Learning objectives
- Definition and types of liver resections
- Anesthetic management of liver resection
Definition and mechanisms
- Hepatectomy or liver resection is a surgical operation to remove part or all of the liver
- Up to two-thirds can be removed as long as the rest of the liver is healthy
- The liver can regenerate functionally active tissue after resection by hyperplasia of the remnant tissue
- Liver is highly vascular and receives 25% of cardiac output, 80% is supplied by the portal vein and 20% by the hepatic artery
- Is the treatment of choice for colorectal hepatic metastases without evidence of more distant disease spread
- Also used in the management of benign and malignant primary hepato-biliary tumors, donation for transplantation, or hepatic trauma
- The most common liver cancers treated by partial hepatectomy include:
- Hepatocellular carcinoma
- Cholangiocarcinoma
- Metastatic colorectal cancer
- Other benign lesions include:
- Gallstones in the intrahepatic ducts
- Adenoma
- Liver cystadenoma or a cyst
Types of liver resections
| Major liver resection | Right or left hepatectomy or lobectomy removes the right or left lobe |
| Minor liver resection | Segmental or wedge resection removes a segment or a part of a segment with a tumor with a margin around it Another minor liver resection is the left lateral sectionectomy, which removes the lateral part (section) of the left lobe |
| Multiple liver resections | Multiple tumors may be resected at the same time |
| Two-stage liver resection | If it is too dangerous to remove all the tumors at once |
Complications
- Infection
- Bleeding
- Bile leakage
- Pleural effusion
- Ascites
- Deep vein thrombosis
- Kidney failure
- Liver failure
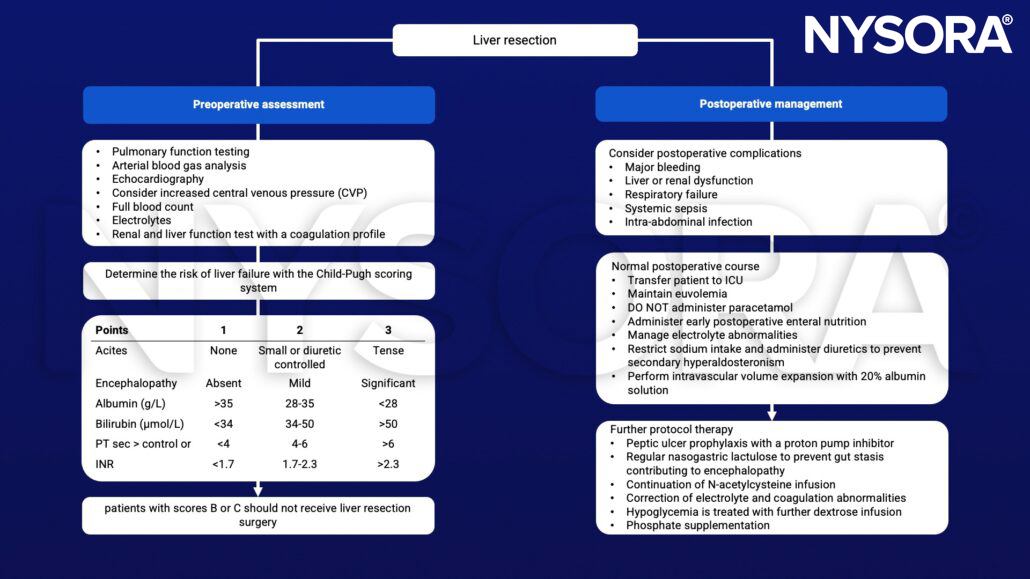
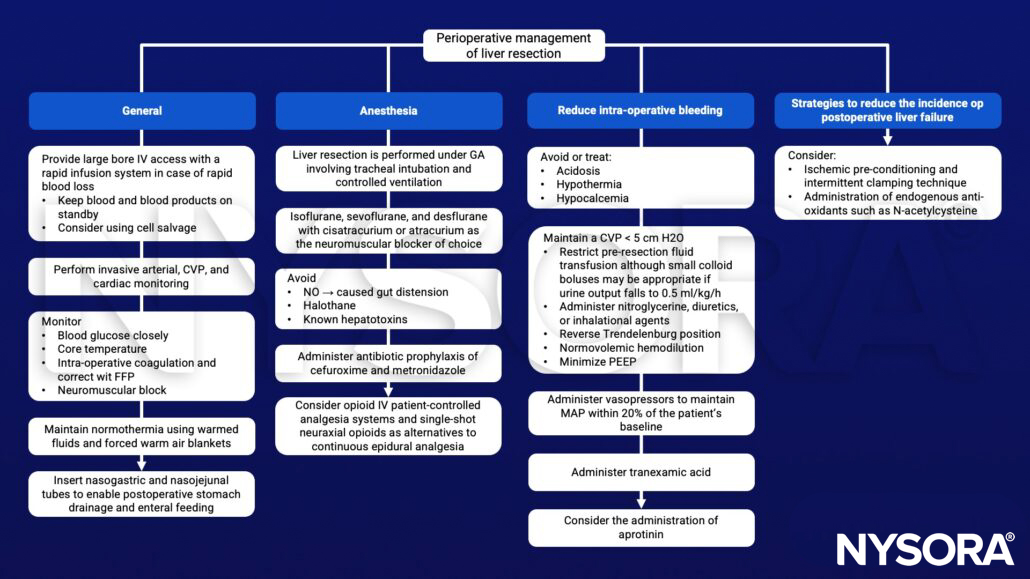
Management
- Consider:
- The potential for massive blood loss
- Risk of postoperative liver dysfunction and coagulopathy
- Altered drug metabolism
- Temporary occlusion of blood supply during liver resection (surgical technique to minimize bleeding) –> ↓ CO up to 10%, ↑ LV afterload by 20-30%
- Surgical manipulation may cause transient IVC compression and a decrease in venous return
Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Page AJ, Kooby DA. Perioperative management of hepatic resection. J Gastrointest Oncol. 2012;3(1):19-27.
- Harto A, Mills G. 2009. Anaesthesia for hepatic resection surgery. Continuing Education in Anaesthesia Critical Care & Pain9;1:1-5.
Clinical updates
Monsel et al. (EJA, 2025) provide a comprehensive, contemporary review of perioperative anesthesia and critical care management for patients with hepatocellular carcinoma (HCC), with liver resection as a central focus. The review synthesizes recent evidence on preoperative risk stratification (portal hypertension, cirrhosis severity, sarcopenia), intraoperative management (fluid strategy, coagulation, anesthetic technique, analgesia), and postoperative ICU considerations specific to hepatic surgery. It also contextualizes liver resection within modern multimodal HCC care, including minimally invasive approaches, locoregional therapies, and down-staging strategies.