Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About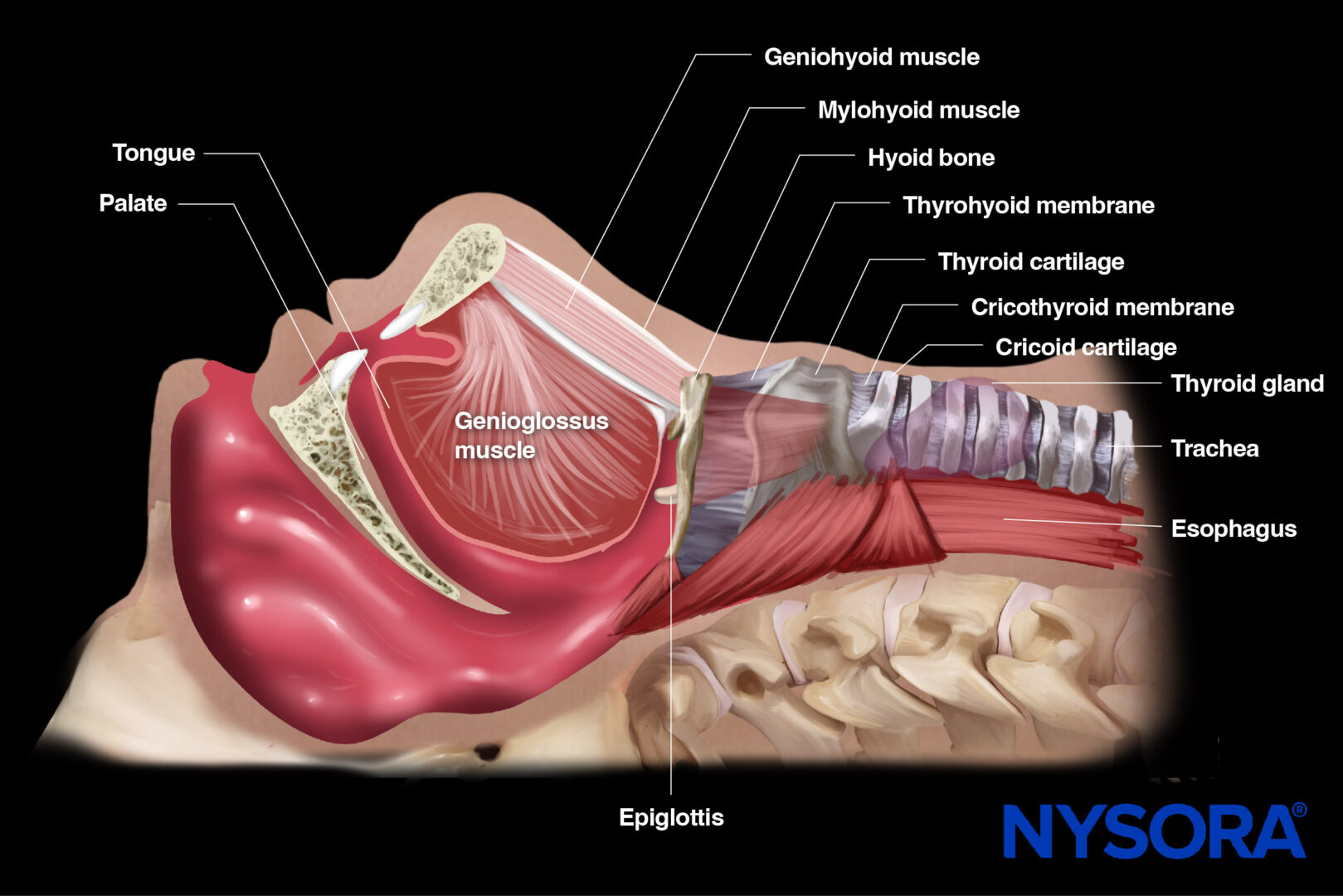
Indications
- Preoperative assessment:
- Airway size and prediction of the ETT size
- Identification of anatomic variations and airway obstructions
- Prediction of difficult laryngoscopy (not validated)
- Intraoperative guidance:
- Correct ETT placement and depth in the trachea
- Surgical airway assistance: real-time guidance for cricothyroidotomy or tracheostomy
- Sensory blocks for awake intubation
- Correct ETT placement and depth in the trachea
- Postoperative follow-up:
- Evaluation of the vocal cords: post-extubation stridor or failure
- Prediction of post-extubation stridor/failure (not validated)
- Evaluation of the vocal cords: post-extubation stridor or failure
- Critical care setting during ventilatory weaning:
- Evaluation of vocal cords and epiglottis
Essential info
- Airway ultrasound is non-invasive, safe, highly accurate, easily accessible, and quick to learn in the OR or ICU.
- Airway ultrasound can provide real-time assessment and management of airway-related conditions in routine and emergency settings.
- Difficult airway management leads to high morbidity and mortality. 64% of anesthesia-associated deaths are the result of airway management complications, both during induction and securing of the airway
- A transverse view of the neck can confirm the ETT placement in the trachea with 98% sensitivity and 98% specificity.
Functional anatomy
The upper airway consists of several structures that conduct air from the nose and mouth to the lower airway. These structures include the nasal cavity, oral cavity, pharynx, larynx, and trachea. Together, they ensure proper airway patency, filtration, and protection of the lower respiratory tract. They are usually classified into two parts: suprahyoid (mouth floor) and infrahyoid (neck).
