Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
INTRODUCTION
Anesthesia of the foot can be accomplished by blocking the five peripheral nerves that innervate the area at the level of the ankle. This technique relies on anatomic landmarks that are easily identified. It does not require special equipment, paresthesia elicitation, nerve stimulation, special positioning, or patient cooperation. The ankle block can be used for all types of foot surgery and is safe and reliable, and has a high success rate.
Ankle block impairs ambulation on the affected leg, but to a lesser degree than sciatic or popliteal block, and patients can be discharged home before the block wears off. Long-acting local anesthetics with ankle block can provide excellent postoperative analgesia.
Indications and Contraindications
All types of foot surgeries can be carried out with ankle block, including bunionectomy, forefoot reconstruction, arthroplasty, osteotomy, and amputation. Ankle block can also provide analgesia for fracture and soft tissue injuries and or gout arthritis. Moreover, it can be used for diagnostic and therapeutic purposes with spastic equinovarus and sympathetically mediated pain. Because motor block of the proximal leg and calf is avoided, ankle block may be preferable to sciatic/femoral (saphenous) nerve block for outpatient forefoot surgery.
Ankle block should be avoided in patients with local infection, infection, edema, burn, soft tissue trauma, or distorted anatomy with scarring in the area of block placement.
NYSORA Tips
- Ankle block is well suited for ambulatory foot surgery.
- Ankle block can be life saving by avoiding the risks of general anesthesia in very ill patients having foot surgery (e.g. toes amputation, debridment).
Clinical Anatomy
The foot is innervated by five nerves (Figures 1 and 2). The medial aspect is innervated by the saphenous nerve, a terminal branch of the femoral nerve (Figure 3). The rest of the foot is innervated by branches of the sciatic nerve:
- The lateral aspect is innervated by the sural nerve arising from the tibial and communicating superficial peroneal branches (Figure 4).
- The deep ventral structures, muscles, and sole of the foot are innervated by the posterior tibial nerve, arising from the tibial branch (Figure 5).
- The dorsum of the foot is innervated by the superficial peroneal nerve, arising from the common peroneal branch (Figure 6).
- The deep dorsal structures and web space between the first and second toes are innervated by the deep peroneal nerve (see Figure 2).

FIGURE 1. Sensory innervation of the sole of the foot.

FIGURE 2. Sensory innervation of the medial aspect of the foot.
.")
FIGURE 3. Saphenous nerve at the level of the ankle (white arrow).

FIGURE 4. Sural nerve at the level of the ankle.

FIGURE 5. Tibial nerve at the level of the ankle.

