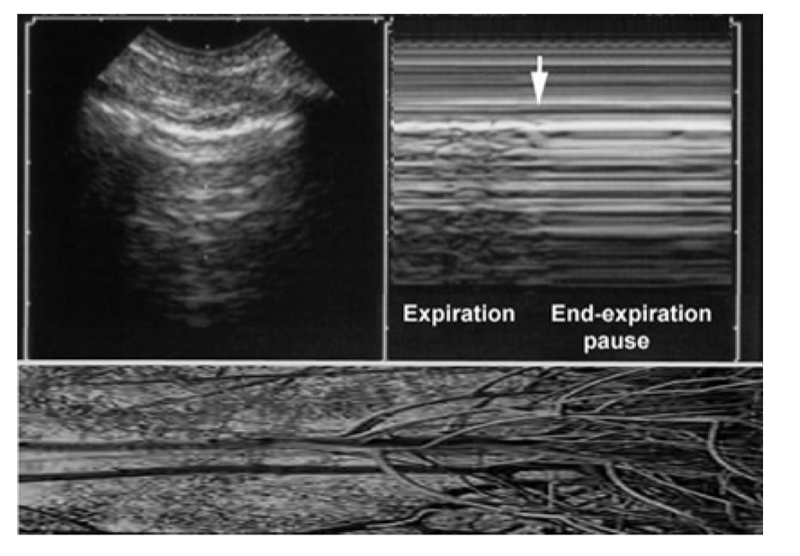
Fig. 6 The mangrove variant. Left, real-time showing a pleural line with A-lines (example here of ill-defined A-lines). Right, M-mode showing a soft interruption of the sand yielding a regular horizontal pattern at the MM-space. This interruption is progressive. This looks like aerial roots of mangrove trees (bottom image, horizontalized). The message is: don’t press the M button if not necessary.
The respiration is not a permanent dynamic; there are pauses. These physiological end-inspiratory and end-expiratory pauses are enhanced in sedated patients. These pauses generate a brief interruption (therefore, usually not seen in polypneic patients). On real-time, the lung sliding quietly stops. On M-mode, the sandy pattern of lung sliding is transiently replaced by a regular horizontal pattern evoking a “stratosphere sign” (this makes a didactic challenge, since this pattern, evoking pneumothorax. This pattern, called mangrove variant (Anecdotal note 3 ), may be confused by young users with a lung point, i.e., a main sign of pneumothorax. We must devote some lines for smashing this problem to smithereens.
1. First, the mangrove variant is a progressive phenomenon. Lung sliding is detected on real-time. It quietly comes, stops, goes, stops, comes, etc. It does not suddenly disappear (like the lung point in pneumothorax). If beginning with the real-time, there is no trouble. The mangrove variant is built by the use of M-mode. M-mode should not be used for confirming a lung sliding which has already been detected using the real-time. This is one perverse effect of an immoderate use of the M-mode.
2. Second, the lung point should be sought for only if pneumothorax is suspected, i.e., in the case of anterior absence of lung sliding associated with exclusive A-lines. The mangrove variant occurs at the entire lung surface, including the anterior parasternal areas. In other words, the only confusion should be, if any, with a limited, parasternal, clinically insignificant pneumothorax. The visualization, more laterally and on the whole lung surface, of the strictly identical pattern avoids any confusion.
10. VARIANT 2: THE PSEUDO-A’-PROFILE
This label represents a daily reality seen on normal lungs (normal lung surface, better) in deeply sedated patients. It designates an apparently abolished lung sliding, which may, if associated with A-lines, suggest pneumothorax. There is quite always one of these subtle signs, subtle but standardizable. We describe the lung pulse, the grain of sand variant, and the T-lines, which are roughly the same entity with some subtleties.
11. THE LUNG PULSE
Take again our volunteer, still deeply sedated and curarized. Give him a normal tidal volume, a normal frequency, let us analyze the left lower BLUE-point, i.e., near the heart, all conditions for improving the detection of a lung sliding. There is a cardiac activity, but it is not visible as far as it is masked by the lung activity. Now, suddenly disconnect the endotracheal tube. We can observe an immediate abolition of lung sliding, which allows the heart to express its beatings through a motionless parenchymateous cushion. This generates a kind of vibration arising from (in actual fact, stopping at) the pleural line, in rhythm with heartbeats, visible in real-time, recordable in M-mode: the lung pulse (Fig. 7).
