Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the pathophysiology and symptoms of croup
- Diagnose croup and assess its severity
- Manage patients presenting with croup
Background
- Laryngotracheobronchitis or croup refers to inflammation of the larynx, trachea, and bronchi
- Common cause of cough, stridor, and hoarseness in children with a fever
- Most children experiencing croup recover without complications
- Rarely, croup can be lethal to infants
- Most often caused by a viral infection (parainfluenza, RSV, rhinovirus, enterovirus, influenza, adenovirus)
- More common in boys compared to girls
Pathophysiology
- Inhalation of virus infecting nasal and pharyngeal mucosal epithelia, further spreading to the subglottic space
- In children, the subglottic space is the most narrow part of the airway
- The inability of the cricoid to expand causes significant narrowing subglottic region secondary to the inflamed mucosa
- When the patient cries or becomes agitated, further dynamic obstruction can occur
Signs & symptoms
- Usually history of 1-3 days of rhinorrhea, nasal congestion, and fever
- Barky or seal-like cough
- Hoarse voice
- High-pitched inspiratory stridor
- Wheezing
- Crackles
- Air trapping
- Tachypnea
- Cyanosis
Diagnosis
- Mostly clinical diagnosis
- Abrupt onset of barky cough, stridor, and hoarseness
- Often dyspnea and fever
- Overt inspiratory stridor in the neck on auscultation
- Steeple sign on radiography (usually not necessary)
- Laboratory studies are rarely needed
- Laryngoscopy when alternate diagnoses are suspected (perform with caution when epiglottitis is suspected)
Differential diagnosis
| Condition | Typical age range | Clinical presentation | Diagnostic tests |
|---|---|---|---|
| Croup | 6 months to 3 years | Acute onset of barking cough, stridor, and hoarseness | None required |
| Bacterial tracheitis | <6 years | High fever, barking cough, respiratory distress, and rapid deterioration | Neck radiography (irregular tracheal mucosa) and complete blood count |