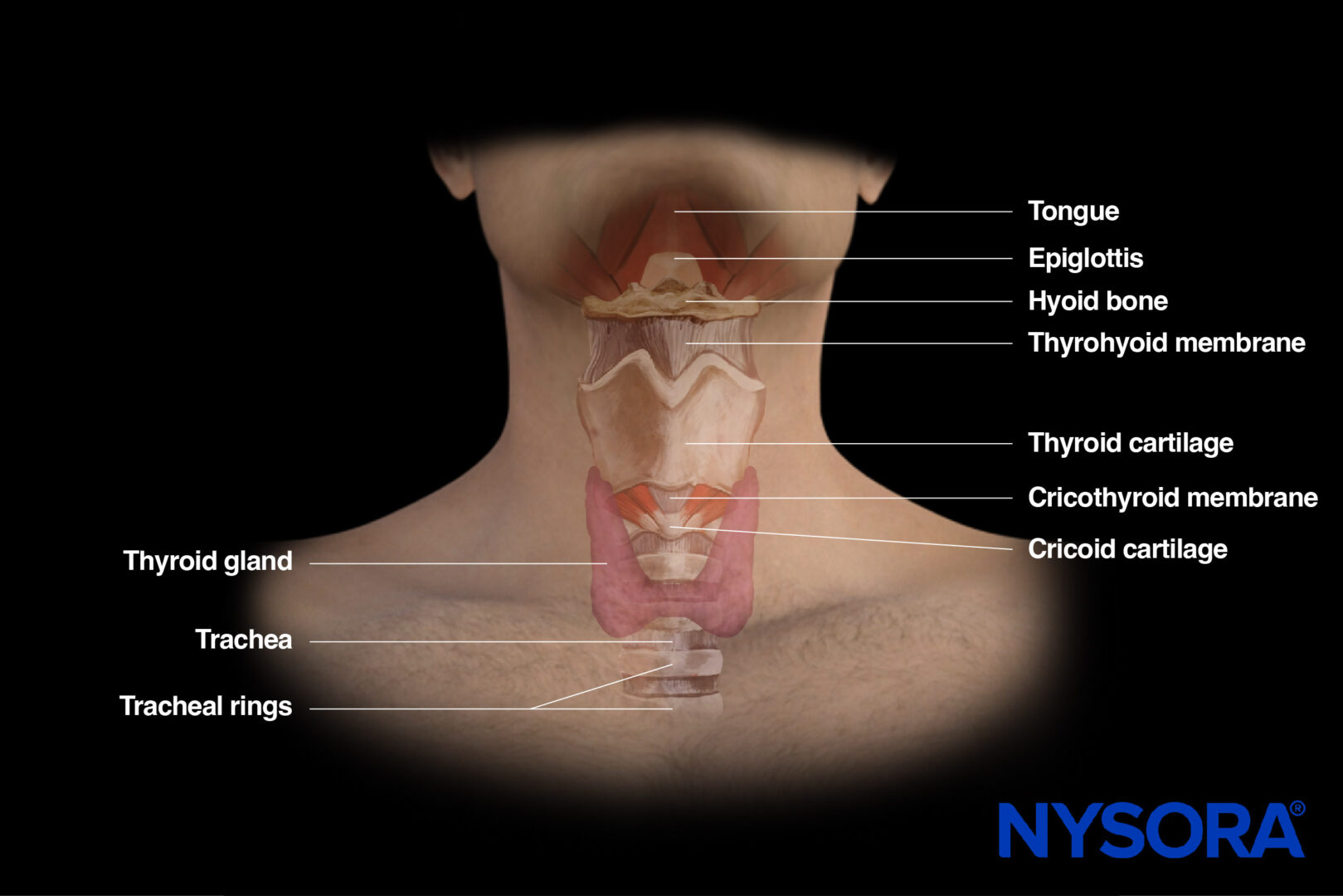
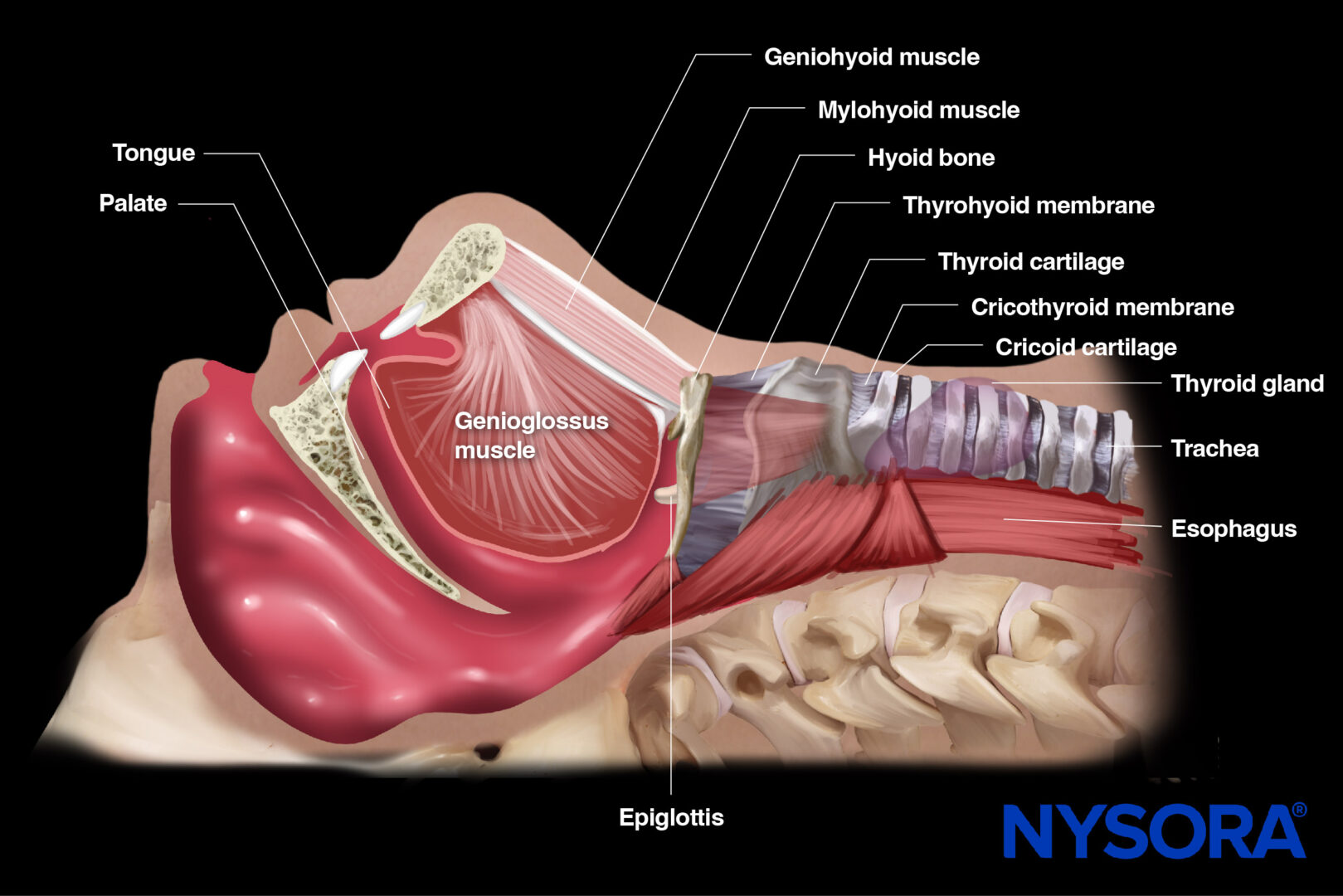
Functional anatomy of the airway.
Structures
- Nasal cavity
This cavity warms, humidifies, and filters air as it passes through. It is lined with mucous membranes and nasal turbinates.
- Oral cavity
Alternative pathway for air, particularly during mouth breathing. It includes the lips, the lining inside the cheeks and lips, the front two-thirds of the tongue, the upper and lower gums, the mouth floor under the tongue, the bony roof of the mouth, and the small area behind the wisdom teeth.
- Mouth floor
The area under the tongue, between the sides of the mandible. Formed by suprahyoid muscles: the mylohyoid muscle, geniohyoid muscle, digastric muscle, and stylohyoid muscle.
- Hyoid bone
The hyoid bone does not form joints with any other bone, and muscles and ligaments connect it to the mouth floor, tongue, epiglottis, pharynx, throat, mandible, temporal bone, and styloid process. The thyrohyoid ligament or membrane attaches the posterior surface of the body of the hyoid bone to the upper border of the thyroid cartilage.
- Pharynx
The pharynx is a common passageway for air entering the larynx and lungs and food and liquid entering the esophagus. The pharynx begins behind the nose and opens into the larynx and esophagus. It is divided into three parts: the nasopharynx (the upper part of the pharynx behind the nose), the oropharynx (the middle part of the pharynx), and the hypopharynx (the bottom part of the pharynx). It also plays an important role in speech.
