Learning objectives
- Describe the pathophysiology and symptoms of a subarachnoid hemorrhage
- Diagnose and clinically grade a subarachnoid hemorrhage
- Manage patients presenting with a subarachnoid hemorrhage
Background
- Subarachnoid hemorrhage account for 5% of all strokes
- Mortality rate ~50%
- One-third of survivors need lifelong care
- Prompt diagnosis and early treatment are critical
Pathophysiology
- Etiology
- Intracranial aneurysm (85% of cases)
- Arteriovenous malformations
- Trauma
- Moyamoya disease
- Risk factors
- Hypertension
- Atherosclerosis
- Cocaine use
- Alcohol abuse
- Smoking
- Connective tissue disorders
- Coarctation of the aorta
- Congenital conditions (autosomal-dominant polycystic kidney disease, Ehlers Danlos Type 4, familial intracerebral aneurysms)
- Cause
- Hemodynamically induced shear stress (sudden increase in cerebrovascular arterial pressure)
- Aneurysmal rupture leads to blood quickly traversing through the intracranial cisterns and subarachnoid space (within seconds)
- Global cerebral ischemia resulting from increased intracranial pressure, decreased cerebral perfusion, and reduced cerebral blood flow
- Intraventricular bleeding can cause acute ventricular dilatation and hydrocephalus
