Learning objectives
- Recognize end-stage liver disease (ESLD)
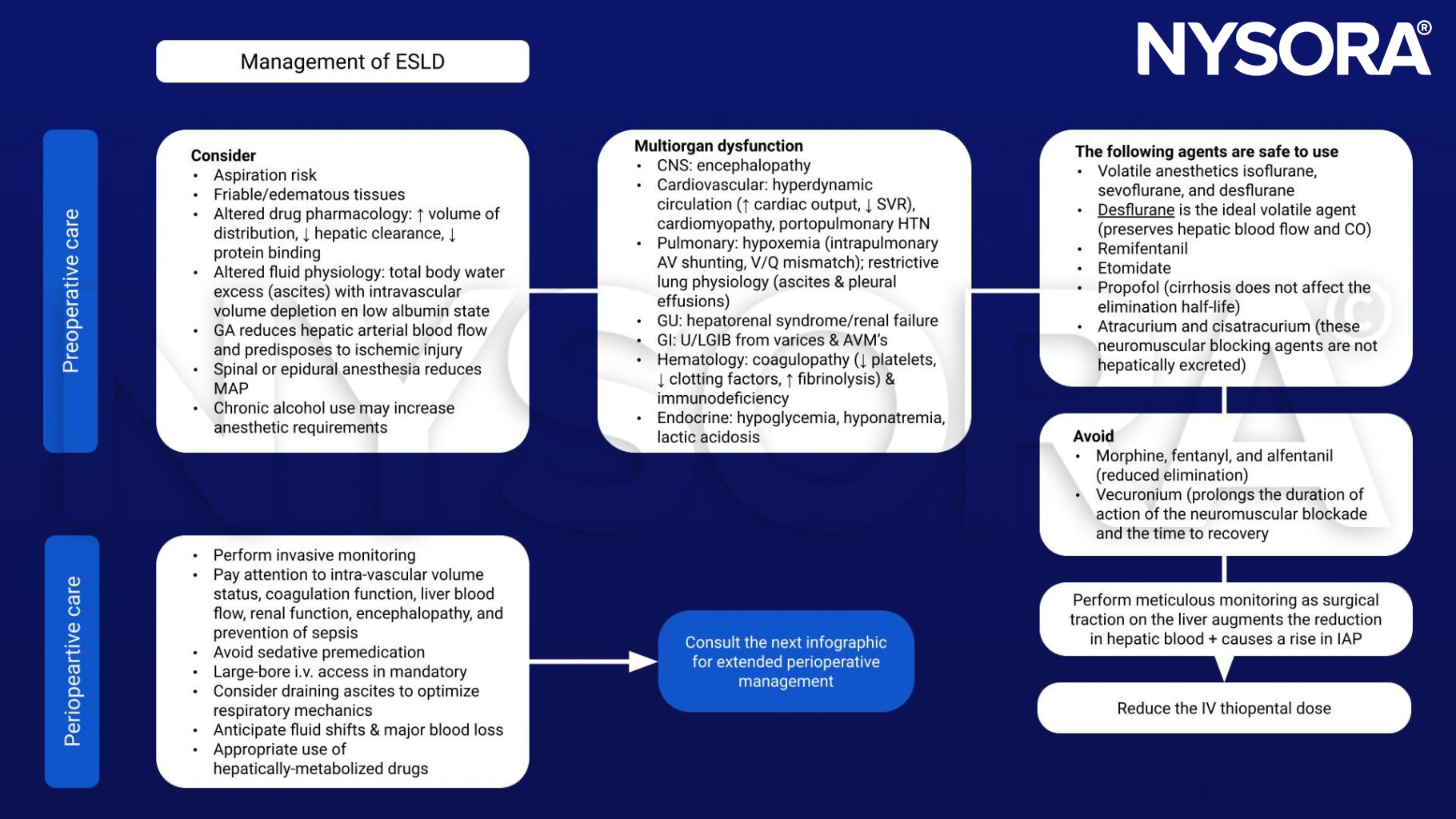
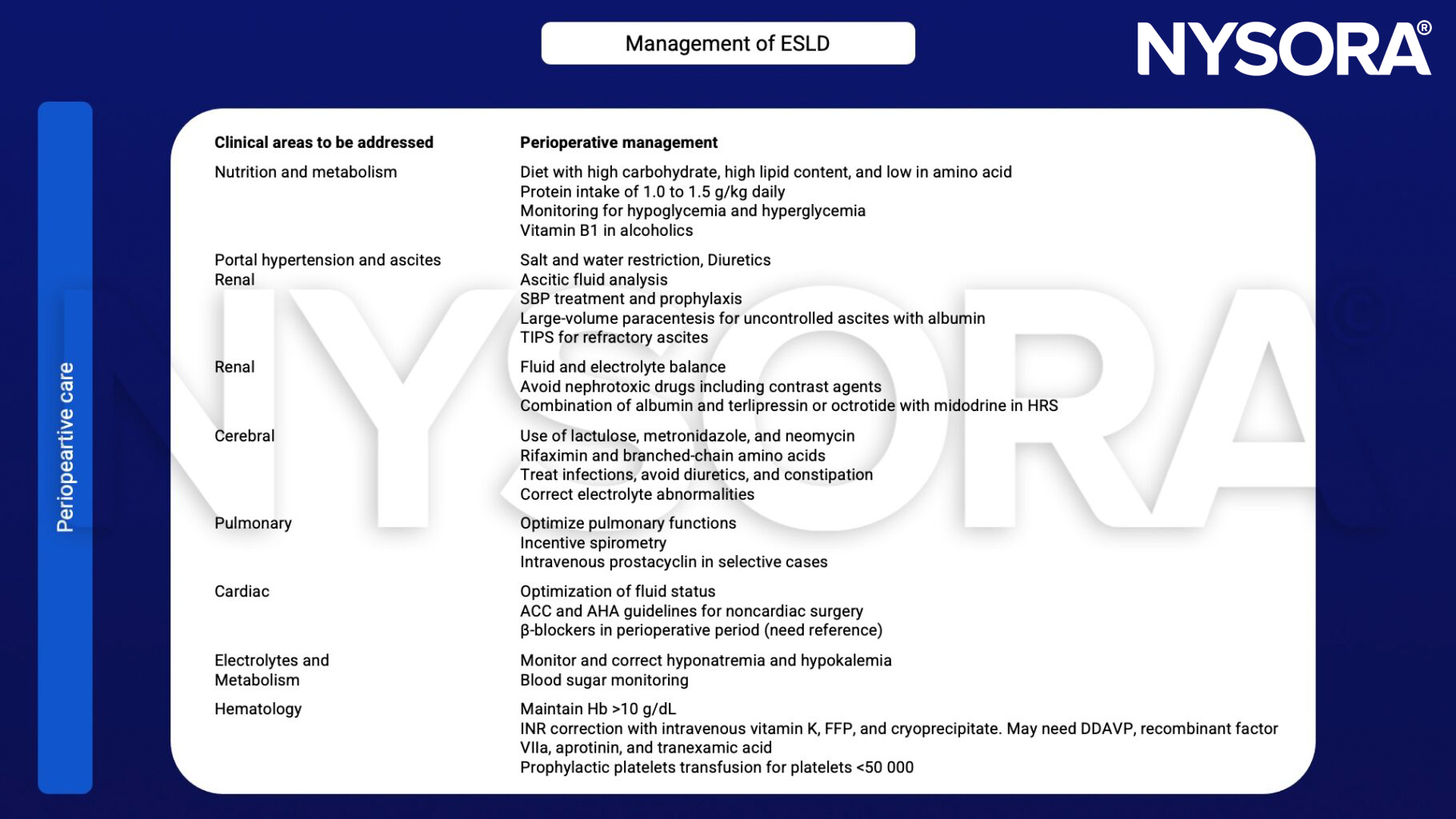
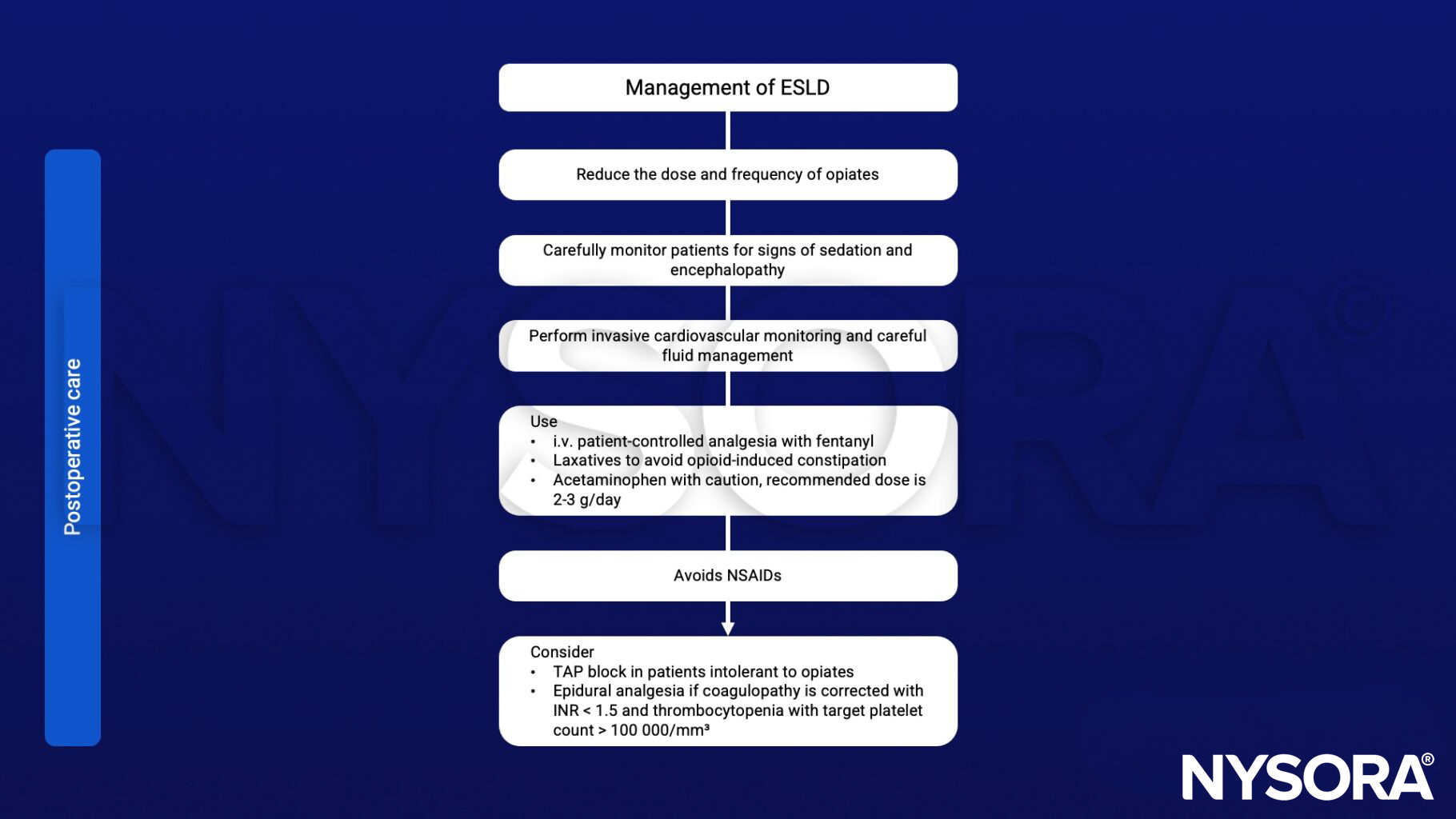
- Management of ESLD
Definition and mechanisms
- Chronic liver failure progresses over months to years
- Often the result of cirrhosis of the liver
- ESLD is the final stage of acute and chronic liver failure accompanied by ascites, variceal bleeding, hepatic encephalopathy, or renal impairment
- Patients with severe symptoms of cirrhosis may benefit from a liver transplant
Signs & symptoms
- Weakness
- Fatigue
- Loss of appetite
- Nausea
- Vomiting
- Weight loss
- Abdominal pain and bloating
- Itching
Decompensated cirrhosis
- Bleeding varices
- Ascites
- Encephalopathy
- Jaundice
Complications
- Edema and ascites
- Bruising and bleeding
- Portal hypertension
- Esophageal varices and gastropathy
- Splenomegaly
- Jaundice
- Gallstones
- Sensitivity to medications
- Hepatic encephalopathy
- Insulin resistance and type 2 diabetes mellitus
- Liver cancer
Anesthetic management
Keep in mind
- Patients with end-stage liver disease can also develop kidney failure