| Epiglottitis | 3 to 12 years | Acute onset of dysphagia, odynophagia, drooling, high fever, anxiety, and muffled voice | Neck radiography (thickened epiglottis) and complete blood count |
| Foreign bodyaspiration | <3 years | Acute onset of choking and/or drooling | Acute onset of choking and/or drooling |
| Hemangioma | <6 months | Stridor worse with crying | Airway endoscopy |
| Large airway lesions (subglottic stenosis, laryngeal cleft, tracheomalacia, laryngomalacia) | <6 months to 4.5 years | Recurrent episodes of barking cough and stridor | Airway endoscopy |
| Neoplasm | No age predilection | Progressive airway symptoms | Lateral neck radiography and CT |
| Peritonsillar abscess | 6 months to 3.5 years | Sore throat, fever, “hot potato” voice | Neck radiography, neck CT, and complete blood count |
| Retropharyngeal abscess | 2 to 4 years | Fever, drooling, dysphagia, odynophagia, and neck pain | Neck radiography (bulging posterior pharyngeal wall), neck CT, and CBC |
| Thermal injury/smoke inhalation | No age predilection | Exposure to heat, smoke, or chemical | Direct laryngoscopy |
Severity scoring
Westley Croup Score:
| Clinical sign | Score | |
|---|---|---|
| Level of consciousness | Normal (including sleep) | 0 |
| Disoriented | 5 | |
| Cyanosis | None | 0 |
| With agitation | 4 | |
| At rest | 5 | |
| Stridor | None | 0 |
| When agitated | 1 | |
| At rest | 2 | |
| Air entry | Normal | 0 |
| Decreased | 1 | |
| Markedly decreased | 2 | |
| Retractions | None | 0 |
| Mild | 1 | |
| Moderate | 2 | |
| Severe | 3 |
Total score:
- ≤2: Mild
- 3 – 7: Moderate
- 8 – 11: Severe
- ≥12: Impending respiratory failure
Complications
- Hospitalization
- Secondary bacterial infection
- Pneumothorax
- Otitis media
- Dehydration
- Lymphadenitis
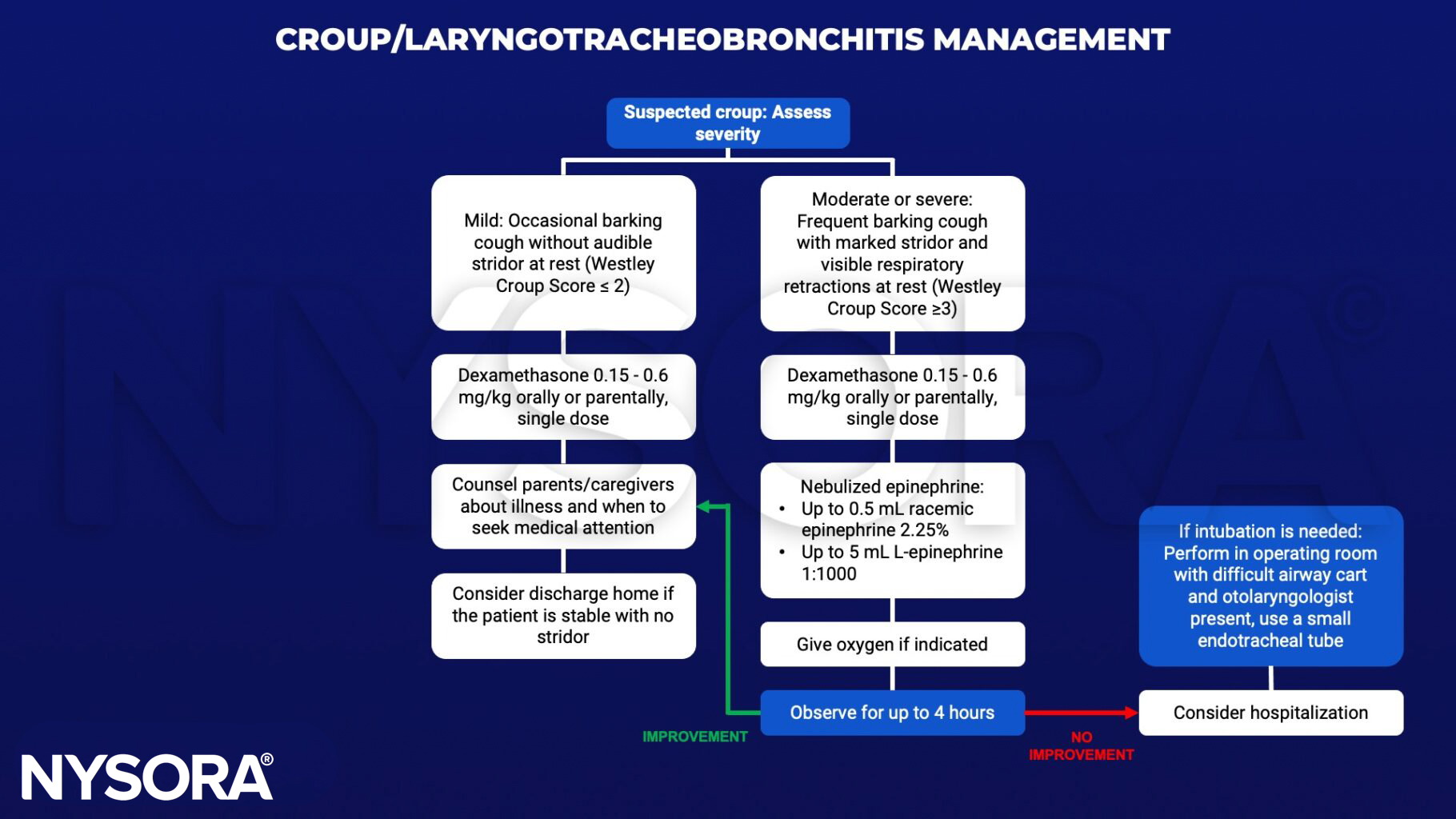
Management
Suggested reading
- Ernest S, Khandhar PB. Laryngotracheobronchitis. [Updated 2022 Jun 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519531/
- Smith DK, McDermott AJ, Sullivan JF. Croup: Diagnosis and Management. Am Fam Physician. 2018;97(9):575-580.
- Maloney E, Meakin GH. Acute stridor in children. Continuing Education in Anaesthesia Critical Care & Pain. 2007;7(6):183-6.