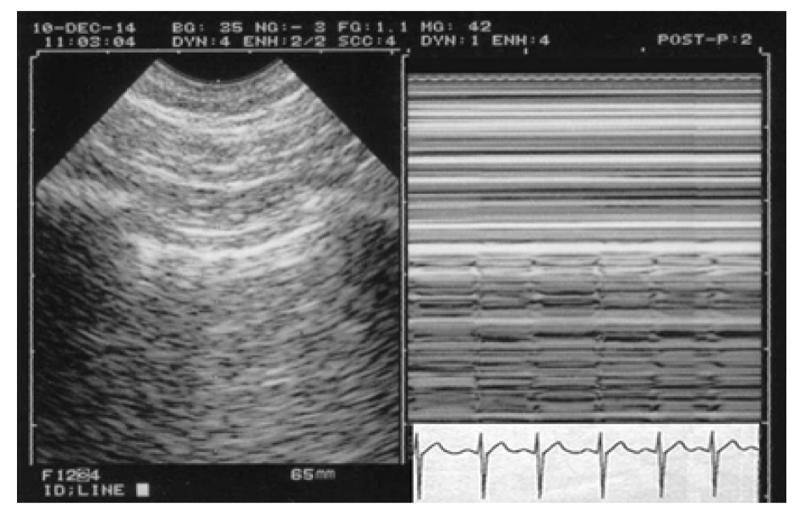
Fig. 7 The lung pulse. In this case of complete and recent atelectasis, lung sliding is abolished. Merlin’s space displays O-lines (i.e., A-lines). Pneumothorax? Impossible: vibrations in rhythm with the heart activity are seen in real time, stopping at (or arising from) the pleural line. They can be recorded in M-mode (q waves of ECG). Patient probably on mechanical ventilation (quiet Keye’s space in spite of this disorder).
The lung pulse can be discrete. It is sometimes absent, maybe (not always) when the heart is too far (right lung) or if the heartbeats are too weak. Maybe the lung pulse is a sign of good cardiac function. This variant of lung activity indicates a disease (loss of lung compliance, including atelectasis) but also an absence of disease (the visceral pleura is well attached, i.e., there is no pneumothorax). The lung pulse rules out pneumothorax. In order to simplify medicine, we can avoid the reading of long articles positioning the “lung pulse” at the end of long decision trees (lung sliding absent, then B-lines absent, then lung point absent, then lung pulse present = no pneumothorax). Please just consider that we can simply write: “lung sliding, or any equivalent such as the lung pulse” at the begin of the decision tree. The impaired lung expansion is seen mainly in complete atelectasis (including one lung intubation, foreign body aspiration, lung exclusion in thoracic surgery, etc.), acute pleural symphysis (often seen in ARDS), chronic conditions (pleural sequelae), simple apnea, and expiratory pause, a.m.o.
12. THE GRAIN OF SAND VARIANT
When lung sliding is extremely discrete, the seashore sign can be restricted to the visualization of some sand (we made previous comparisons with a termitarium). In these cases, detecting even a few grains of sand, provided they stop exactly at the pleural line, is enough for considering that the lung is at the chest wall.
13. THE T-LINE
This is an extreme variant, shaping more or less the letter “T,” starting exactly from the pleural line (Fig. 8).