- Larynx
Contains the vocal cords and serves as the entry point to the lower airway. It plays a role in phonation, swallowing, and preventing food aspiration while breathing. It is divided into three parts: supraglottis, glottis (vocal cords), and subglottis. The laryngeal skeleton consists of nine cartilages; three are unpaired cartilages (thyroid, cricoid, epiglottis), and three are paired cartilages (arytenoid, corniculate, cuneiform). The cartilages are held together by joints and ligaments, including the cricothyroid ligament or membrane, with its apex in the middle of the thyroid cartilage and its base in the superior border of the cricoid cartilage.
- Thyroid gland
A butterfly-shaped endocrine gland below the larynx consisting of two lobes on both sides of the trachea connected by a central isthmus.
- Trachea
Connects the larynx to the bronchi, lined with ciliated epithelium and cartilaginous rings for support.
Innervation
- Nasal Cavity
Sensory innervation by branches of the trigeminal nerve (V): the ophthalmic (V1) and maxillary (V2) divisions.
- Pharynx
Sensory innervation of the nasopharynx is provided by branches of the trigeminal nerve’s maxillary division (V2) (V). The oropharynx and laryngopharynx receive sensory innervation from the glossopharyngeal nerve (IX) and motor innervation from the vagus nerve (X), specifically its pharyngeal branches.
- Larynx
Sensory innervation of the supraglottic region by the internal branch of the superior laryngeal nerve and the subglottic region by the recurrent laryngeal nerve, both branches of the vagus nerve. The recurrent laryngeal nerve also supplies motor innervation to the intrinsic muscles of the larynx, while the external branch of the superior laryngeal nerve innervates the cricothyroid muscle.
- Trachea:
Sensory innervation by branches of the vagus nerve (X), primarily the recurrent laryngeal nerve. The vagus nerve also supplies motor innervation to the tracheal smooth muscle.


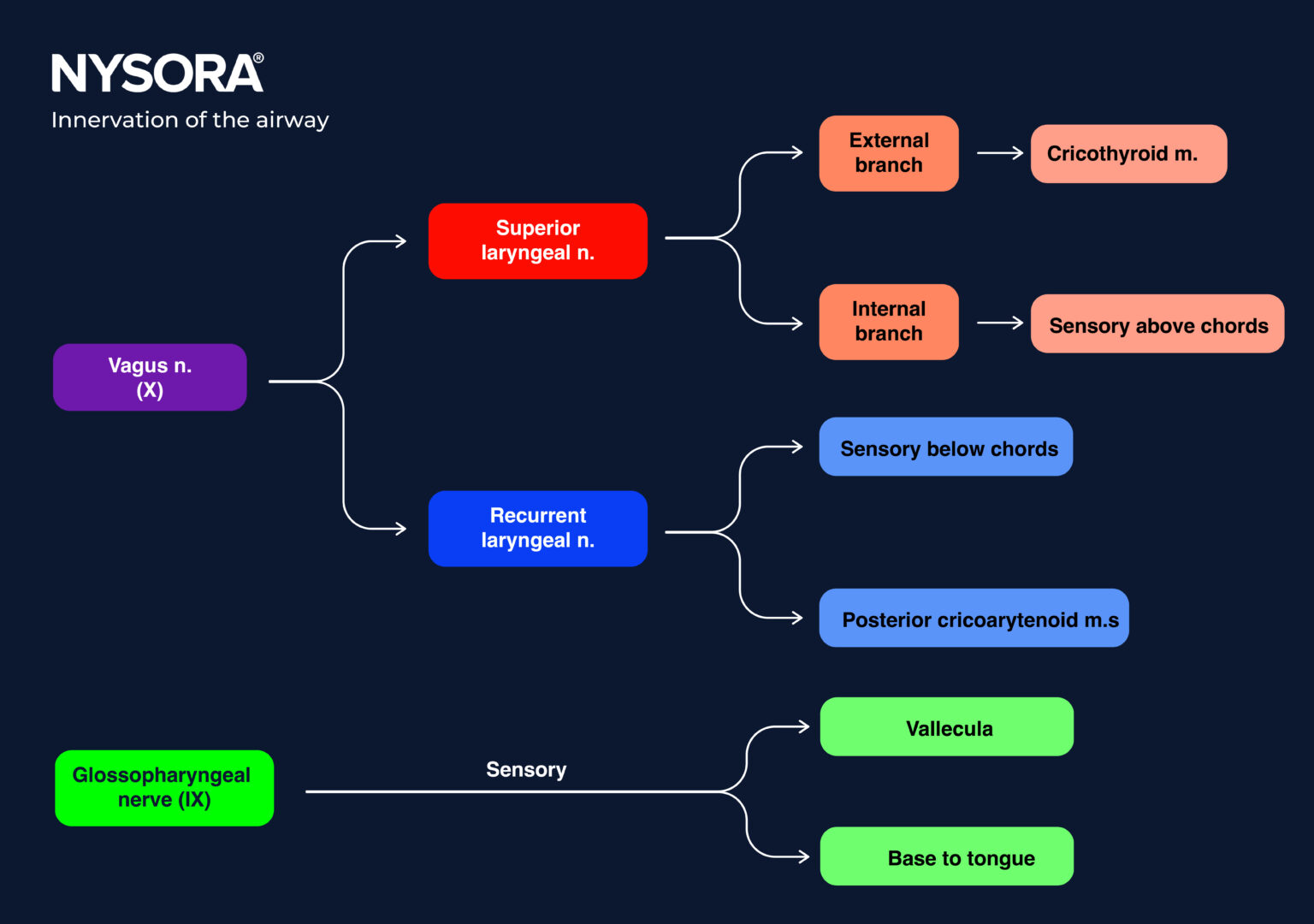
Innervation of the airway.
Blood supply
Branches of the external carotid artery, the facial artery, and the inferior thyroid artery primarily provide the blood supply to the upper airway.
- Nasal cavity
The nasal cavity receives blood supply from branches of both the internal carotid artery (sphenopalatine artery and posterior ethmoidal artery) and external carotid artery (superior labial artery, lateral nasal artery, and greater palatine artery).
- Pharynx
Blood supply to the pharynx is derived from branches of the external carotid artery (ascending pharyngeal artery) and branches of the facial artery (ascending palatine artery).
- Larynx
The blood supply to the larynx is predominantly from branches of the external carotid artery (superior laryngeal artery, a branch of the superior thyroid artery) and a branch of the inferior thyroid artery (the inferior laryngeal artery).
- Trachea
Blood supply to the trachea is mainly from branches of the inferior thyroid artery and small branches of the bronchial arteries.

Blood supply to the airway.
Ultrasound machine setup
Transducer:
- Suprahyoid (mouth floor): curvilinear
- Infrahyoid (neck): linear high frequency
Ultrasound preset: Vascular
Orientation: Index mark to the patient’s right side and transverse for the short axis view. Toward the head of the patient for the sagittal or long-axis view.
Depth:
- Suprahyoid (mouth floor): 5-10 cm
- Infrahyoid (neck): 3-4 cm
Patient position
- Position the patient supine with both arms next to the body.
- Always use the sniffing position; this is especially important for suprahyoid scanning.

Patient and transducer position for airway assessment.