- Brain tissue oxygen pressure and pH are reduced
- Compensatory hypertension occurs within minutes to hours
- Blood-brain barrier disruption, cerebral edema, and a thromboinflammatory cascade
Signs & symptoms
- Sudden onset of “worst headache of life”
- Loss of consciousness
- Nausea and/or vomiting
- Nuchal rigidity
- Photophobia
- Seizures
- Comatose and hypertensive at presentation
Diagnosis
- Non-contrast cranial CT
- Lumbar puncture in patients with a high index of suspicion and a normal CT scan (red blood cell count, bilirubin level, and xanthochromia)
- CT angiogram and/or digital subtraction angiography to identify the cause
Clinical grading
| Grade | World Federation of Neurologic Surgeons | Hess and Hunt | Fisher (CT scan appearance) |
|---|---|---|---|
| 1 | Glasgow Coma Scale score 15, no motor deficit | Asymptomatic or minimal headache and slight nuchal rigidity | No blood detected |
| 2 | Glasgow Coma Scale score 13-14, no motor deficit | Moderate to severe headache nuchal rigidity, no neurological deficit other than cranial nerve palsy | Diffuse thin layer of subarachnoid blood (vertical layers <1 mm thick) |
| 3 | Glasgow Coma Scale score 13-14 with motor deficit | Drowsy, confusion, or mild neurological deficit | Localized clot or thick layer of subarachnoid blood (vertical layers ≥1 mm thick) |
| 4 | Glasgow Coma Scale score 7-12, with or without motor deficit | Stupor, moderate-to-severe hemiparesis, possibly early decerebrate rigidity and vegetative disturbances | Intracerebral or intraventricular blood with diffuse or no subarachnoid blood |
| 5 | Glasgow Coma Scale score 3-6, with or withour motor deficit | Deep coma, decerebrate rigidity, moribund appearance |
Complications
- Re-bleeding
- Seizures
- Hydrocephalus
- Vasospasm
Management
- Acute management
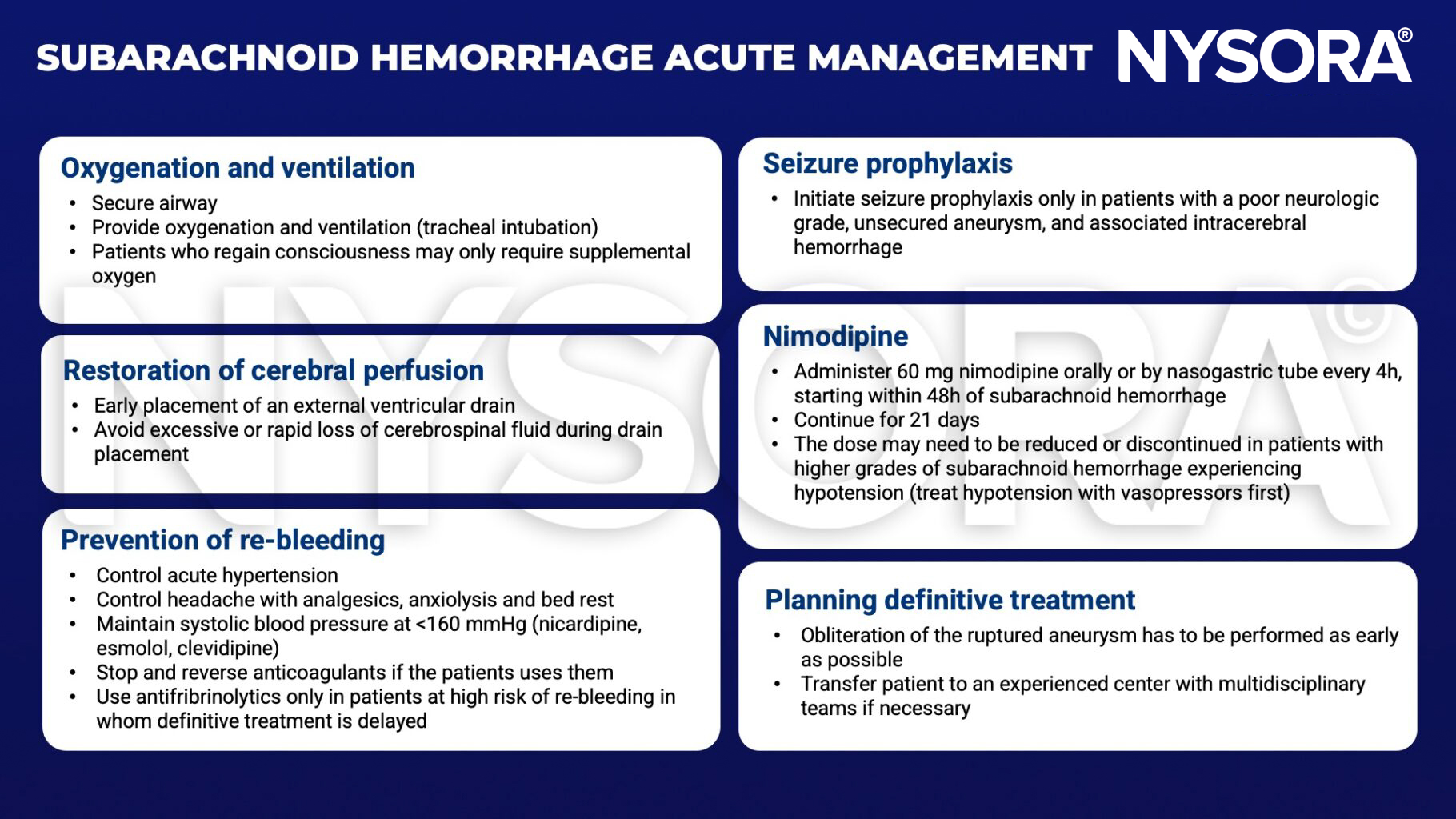
- Treatment options
-
- Endovascular coiling: Preferred in geriatric patients, particularly those with high-grade aneurysmal subarachnoid hemorrhage from the rupture of basilar apex aneurysm
- Surgical clipping: Preferred in patients with large intraparenchymal hematomas, aneurysm of the middle cerebral artery, and in those not likely to be compliant with long-term follow-up
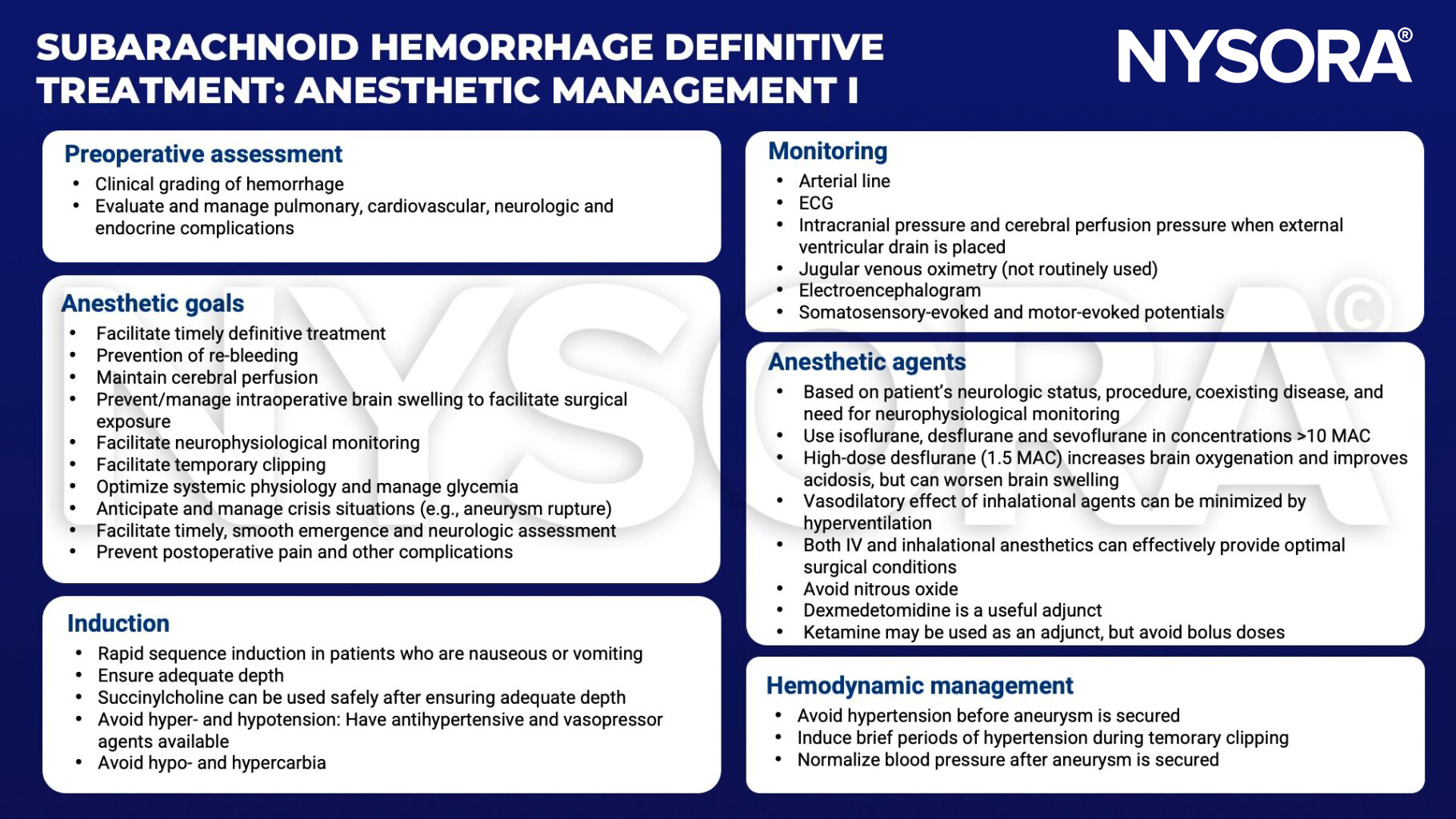
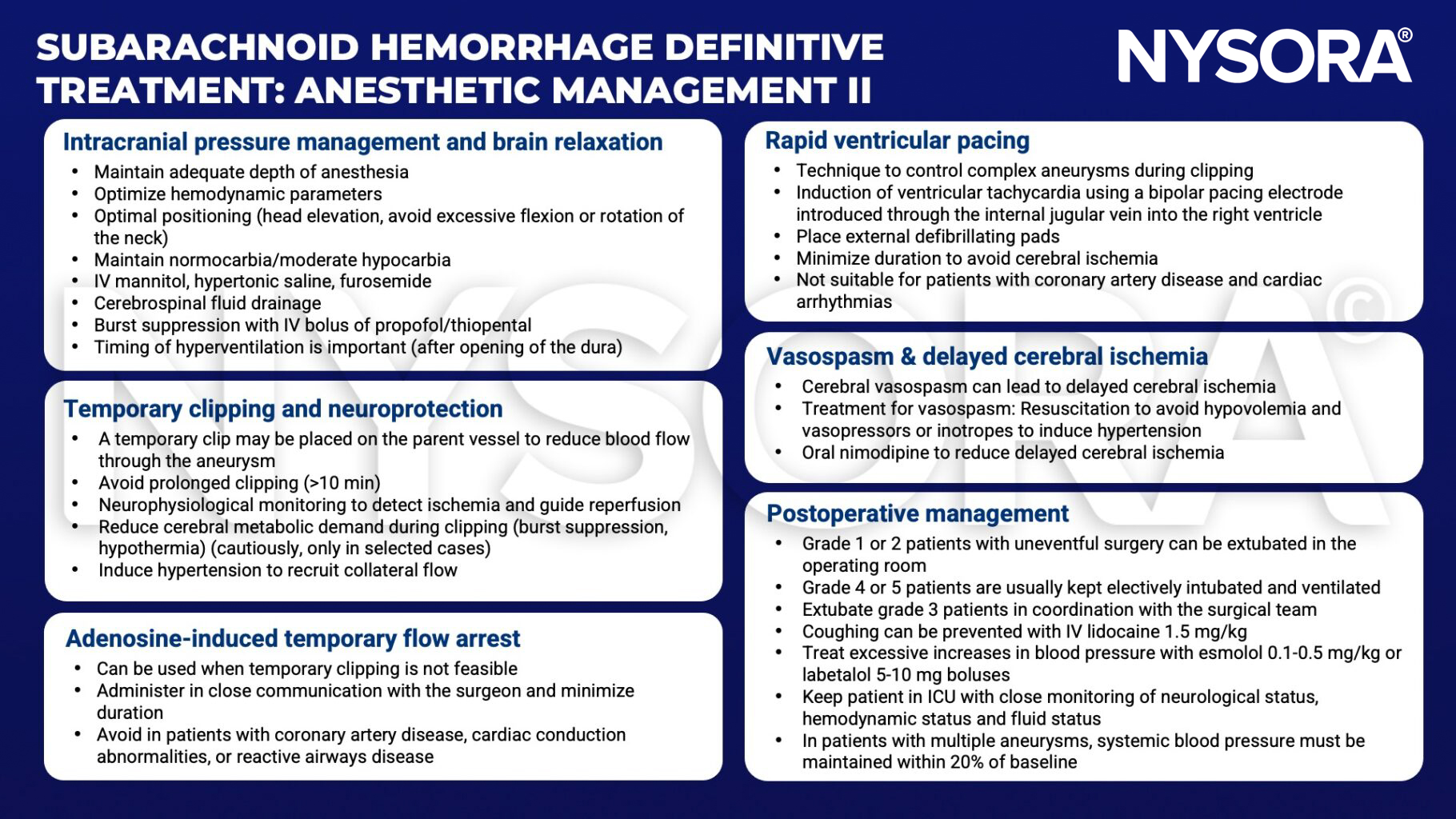
- Anesthetic management
Suggested reading