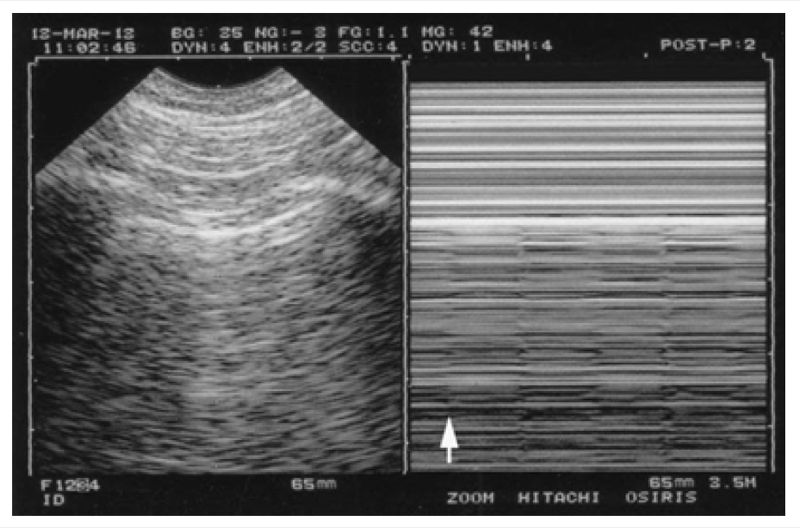
Fig. 8 An extreme variant of T-lines. An example of pseudo-A’-profile with the T-line. To the left, a short A-line. To the right, this very subtle lung activity, materialized by these T-lines (each looks like a “T”), stopping exactly at the pleural line. No pneumothorax here again. Just one arrow is inserted at the foot of the first T-line, for not spoiling this subtle image. Four T-lines are identified in the MM-space. This old patient had a large emphysematous bulla and respiratory discomfort, but the pneumothorax could be ruled out. Some antibiotics and physiotherapy solved the problem. Minor note, T-lines have nothing to do with B-lines (the T-line is an M-mode concept, the B-line a real-time image).
Following the rule expressed above, the slightest T-line rules out pneumothorax. There are probably several ways for the T-lines to be displayed (Fig. 9).

Fig. 9 A variant of lung sliding. This variant may be labeled the “bandoneon sign.” The meaning is unchanged: no pneumothorax. Note to the left (real-time) a beautiful Z-line.
14. LUNG SLIDING ABOLISHED WITH ONE OR TWO B-LINES
These B-lines are usually sufficient for demonstrating the presence of the visceral pleura against the parietal pleura. Note: with not one, not two, but three B-lines (or more), the pattern would be the “B’-profile”.
15. VARIANT 3: THE A’-PROFILE
This profile, which is also the first main sign of pneumothorax, combines complete abolition of lung sliding, complete absence of equivalents (lung pulse, T-line, etc.), and exclusive A-lines (which implies complete absence of B-line). Since medicine is medicine, in some cases, patients without pneumothorax can exhibit a genuine A’-profile. We can explain it by considering an absence of lung expansion for any reason (see above) associated with complete absence of interstitial syndrome or lung fissure and without any perception of heartbeats. One message: the A’-profile is not sufficient for the diagnosis of pneumothorax.
16. LUNG SLIDING: THREE DEGREES, BUT A DICHOTOMOUS SIGN ANYWAY
Some users complain that the familiar dichotomy which defines lung ultrasound is not respected here. It is. There are simply two levels of dichotomy (Fig. 10).
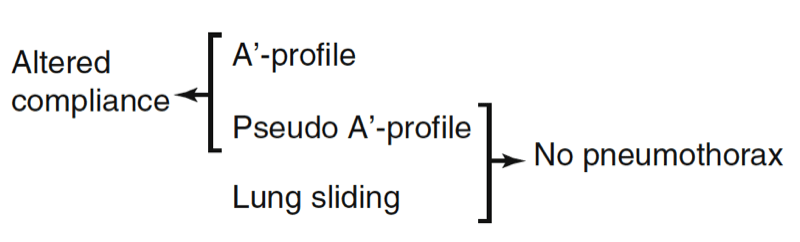
Fig. 10 Double dichotomy. The double dichotomy of lung sliding. Present or quite abolished, it rules out pneumothorax. Quite abolished or abolished, it indicates a major impairment of lung compliance.
1. When the question is “pneumothorax,” the completely abolished lung sliding is opposed to all other variants (normal lung sliding and all kinds of minimal lung sliding), which clearly rule out pneumothorax. Very discrete or abolished lung sliding makes a big clinical distinction.
2. When the question is “impaired lung compliance,” an abolished or very discrete lung sliding is pathologic, as opposed to ample lung sliding. Very discrete or abolished lung sliding make no clinical difference. Lung sliding is decreased in several processes in the critically ill, mainly ARDS.