Tip
Patient maneuvers can help to visualize anatomical structures better:
- Swallowing helps to visualize the esophagus
- Phonating helps identify the vocal cords
Landmarks
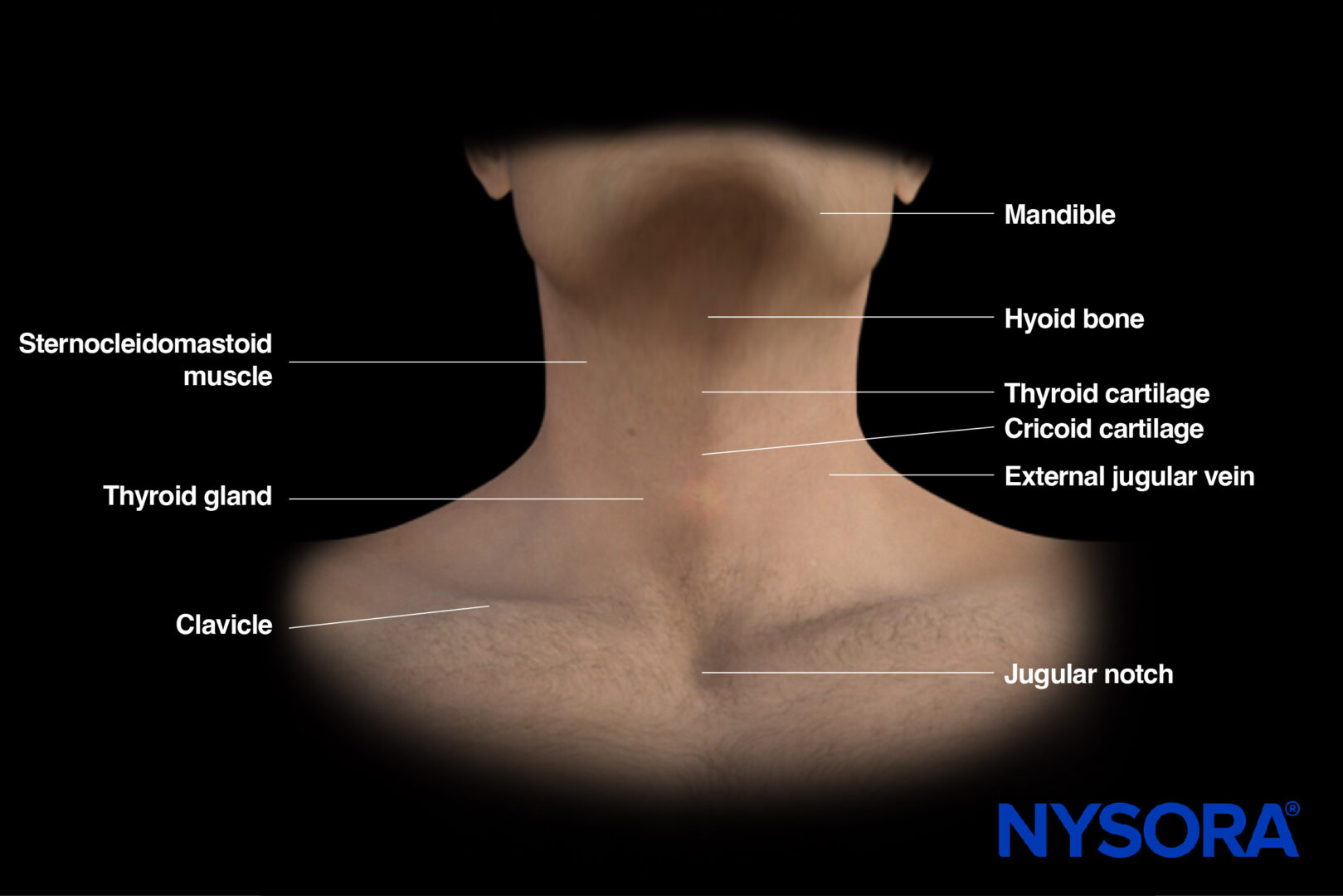
External landmarks for airway assessment.
Transducer position
Ultrasound can visualize structures such as the tongue, hyoid bone, epiglottis, thyrohyoid membrane, thyroid cartilage, cricothyroid membrane, cricoid cartilage, trachea, and the esophagus. Depending on the anatomical area of interest, different transducer positions are used:
Suprahyoid area
Here, the sagittal orientation is the standard for scanning. The index mark is always oriented toward the patient’s head.

Position 1: Suprahyoid sagittal view.
Infrahyoid area
Both the sagittal (longitudinal) and the transverse (axial) approach are used for infrahyoid scanning and position the transducer on the midline of the neck.
- Sagittal position: also called the ‘String of pearls’ technique. This dynamic scan starts caudally at the level of the trachea and requires you to slide the transducer cranially. The index mark aims toward the head of the patient.

Position 2: Infrahyoid sagittal view.
- For the transverse position, the index mark aims toward the right side of the patient, and different levels can be scanned from cranial to caudal:
- Hyoid bone
- Thyrohyoid membrane
- Thyroid cartilage
- Cricothyroid membrane
- Cricoid cartilage
- Trachea
Positions 3-8: Infrahyoid transverse view.
Scanning
Suprahyoid area
Place the transducer longitudinally on the skin surface, just below the mandible and above the hyoid bone. The hyoid bone is seen on the right of the screen as a narrow curved structure, causing an acoustic shadow together with the mentum on the left side of the screen. Underneath the mylohyoid and geniohyoid muscles, the tongue is seen and appears fan-shaped, with intrinsic muscles that give a typically striated appearance. The hyperechoic line deep in the image corresponds to the air-tissue interface of the tongue.
This view can be used for oral assessment and airway measurements to predict difficult airway procedures.
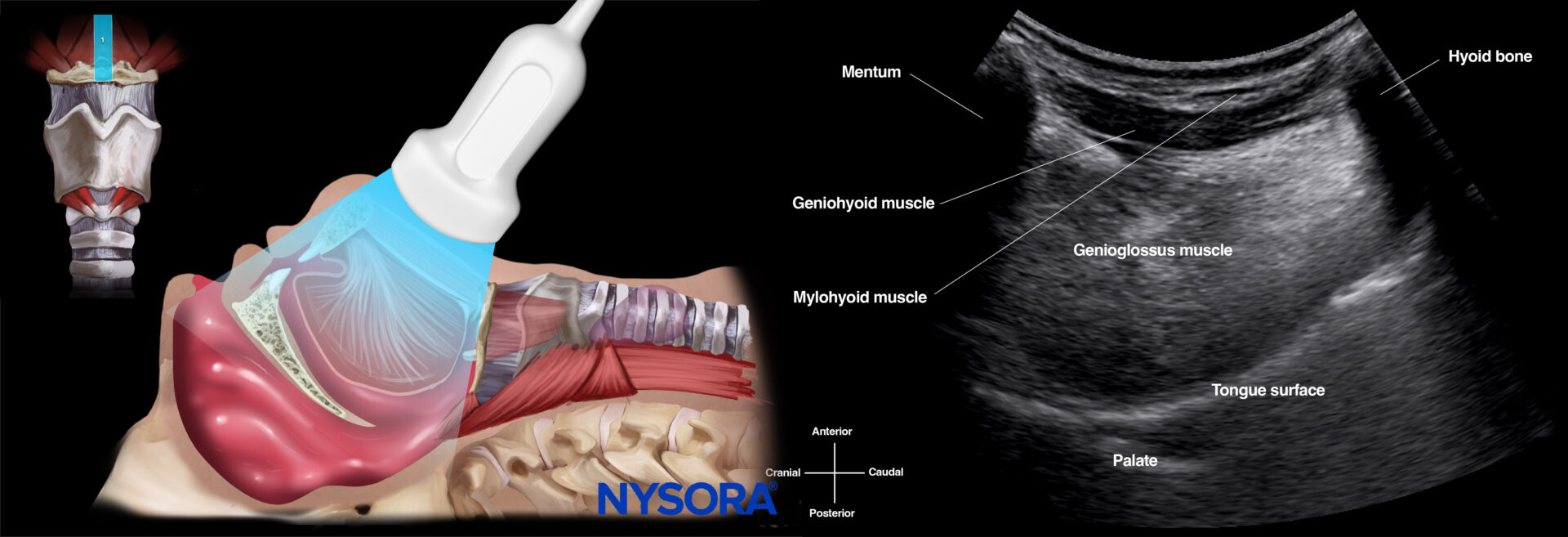

Ultrasound and Reverse Ultrasound Anatomy: Suprahyoid area.
