Learning objectives
- Recognize airway trauma
- Management of airway trauma
Definition and mechanism
- A life-threatening condition resulting from blunt and penetrating injuries to the neck and chest, as well as from medical procedures that may injure the airway
- Maxillofacial, neck, or laryngeal trauma
- Airway obstruction or obstruction by blood, secretions, tissue edema, debris, and vomitus
- Airway trauma can be associated with cervical spine injury which will worsen during intubation
Signs and symptoms
- Neck pain
- Hoarseness
- Dysphagia
- Cough
- Dysphonia
- Laryngeal dyspnea
- Loss of consciousness
- Stridor
- Cyanosis
- Hypoxemia
- Hamman’s sign or a mediastinal crunch (a crunching, rasping sound, heard over the precordium in mediastinal emphysema)
Blunt airway injury
| Anatomical territory | Associated problems | Caution: red flag signs and symptoms |
|---|---|---|
| Maxillofacial | Traumatic brain injury and base of skull fracture Cervical spine fracture Ophthalmic injury Vascular injury Pulmonary aspiration of blood and debris | Signs of Increased intracranial pressure Neurological deficit Neurogenic shock Significant bleeding from fracture displacement Bilateral anterior mandible fractures and airway obstruction Ventilatory failure |
| Laryngotracheal | Cervical fracture Vascular injury Oesophageal injury Rib fractures and flail segment Pneumothorax Haemothorax Pneumomediastinum Pulmonary contusion | Massive hemoptysis and stridor have previously been reported as cardinal features of severe laryngotracheal trauma Massive surgical emphysema Ventilatory failure Cardiovascular collapse |
| Trachea and bronchi | Vascular injury Oesophageal injury Rib fractures and flail segment Tension pneumothorax Hemothorax Pneumomediastinum Pulmonary contusion | Massive hemoptysis Massive surgical emphysema Ventilatory failure Cardiovascular collapse |
Management
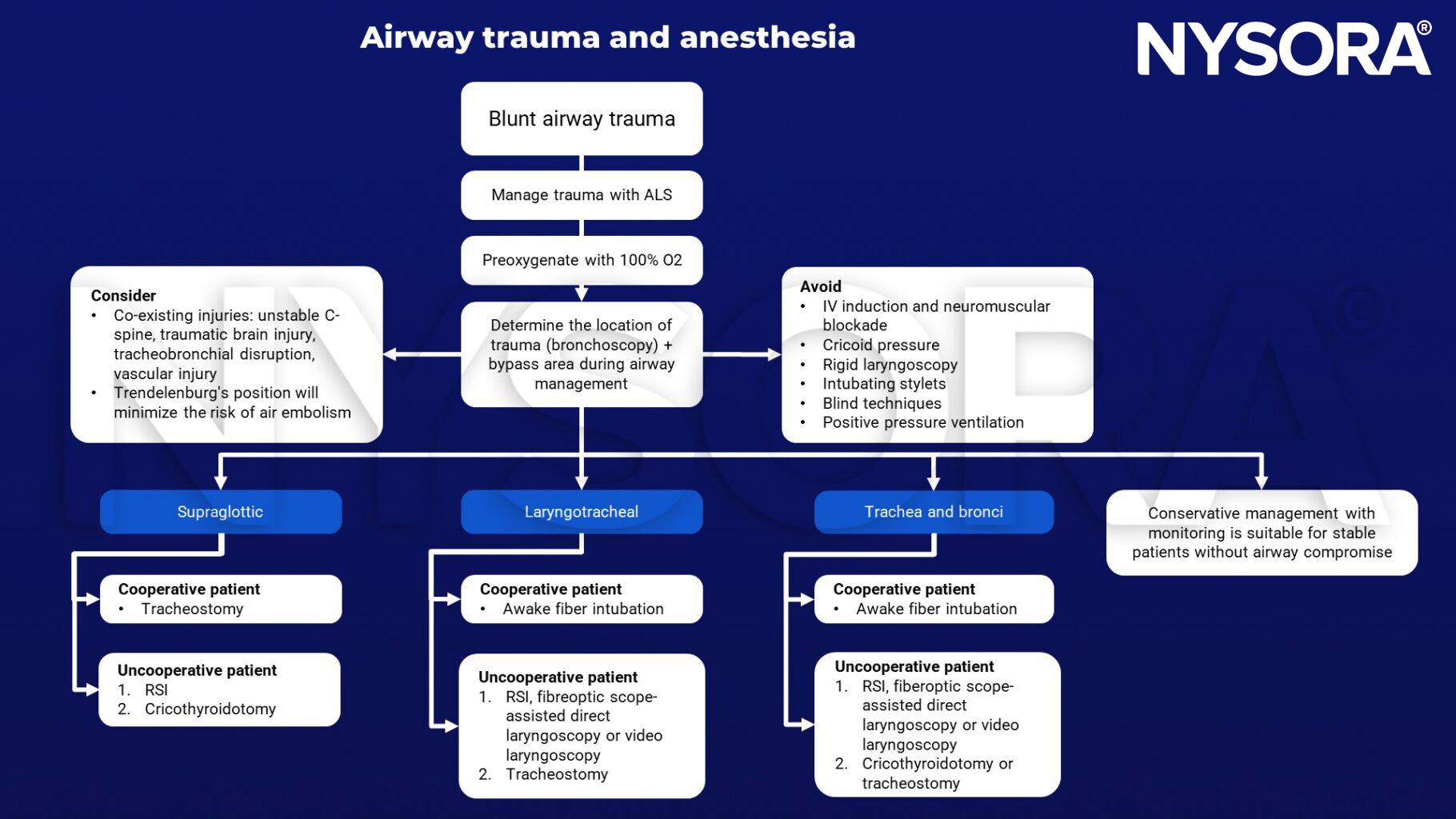
Keep in mind
- Full stomach vs difficult airway vs need for double-lumen tube
- Airway management may be difficult in the uncooperative or pediatric patient
Suggested reading
- Shilston J, Evans DL, Simons A, Evans DA. Initial management of blunt and penetrating neck trauma. BJA Educ. 2021;21(9):329-335.
- Mercer SJ, Jones CP, Bridge M, Clitheroe E, Morton B, Groom P. Systematic review of the anaesthetic management of non-iatrogenic acute adult airway trauma. Br J Anaesth. 2016;117 Suppl 1:i49-i59.
- Jain U, McCunn M, Smith CE, Pittet JF. Management of the Traumatized Airway. Anesthesiology. 2016;124(1):199-206.
- Prokakis C, Koletsis EN, Dedeilias P, Fligou F, Filos K, Dougenis D. Airway trauma: a review on epidemiology, mechanisms of injury, diagnosis and treatment. J Cardiothorac Surg. 2014;9:117.
Clinical updates
Abou-Arab et al. (BJA, 2020) describe two morbidly obese COVID-19 patients who developed severe tracheal perforations after difficult intubation with bougie use, resulting in pneumomediastinum, pneumothorax, and need for ECMO support. The cases highlight that Grade IV laryngoscopic views combined with blind bougie advancement can cause membranous tracheal rupture or cricoid membrane perforation, and they reinforce early use of videolaryngoscopy to minimize attempts and reduce airway trauma risk.