17. CAN ONE QUANTIFY LUNG SLIDING?
Here and briefly, at the lower BLUE-point, a normal lung sliding covers the distance of the pleural line, i.e., roughly, 2 cm. One word on the B-lines (next chapters). When they are present, using our probe and its sectorial image, they move like pendulums. This phenomenon amplifies the dynamics of lung sliding. This is one of the countless advantages of our microconvex probe.
At an advanced level, the user will identify “ample lung sliding,” “weak lung sliding,” and “absent lung sliding” – as easily as distinguishing an awake person, a sleeping person, and a corpse. The real A’-profile looks like a deadly standstillness.
18. HOW ABOUT OUR HEALTHY VOLUNTEER?
We have to thank him and apologize for the hard manipulations we made on him. After that, if you have difficulties to find a next enthusiastic one willing to undergo the same delights, don’t worry: just ask any new volunteer to breathe deeper and deeper, up to recruiting accessory muscles (deep breathe through one nostril), then very slowly, then halt breathing. You reproduce all these patterns at will – and this should be done in all these workshops. Some academicians are sorry that the attendees of courses can feel a little frustrated not to see a lot of diseases there (“n’ont pas leur biscuit,” according to the French words). Healthy models can express a lot of LUCI.
19. TECHNICAL NOTES
1. Dyspnea and lung sliding
We created here a dyspnea on healthy lungs, for simplifying. Apart from pneumothorax, various diseases impair lung sliding (this is detailed through the textbook).
2. Suboptimal control of the gain
If an operator for no reason increases the gain too much and looks at the M-mode before the real-time (double mistake), the far-field will be polluted by a background noise, looking from very far like a seashore sign. This pattern, called the Peyrouset phenomenon (our fellow, who witnessed it), is not a serious pitfall:
a. The sand of the Peyrouset phenomenon is not punctiform like the seashore sign but rather micropunctiform.
b. This sand progressively fades, whereas the sandy pattern of the seashore sign stops at the very location of the pleural line.
c. The M-mode should not have a diagnostic interest except specific situations (objectifying minimal or maximal lung sliding).
It should usually be used only for keeping a document showing on paper what was actually seen on real-time. Lung sliding is detected using real-time. In no case will the Peyrouset phenomenon give the illusion of a lung sliding in a patient with a pneumothorax if one cares among others in focusing on the real-time image.
Figure 11 gives clues that allow easy distinction from a genuine seashore sign.

Fig. 11 The Peyrouset phenomenon, a side effect of excessive gain. The left image indicates the air of the ICU room – the probe is still on its stand. What is visible here is an air acoustic barrier. These roughly horizontal artifacts, called H-lines. To the right, on M-mode, the gain was (for no reason) too much increased, and a noise appears. We can see two major differences with the seashore sign. (1) The “sand” is microscopic (compare with standard seashore sign, in the white cartouche). (2) The sand density increases toward the bottom of the screen, progressively, without sudden change (whereas the seashore sign has a millimetric limit, precisely at the pleural line). To see displayed the (ill-defined) top of this parasite noise at the very level of the pleural line would really be bad luck. Don’t press the M button if not necessary.
20. ANECDOTAL NOTES
1. Euphonic note on lung sliding
Lung sliding, sliding lung is easy to pronounce (and if we may allow, rather elegant). “Pleural sliding” and “pleural gliding” are more difficult (even for native English speakers) and longer, for no advantage. The “gliding sign,” the worst, confuses with the pericardium, peritoneum, eyeball, and any muscle, all “gliding” structures. As to “seashore sign,” the term “beach” sign, sometimes heard, is maybe a little short for such a precious application, with in addition the risk of ill-defined spelling generating more trite words.
2. Note about ventricular tachycardia
The diagnosis is based on ECG on fleeting visualizations of fusion or capture complexes, quite exactly the same logic.
3. The mangrove variant
The mangrove sign was conceived during a CEURF training program in a Pacific area full of mangrove (Neo Caledonia, 2004). The stretched aerial roots of these mangrove trees were reminder of the sand of the mangrove variant.