Note
It is important to understand that air in the airway creates acoustic shadowing and reverberation artifacts, limiting the penetration of ultrasound waves into deeper tissues. Therefore, the hyperechoic line observed in all images corresponds to air-tissue interfaces.
Infrahyoid area – Sagittal
Long-axis scanning of the upper airway is often called the ‘String of pearls’ technique because the sonographic appearance of the tracheal rings resembles a pearl necklace.
For this technique, however, you start scanning with the transducer in the transverse position at the sternal notch to define the tracheal rings and the midline. In the short-axis view, the trachea appears as a horseshoe-shaped structure. Position the ultrasound transducer in the middle of the tracheal ring, and rotate it 90 degrees (indicator to the head of the patient).
The tracheal rings are dark hypoechoic structures with a ‘pearl-like’ structure. When sliding the ultrasound transducer cranially, the cricoid is the first larger, elongated, hypoechoic ‘pearl.’ Moving more cranially, you can find the thyroid cartilage with an even more elongated appearance. The hyperechoic cricothyroid membrane connects the thyroid cartilage with the cricoid cartilage. More cranially, the hyoid bone can be found with the thyrohyoid membrane connecting the hyperechoic hyoid bone and the thyroid cartilage. In this view, the epiglottis can also be seen as a hypoechoic longitudinal curvilinear structure.
The following positions can be obtained from caudal to cranial in the infrahyoid sagittal view:
- Tracheal rings position (‘string of pearls’)
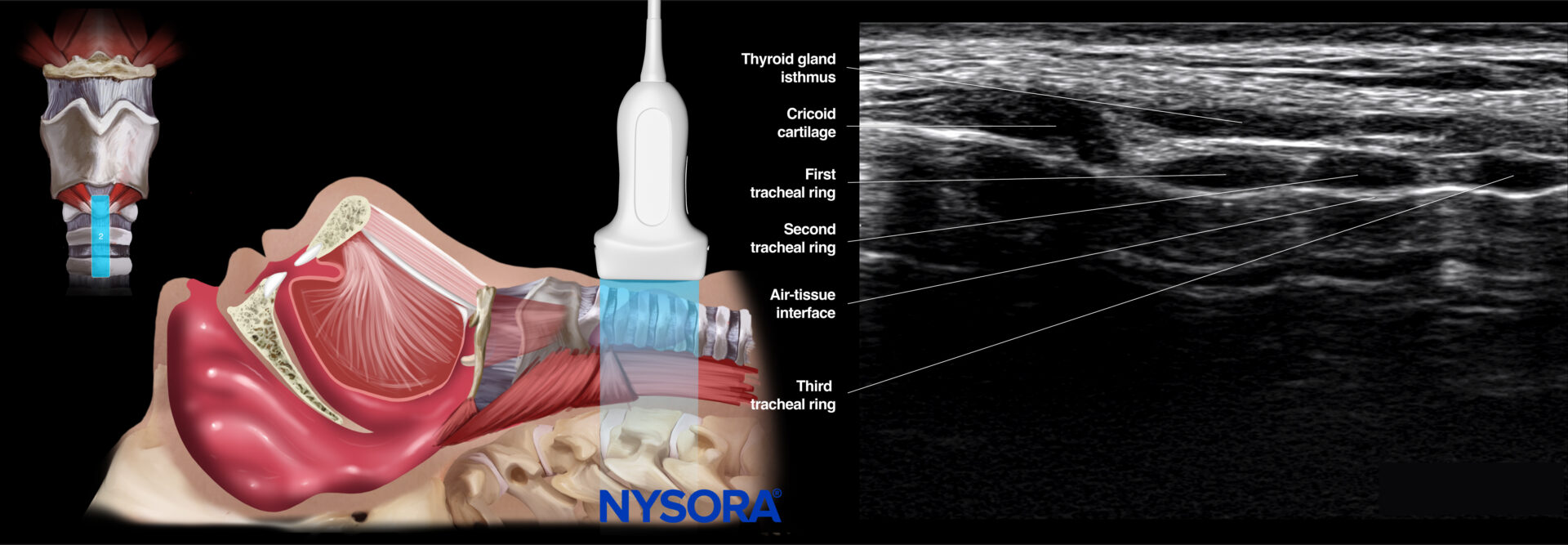
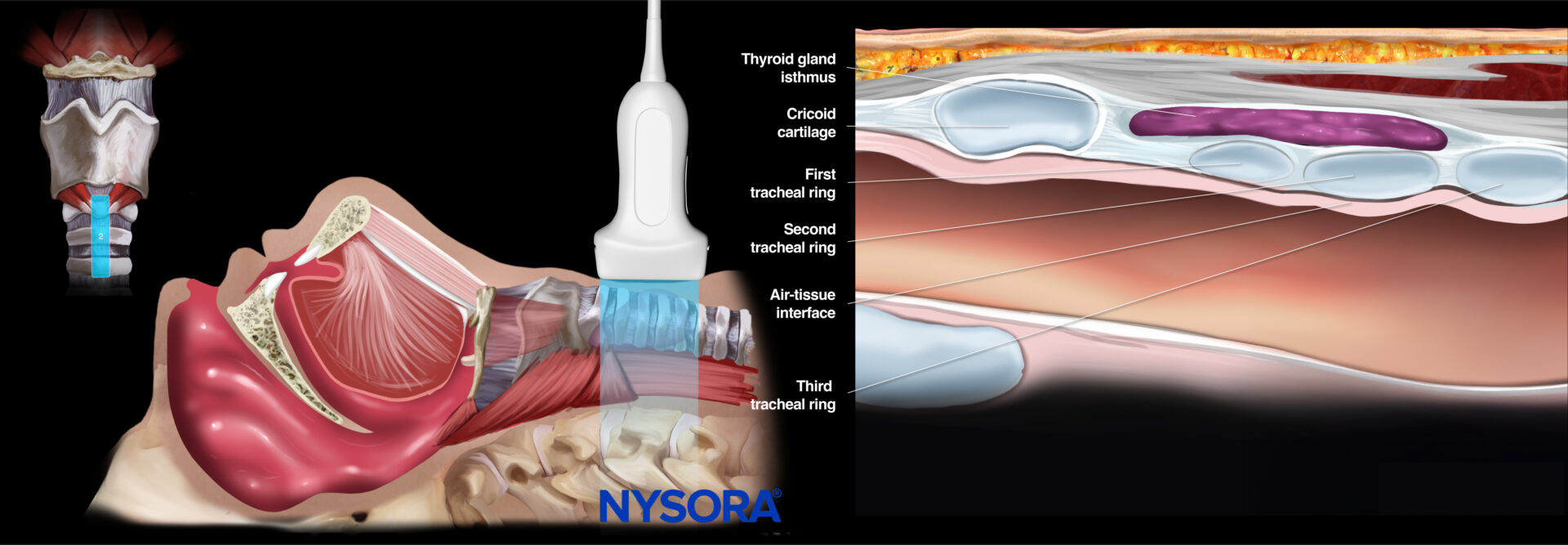
Ultrasound and Reverse Ultrasound Anatomy: Tracheal rings.