FIGURE 6. Superficial peroneal nerve. Shown is the emergence of the superficial nerve and its distribution on the dorsum of the foot. 1, Superficial peroneal nerve; 2, sural nerve.
At the level of the malleoli, the saphenous, superficial peroneal, and sural nerves are relatively superficial and subcutaneous. The posterior tibial and deep peroneal nerves are deep to the flexor and extensor retinaculi, respectively, and are more difficult to locate. The posterior tibial nerve passes with the artery posterior to the medial malleolus deep to the flexor retinaculum, giving off a medial calcaneal branch to supply the lower and posterior surface of the heel. The nerve and artery then become superficial and more accessible as they curve behind and underneath the sustentaculum tali, a bony ridge on the calcaneus about 2–3 cm below the medial malleolus. The nerve then divides into medial and lateral plantar nerves.
The deep peroneal nerve passes lateral to the anterior tibial artery, extensor hallucis longus, and tibialis anterior tendons, and medial to the extensor digitorum longus tendon, deep to the extensor retinaculum. It becomes more superficial to travel sustenaculum tali (a bony medial calcaneal ridge 2–3 cm below the malleolus).
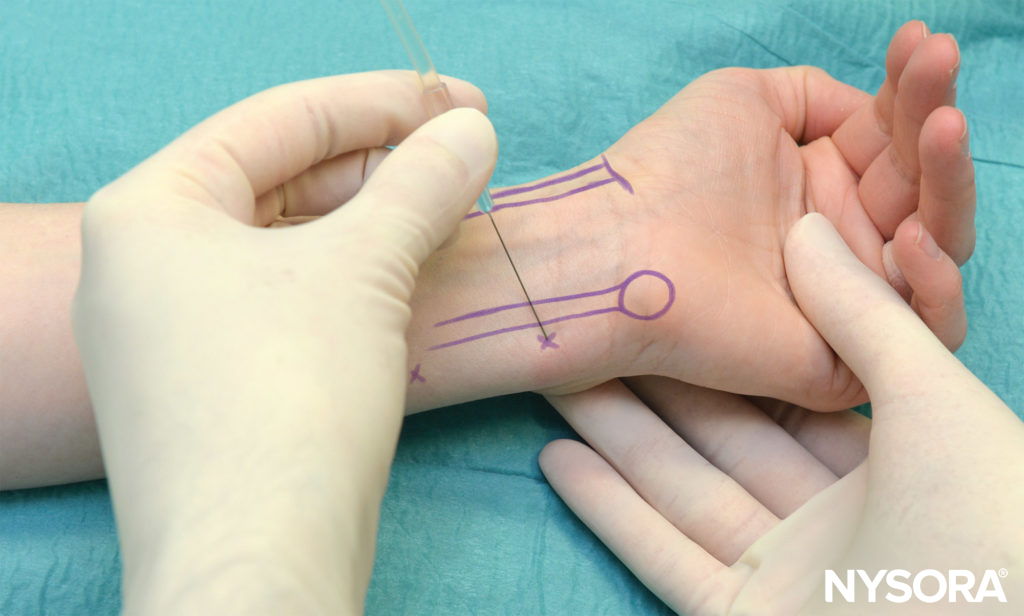
For block at the level of the malleoli, the saphenous, sural, and superficial peroneal nerves are blocked with a circumferential subcutaneous injection of 10–15 mL of local anesthetic along with a line just proximal to the malleoli and anterior from the Achilles tendon medially to laterally (Figures 8 through 10). The deep peroneal nerve is blocked by injection of 5 mL of local anesthetic just lateral to the extensor hallucis longus tendon deep to the retinaculum along the same circumferential line (Figure 11). The posterior tibial nerve is blocked by injection of the same volume of local anesthetic just posterior to the posterior tibial artery if palpable, or mid-way between the Achilles tendon and medial malleolus deep to the retinaculum (Figure 12).
For block at the midtarsal level, the saphenous, sural, and superficial peroneal nerves are blocked with a circumferential subcutaneous injection of 10–15 mL of local anesthetic along a line distal to the malleoli from the Achilles tendon medially to laterally. The deep peroneal nerve is blocked just lateral to the extensor hallucis longus tendon and medial to the dorsalis pedis artery. The posterior tibial nerve is blocked on either side of the posterior tibial artery (if palpable).

FIGURE 7. Maneuver to accentuate the landmarks for the deep peroneal nerve block. 1, Extensor hallucis longus; 2, extensor digitorum longus; 3, medial malleolus; 4, lateral malleolus.

FIGURE 8. Saphenous nerve block is accomplished by injection of 5 mL of local anesthetic subcutaneously at the level of the medial melleolus.

FIGURE 9. Superficial peroneal block.

FIGURE 10. Block of the sural nerve.

FIGURE 11. Block of the deep peroneal nerve.