- Deepak Sharma; Perioperative Management of Aneurysmal Subarachnoid Hemorrhage: A Narrative Review. Anesthesiology 2020; 133:1283–1305
- Kundra S, Mahendru V, Gupta V, Choudhary AK. Principles of neuroanesthesia in aneurysmal subarachnoid hemorrhage. J Anaesthesiol Clin Pharmacol. 2014;30(3):328-337.
- Luoma A, Reddy U. Acute management of aneurysmal subarachnoid haemorrhage. Continuing Education in Anaesthesia Critical Care & Pain. 2013;13(2):52-8.
Clinical updates
Zoumprouli et al. (Current Opinion in Anesthesiology, 2025) report important recent advances in the critical care management of aneurysmal subarachnoid hemorrhage (aSAH), highlighting tighter systolic blood pressure control (<160 mmHg) before aneurysm securing to reduce rebleeding risk, and emerging evidence supporting prophylactic lumbar cerebrospinal fluid drainage to reduce delayed cerebral ischemia and improve neurological outcomes. The review also identifies a shift toward more individualized care, with data suggesting a liberal transfusion threshold around hemoglobin 9 g/dL and targeted normothermia (36–37.5 °C), alongside growing roles for quantitative imaging, CT perfusion–guided therapies, and investigational agents such as intravenous nimodipine and milrinone for vasospasm management.