- Cricoid position
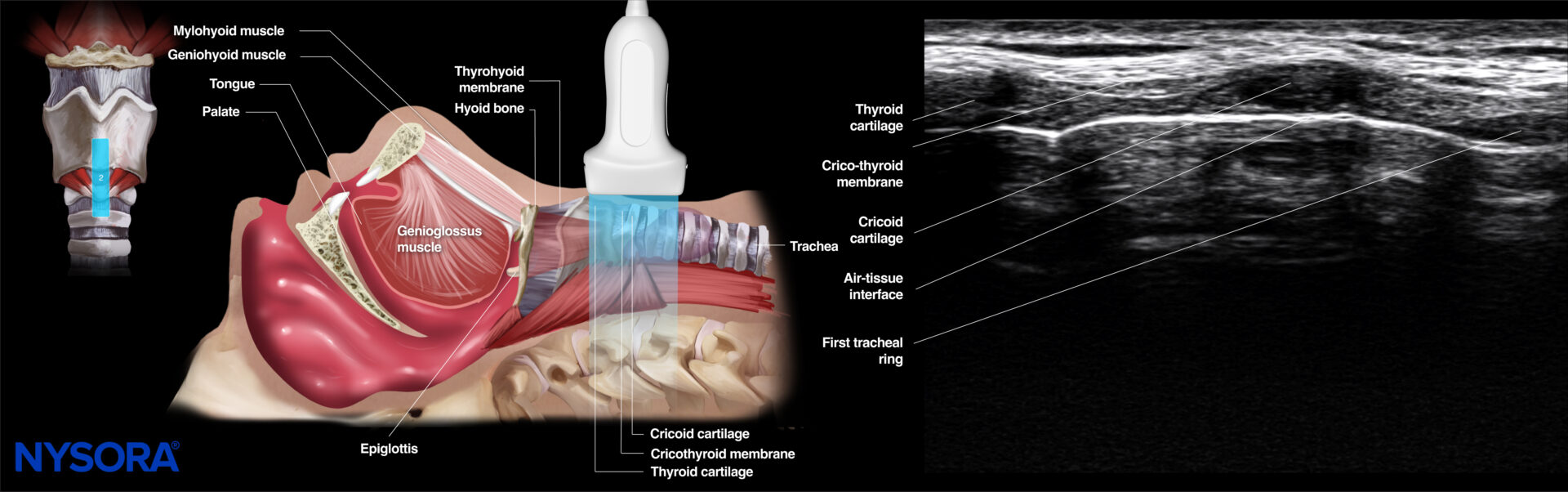
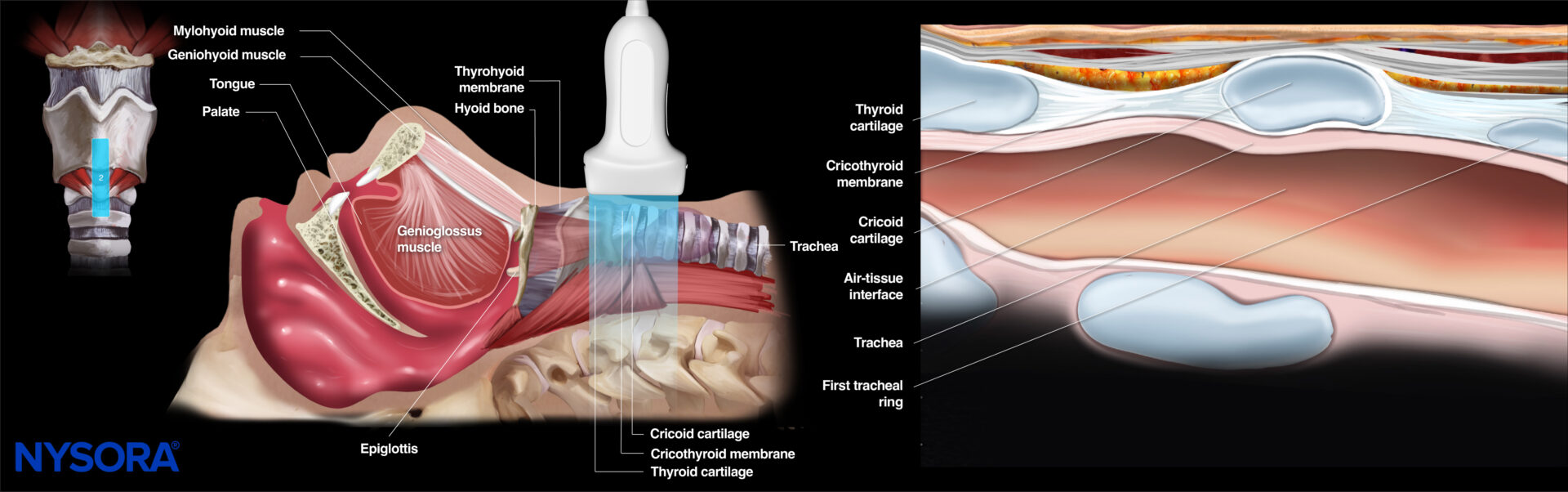
Ultrasound and Reverse Ultrasound Anatomy: Cricoid cartilage.
- Hyoid position

Ultrasound and Reverse Ultrasound Anatomy: Hyoid bone.
Infrahyoid area – Transverse
The infrahyoid portion of the upper airway can be visualized in the short axis by placing the transducer transversely at different levels or anatomical positions starting from cranial to caudal:
- Hyoid bone
- Thyrohyoid membrane
- Thyroid cartilage
- Cricothyroid membrane
- Cricoid cartilage
- Trachea
Note
Scanning is often started just above the hyoid bone until the typical sonographic shape of the hyoid bone is recognized. It can then be used as a reference point for the more caudal evaluation of anatomical structures.