FIGURE 12. Block of the posterior tibial nerve.
Equipment
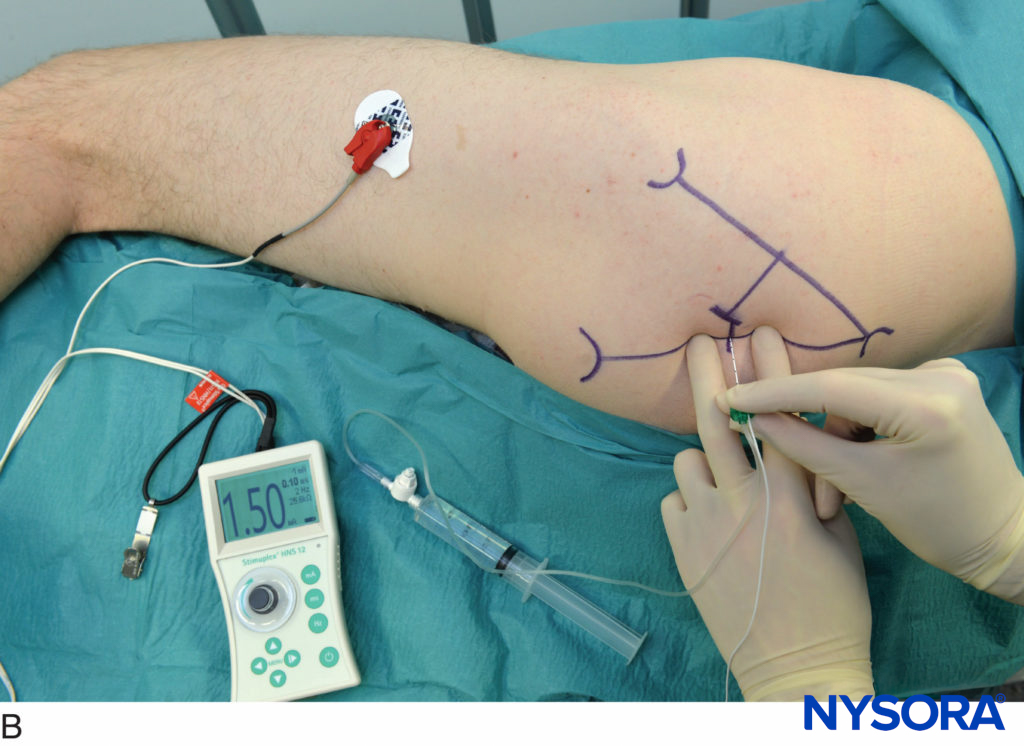
No special equipment other than disinfectant, gauze, and 10-mL syringes with 1.5-in., 25-gauge needles is required for ankle block. Although nerve stimulation is not necessary for distal approaches, it has been described for the proximal approach to the posterior tibial nerve.
If a tourniquet is required for surgery, a pneumatic ankle tourniquet should be used rather than an Esmarch bandage, because pressures with the latter are variable, are unknown, and may be extremely high, up to 380 mmHg.
Tourniquet pressures just above the malleoli between 200 and 250 mmHg should ensure a bloodless field and maximize safety. Ankle tourniquets are tolerated better than those placed at the midcalf or thigh, with less pain and no increase in neurologic complications. An audit of 1000 cases of ankle block revealed that with proper tourniquet application and the option of sedation, only 3.1% of patients complained of tourniquet pain. Risk factors for tourniquet pain were age over 70 and tourniquet times greater than 30 minutes.
NYSORA Tips
Always ensure that when a tourniquet is required, a padded ankle tourniquet is used to maximize patient comfort, minimize sedation, and prevent general anesthesia.
Technique
There are several techniques for performing ankle block; they can be classified as perimalleolar or midtarsal (inframalleolar) blocks. The location of the block determines the procedures that can be done; forefoot surgery is easily accomplished under a midtarsal block, but midfoot and more proximal foot surgery require a perimalleolar block. Success rates are higher with the midtarsal technique because the deep peroneal and posterior tibial nerves are more superficial, so this technique is preferable for forefoot surgery.
For all approaches, the patient can be supine, with a pillow under the calf to facilitate access.
Saphenous, Superficial Peroneal, and Sural Nerve Blocks
The saphenous, superficial peroneal, and sural nerves are already subcutaneous just proximal to the malleoli, and all can be blocked by a subcutaneous ring of local anesthetic at this location from just anterior to the Achilles tendon medially to laterally (see Figures 8 through 10). The advantage of blocking these nerves here is that the area under an ankle tourniquet will be anesthetized and tourniquet pain is less likely. By injecting slowly and continuously advancing a 1.5 -in., 25-gauge needle into the previously injected area, the number of injections and discomfort from them can be minimized. This subcutaneous ring of local anesthetic can also be performed distal to the malleoli for a midtarsal block.
Deep Peroneal Nerve Block
For the perimalleolar approach, the patient is asked to extend the great toe, which will tense and identify the extensor hallucis tendon (see Figure 7). A 1.5-in., 25-gauge needle is inserted immediately lateral to the tendon, perpendicular to the tibia, and is advanced until it contacts bone (see Figure 11). The needle is then withdrawn a few millimeters, and after negative aspiration, 5 mL of local anesthetic is injected. For the midtarsal approach, the extensor hallucis tendon is identified as mentioned above, but more distally, and the pulse of the dorsalis pedis artery is identified on the top of the foot as well. A 1.5-in., 25-gauge needle is inserted immediately lateral to the tendon and medial to the artery, and after negative aspiration, 5 mL of local anesthetic is injected.
Posterior Tibial Nerve Block
For the perimalleolar approach, a 1.5-in., 25-gauge needle is inserted just posterior to the pulse of the posterior tibial artery behind the medial malleolus, or if it cannot be palpated, mid-way between the Achilles tendon and the posterior aspect of the medial malleolus (see Figure 12). The needle is directed toward the tibia at a 45-degree angle to contact bone. The needle is then withdrawn a few millimeters, and after negative aspiration, 5 mL of local anesthetic is injected. For the midtarsal approach, there are two approaches. Either the posterior tibial artery is identified below and distal to the medial malleolus on the calcaneus, or the sustentaculum tali is identified. The needle is directed toward the calcaneus, slightly under the bony shelf of the sustentaculum tali, or on either side of the tibial artery. After contact with bone, the needle is withdrawn 2 mm, and 5 mL of local anesthetic is injected.