- This is often reversible with a liver transplant but some patients may need a combined liver and kidney transplant
Suggested reading
- Abbas N, Makker J, Abbas H, Balar B. Perioperative Care of Patients With Liver Cirrhosis: A Review. Health Serv Insights. 2017;10:1178632917691270. Published 2017 Feb 24.
- Rakesh Vaja, BSc MBChB FRCA, Larry McNicol, MBBS (Hons) FRCA FANZCA, Imogen Sisley, MBChB MRCP FRCA, Anaesthesia for patients with liver disease, Continuing Education in Anaesthesia Critical Care & Pain, Volume 10, Issue 1, February 2010, Pages 15–19
Clinical updates
Philips et al. (Journal of Clinical and Experimental Hepatology, 2023) explain when to start palliative care in end-stage liver disease, noting that high MELD or Child-Pugh scores, repeated hospitalizations, persistent ACLF, rapid MELD rise, and worsening frailty should prompt early palliative involvement rather than waiting until hospice. They emphasize structured goals-of-care discussions and proactive management of high-burden symptoms, safe acetaminophen use (dose-adjusted), avoidance of NSAIDs, cautious opioid selection (hydromorphone preferred in renal dysfunction), treatment of muscle cramps (taurine, baclofen), pruritus (cholestyramine, rifampin, naltrexone), and sleep disturbance, alongside selected disease-modifying interventions such as TIPS, long-term albumin (ANSWER trial context), alfapump®, and shunt embolization when appropriate to improve quality of life and transplant-free survival.
Gilbert-Kawai et al. (BJA Education, 2022) outline updated perioperative management strategies for patients with liver disease, emphasizing the use of contemporary risk stratification tools (CTP, MELD, and VOCAL-Penn) and early multidisciplinary involvement, particularly for high-risk or decompensated patients. The authors highlight the paradigm shift toward “rebalanced haemostasis,” advising against routine prophylactic FFP for elevated INR and instead recommending viscoelastic testing (e.g., ROTEM/ROTEG) to guide transfusion, with platelet transfusion generally reserved for counts <50×10⁹ L⁻¹. They further stress careful intraoperative hemodynamic management to prevent AKI and hepatic decompensation, avoidance of nephrotoxic/hepatotoxic drugs, and postoperative ICU/HDU monitoring for early detection of encephalopathy, infection, and synthetic dysfunction.