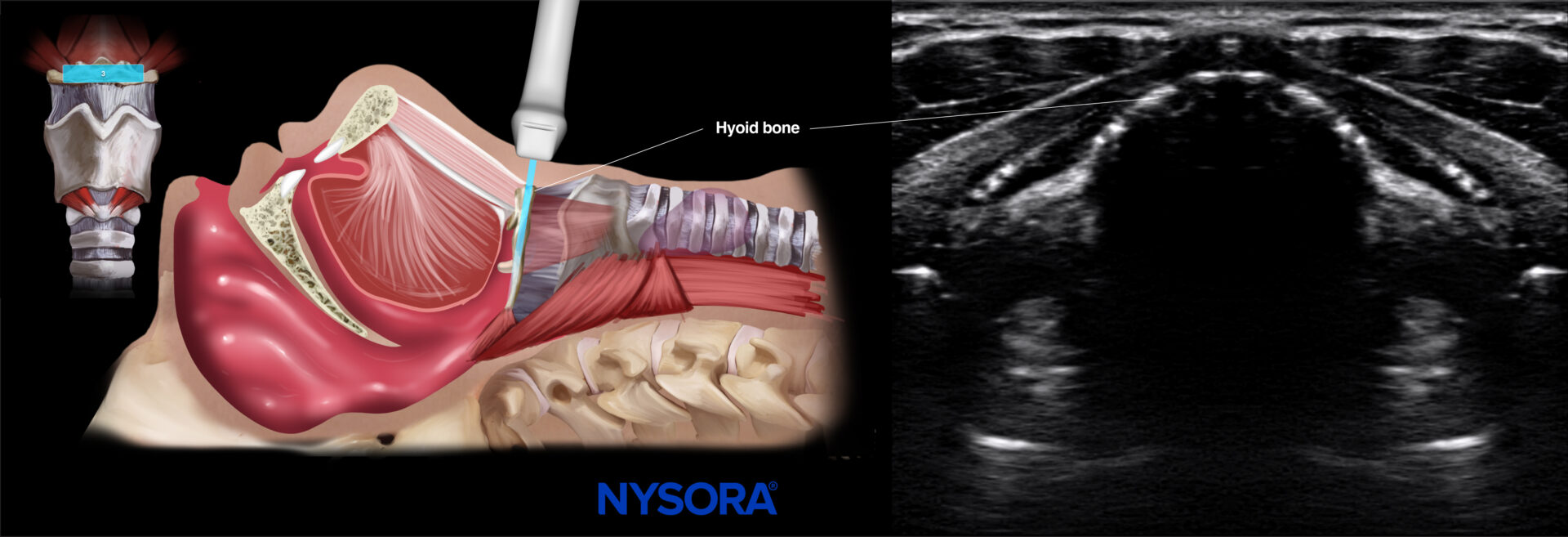
- Hyoid bone
To identify the hyoid bone, position the ultrasound transducer at the middle of the mentum (suprahyoid) in a transverse orientation and slide the ultrasound transducer more caudally. The hyoid bone is the first bony structure you will encounter. It can be identified as a linear hyperechoic inverted wide U-shaped structure with two greater horns (cornua) and a body.
The hyoid bone makes the anatomical distinction between the supra- and infrahyoid views. The suprahyoid view can be used for airway measurements to predict difficult airway procedures, while the infrahyoid views have other utility for airway management.

Ultrasound and Reverse Ultrasound Anatomy: Hyoid bone.
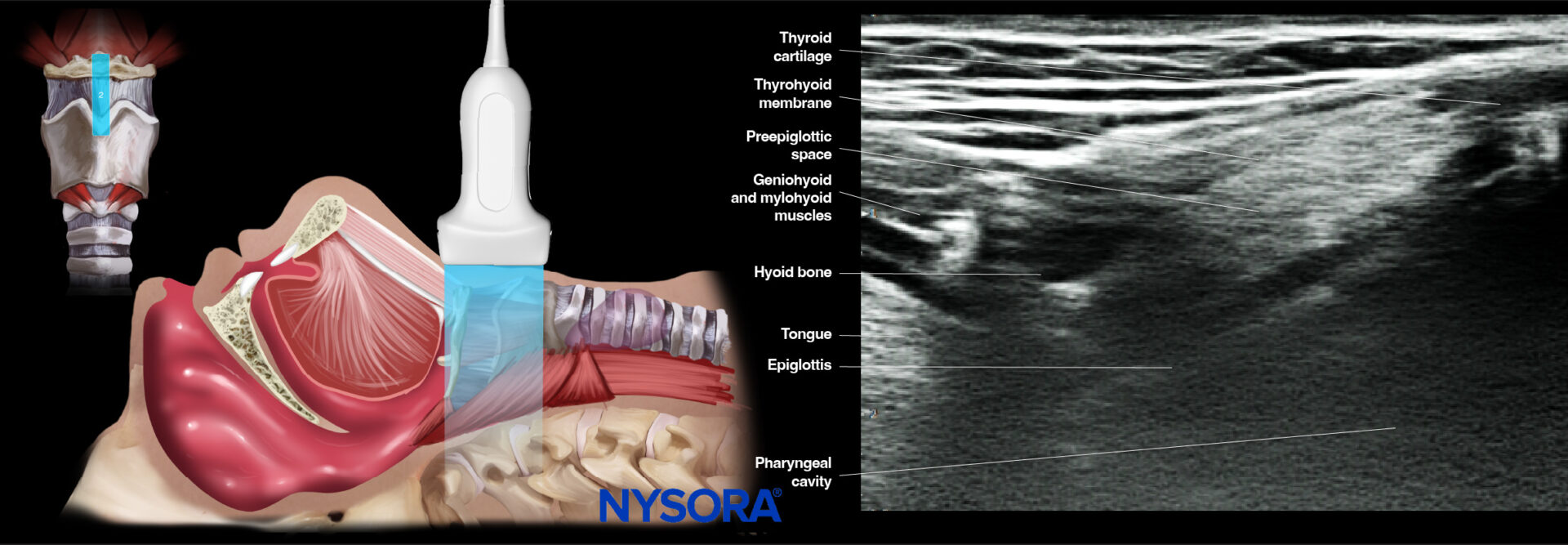
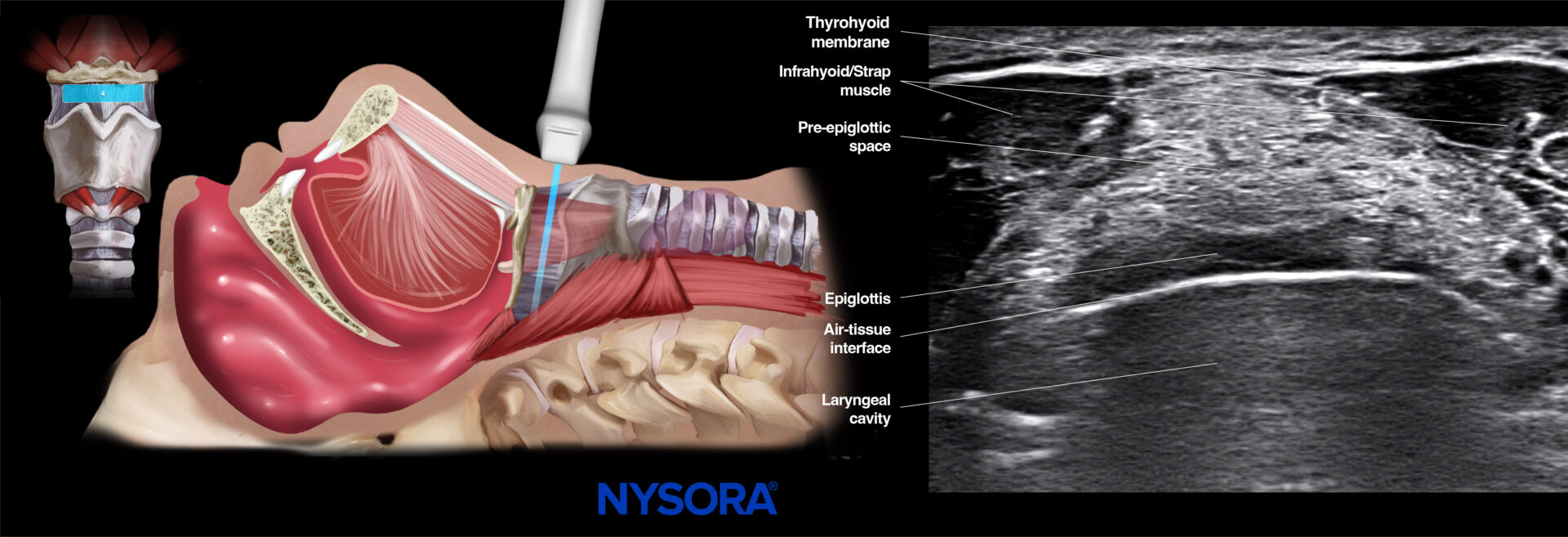
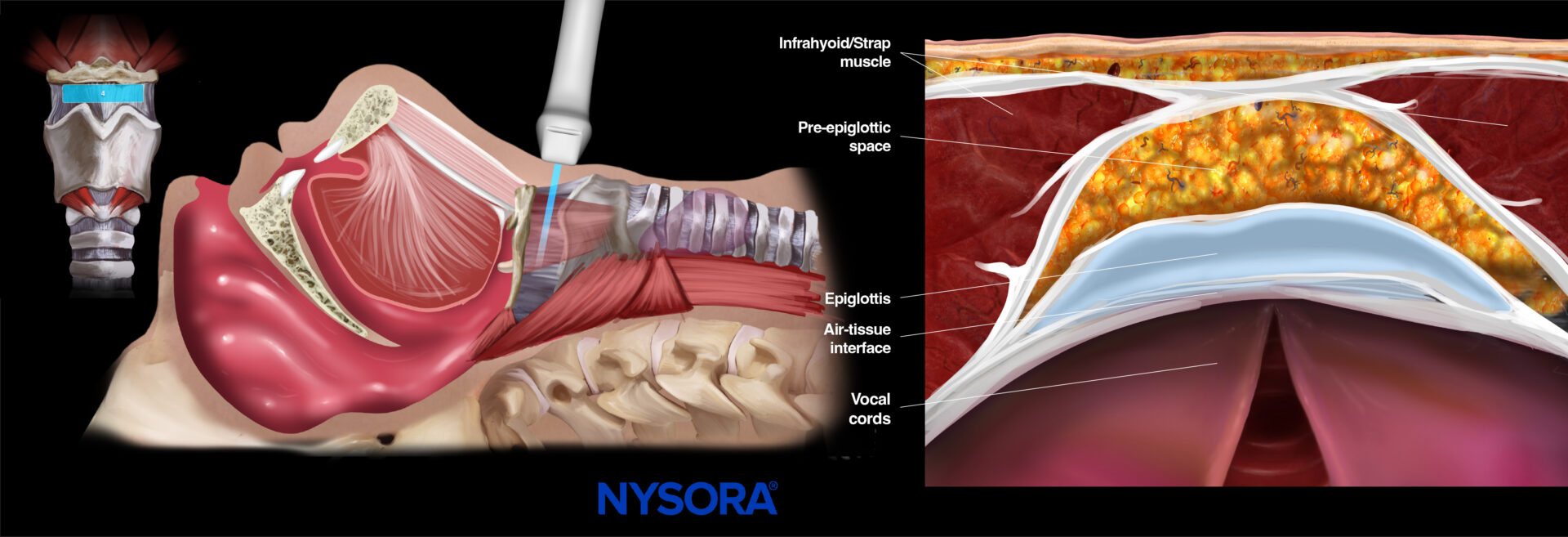
- Thyrohyoid membrane
Scan more caudally from the hyoid bone to meet the thyrohyoid membrane just above the thyroid cartilage. The thyrohyoid membrane can be identified as a hyperechoic horizontal line. Deeper to the thyrohyoid membrane, the infrahyoid muscles are seen on both sides of the screen. More posteriorly, the epiglottis appears as a hypoechoic curvilinear structure with a hyperechoic pre-epiglottic space that consists of adipose tissue.
If epiglottitis is suspected, the thyrohyoid membrane view can be used for epiglottis assessment.
Note
The infrahyoid muscles, or strap muscles, are a group of four pairs of muscles in the anterior part of the neck: the sternohyoid, sternothyroid, thyrohyoid, and omohyoid muscles.
Ultrasound and Reverse Ultrasound Anatomy: Thyrohyoid membrane.
- Thyroid cartilage
Next and more caudal, at the level of the thyroid prominence of the neck, the thyroid cartilage is seen as a hypoechoic inverted V-shaped or triangular structure. The angle of the triangle gets less steep more caudally. Posterior to the thyroid cartilage, the vocal cords appear as a hypoechoic triangle with a central shadow, delineated by the hyperechoic vocal ligaments that move toward the midline when the patient is asked to phonate. The more hyperechoic false vocal cords lie parallel and cranial to the true vocal cords and don’t move during phonation. The arytenoid cartilages are deep to the vocal cords and appear hyperechoic with shadowing.