NYSORA Tips
Because the posterior tibial artery is not palpable in all individuals, the sustentaculum tali is a more consistent, easily palpable landmark for posterior tibial nerve block.
MAYO BLOCK
Clinical Anatomy
The Mayo block is a combination of the nerve block and a field block that involves the infiltration of local anesthesia through the tissues proximal to a surgical site in a ring shape around the first metatarsal (most commonly) or a lesser metatarsal base. When the Mayo block is used around the first metatarsal base, the nerves that are anesthetized include the medial dorsal cutaneous nerve and the deep peroneal nerve on the dorsal aspect. The first and second branches of the common plantar digital nerves, which are superficial branches of the medial plantar nerve, provide sensation to the plantar aspect of the first metatarsal.
Indications
The Mayo block is commonly used in podiatric office surgery to anesthetize the area before performing bunion or hallux surgery. The injection can be used with or without epinephrine.
Technique
The Mayo block consists of three or four separate injections. The block is performed by raising a wheal of local anesthetic proximally and dorsally in the first intermetatarsal space and advancing the needle in the plantar direction while injecting 3–5 mL of local anesthetic (Figure 13). The needle is then withdrawn partially and redirected medially, raising a subcutaneous wheal along its course (3–5 mL) (Figure 14). The needle is then removed and reentered and directed laterally to raise a subcutaneous wheal along the course (3–5 mL) (Figure 15). Finally, the needle is removed and directed plantar-medially to the metatarsal and injected from medial to lateral underneath the metatarsal bone (3–5 mL) (Figure 16). The block encircles the entire metatarsal bone.
")
FIGURE 13. Mayo block, step 2. After a wheal of local anesthesia is raised at the level of the first intermetatarsal space, the needle is advanced in the plantar direction and 3–5 mL of local anesthetic is injected. (Arrow, First metatarsal bone; X, first metatarsal space.)
")
FIGURE 14. Mayo block, step 1. The needle is entered subcutaneously dorsomedially raising a wheal along the course. (Arrow, First metatarsal bone; X, first metarsal space.)
")
FIGURE 15. Mayo block, step 3. The needle is directed medial to lateral subcutaneously and 3–5 mL is injected. (Arrow, First metatarsal bone; X, first metarsal space.)
")
FIGURE 16. Mayo block, step 4. The needle is directed medial to lateral and plantar underneath the metatarsal bone while injecting 3–5 mL of local anesthetic. (Arrow, First metatarsal bone; X, first metarsal space.)
Choice of Local Anesthetic
The decision regarding which local anesthetic solution to use depends on the anticipated duration of surgery and the degree of postoperative pain. Commonly used solutions include lidocaine 2% for shorter, less painful procedures and ropivacaine 0.5% for longer or more painful procedures.
Blood levels of plain local anesthetic are well below toxic levels, even when large amounts are used. Bilateral midtarsal blocks performed with up to 30 mL of plain 0.75% bupivacaine resulted in peak venous blood levels of 0.5 mcg/mL, whereas 13 mL of 2% lidocaine for unilateral block resulted in 1.1 mcg/mL. No adverse local anesthetic effects were reported in a series of 66 patients receiving bilateral ankle blocks with mixtures of plain lidocaine and ropivacaine 0.75%, ropivacaine 0.75% or ropivacaine 0.75% with clonidine 1 mcg/kg. The addition of epinephrine with ankle block remains controversial. The preponderance of the literature suggests that epinephrine should not be used in distal extremity local anesthesia. However, low concentrations of epinephrine in local anesthetic solutions have been used with remarkable safety. The overall incidence of severe vascular complications after injection of epinephrine-containing local anesthetics has been estimated to be 1 per 132,000 injections.
Note that the use of 1:100,000 solutions of epinephrine has a 2.5 greater risk of complications compared with 1:200,000, suggesting that when epinephrine is indicated, it should be used only as dilute concentrations (i.e., 1:300,000 or less). Regardless, epinephrine is probably best avoided altogether in patients with peripheral vascular disease or compromised circulation.
The high-efficacy, prolonged postoperative analgesia and safety of plain bupivacaine and ropivacaine suggest that these drugs should be the choice for surgery in which postoperative pain is expected. However, blocks should be performed 30 minutes before surgery (minimum of 20 minutes) when using bupivacaine or ropivacaine to maximize success rate. In a prospective analysis of 1000 patients, the failure rate was significantly lower after waiting 20 minutes after the injection, with the lowest failure rates occurring after 50 minutes.
NYSORA Tips
When using ropivacaine or bupivacaine, perform the block at least 30 minutes before surgery to allow adequate time for block onset.
PERIOPERATIVE MANAGEMENT
Because performing an ankle block requires more than one injection and requires subcutaneous infiltration, it can cause more discomfort than single-injection blocks. In addition to gentle, slow injection, patients usually benefit from anxiolysis and analgesia with midazolam 1–4 mg and fentanyl 25–100 mcg. Before starting surgery, the block should be checked in all five nerve distributions, and supplemental local anesthetic can be injected if necessary.
Tourniquets should have a soft lining or padding and should be placed just above the malleoli. Ankle tourniquets are tolerated better than those placed at the midcalf or thigh, with less pain and no increase in neurologic complications. An audit of 1000 cases of ankle block revealed that with proper tourniquet application and the option of sedation, only 3.1% of patients complained of tourniquet pain.
Supplementation by the surgeon intraoperatively may rescue an incomplete block. Postoperatively, acetaminophen and a nonsteroidal anti-inflammatory drug (NSAID) can be continued routinely. Depending on the extent and type of surgery, small doses of a long-acting opioid such as controlled-release oxycodone may provide a smooth transition from block to postoperative analgesia and may facilitate rehabilitation. Ambulation with crutches is possible right after surgery. Elevation of the leg, when not ambulating, may further decrease postoperative pain.
COMPLICATIONS AND HOW TO AVOID THEM
Because most surgery is done under tourniquet, it is difficult to differentiate the cause of neurologic complications. In a retrospective study of 3027 patients with pneumatic ankle tourniquet at relatively high pressures of 325 mmHg, there were three cases (0.1%) of posttourniquet syndrome. Ankle tourniquets have been used routinely with as little as 200 mmHg pressure, although a bloodless surgical field may require 218.6 ± 34.6 mmHg, with younger normotensive patients requiring only 203.9 ± 22.3 mmHg. Thus, no more than 250 mm Hg pressure is necessary, and more pressure may be harmful.
The incidence of complications after ankle block is low and is usually in the form of transient paresthesias, which almost always resolve. The incidence is usually less than 1%, although it ranges from 0%–10%, depending on the source of the data. Complications may occur from injection or from application of the tourniquet. In a prospective survey of 284 patients with posterior tibial, sural, and saphenous blocks at the ankle and common peroneal block at the knee, no patient developed postanesthetic neuralgia or other complications. In three other studies with a total of 120 patients who received ankle blocks, no patients developed complications. After midtarsal ankle block in 71 of 100 patients available for follow-up, 1 patient developed transient posterior tibial paresthesias, which resolved in 4 weeks. In another study of 40 patients, 1 developed paresthesias lasting 6 weeks, which resolved. In a retrospective study of 1373 patients who received ankle block followed by a posterior tibial nerve catheter for postoperative analgesia, 5 patients had transient paresthesias, with 1 patient developing neurolysis (probably related to the catheter insertion) but with complete recovery. In a prospective randomized trial of 32 patients (40 total feet) undergoing forefoot surgery under ankle tourniquet (inflation pressure 100 mmHg over systolic) under complete or selective ankle block of which 26 patients (33 total feet) were available for follow-up to injection or tourniquet, 1 had ankle pain, and 1 had cold toes.
Local anesthetic systemic toxicity would be expected to be rare, given the low blood levels after injection. In the retrospective series of 1373 patients previously mentioned, 1 patient had a convulsion, thought to be secondary to an intravascular injection. In another series of 1295 patients who received standard and modified ankle blocks as well as digital nerve blocks, 3 patients had vasovagal reactions and 1 had an episode of hypotension and supraventricular tachycardia, thought by the investigators to be from lidocaine toxicity. No other complications were seen in this series.
There are single case reports of injection-related complications such as an Achilles tendon avulsion from tibial nerve block in a patient with spastic talipes equinovarus, and acute compartment syndrome from ankle block in a patient with previous scarring from forefoot arthroplasty.
Both of these patients had altered anatomy, which may have predisposed them to the complication.
NYSORA Tips
- Ensure that the patient’s anatomy is normal before injection and avoid injecting in scarred or swollen areas.
- Avoid injection of large volumes; most ankle blocks can be performed with less than 30 mL of local anesthetic.
- There should be no resistance to injection at any time. If there is, stop the injection and reposition the needle.
Clinical updates
Pascarella et al. (Journal of Clinical Medicine, 2025) provide an updated, comprehensive review showing that motor-sparing, ultrasound-guided regional techniques—particularly ankle and high-ankle blocks—are preferred for ambulatory foot and ankle surgery, as they balance effective analgesia with early mobilization and lower fall risk than popliteal sciatic blocks. The authors highlight intravenous dexamethasone as a key adjuvant to prolong block duration and reduce opioid requirements, and note growing but still limited evidence for WALANT and Mayo blocks in selected forefoot procedures. Overall, the review emphasizes tailoring block selection, adjuvants, and multimodal analgesia to procedure type and discharge goals, rather than adopting a one-size-fits-all regional strategy.
Schou et al. (Foot and Ankle Surgery, 2024) performed a systematic review with meta-analysis and trial sequential analysis showing that ankle blocks prolong analgesia by ~7 hours compared with no intervention or sham, but with very low-certainty evidence and no reliable reduction in 24-hour opioid consumption. When compared with sciatic nerve blocks, ankle blocks provided ~6–7 hours shorter analgesia and may be associated with slightly higher opioid use, though certainty remained low due to high risk of bias and sparse data. Overall, the findings support ankle blocks as a mobility-preserving option for outpatient forefoot surgery, but highlight the need for higher-quality trials to define their role within multimodal analgesia pathways.
Moosa et al. (BJA Education, 2022) provide an updated, practical synthesis of ultrasound-guided regional anaesthesia for foot and ankle surgery, emphasizing that more proximal ultrasound-guided ankle blocks (rather than traditional landmark techniques at the malleoli) reliably extend sensory coverage to the heel and improve tolerance of ankle tourniquets. The review highlights procedure-specific block selection (ankle vs popliteal sciatic ± saphenous) to balance analgesia with postoperative motor function, noting that ankle blocks preserve mobility compared with popliteal approaches. It also underscores the growing roles of perineural catheters and IV dexamethasone to prolong analgesia during high-pain procedures, while emphasising vigilance for compartment syndrome and safe postoperative mobilisation strategies.