This thyroid view can be used for vocal cord function assessment.
Note
The thyroid cartilage angle is more prominent in males.
![]()
Ultrasound and Reverse Ultrasound Anatomy: Thyroid cartilage.
- Cricothyroid membrane
Thereafter, more caudally to the hypoechoic inverted triangular-shaped thyroid cartilage, the cricothyroid membrane can be identified as a thin hyperechoic horizontal line with bright reverberation artifacts due to the air-tissue interface. The thyroid and cricoid cartilage are seen on both sides of the cricothyroid membrane underneath the infrahyoid muscles.
This view can localize the cricothyroid membrane and any possible overlying structures for emergency airways.
![]()
Ultrasound and Reverse Ultrasound Anatomy: Cricothyroid membrane.
Notes
- An alternative scanning technique to identify the cricothyroid membrane for emergency airway in case of short neck or limited neck mobility is the ‘TACA’ technique (Thyroid-Airline-Cricoid-Airline). The transducer is placed in a transverse position at the level where you can palpate the thyroid cartilage. Here, you see an SA view of thyroid cartilage as a hypoechoic V-shaped to triangular structure. Moving the transducer more caudally, you recognize the cricothyroid membrane as a hyperechoic bright white line. Further caudally, the cricoid cartilage is seen as a hypoechoic C-shaped structure.
- Use the borders of the hypoechoic thyroid and cricoid cartilage as a landmark if you can not identify the hyperechoic cricothyroid membrane.
- Power Doppler can assess vascular structures close to the cricothyroid membrane.
- Cricoid cartilage
When scanning further down, the cricoid cartilage appears as a thick, hypoechoic, and C-shaped structure with bright reverberation artifacts due to the air-tissue interface.
![]()
Ultrasound and Reverse Ultrasound Anatomy: Cricoid cartilage.
Note
Because of age-related calcification of the cricoid cartilage, the acoustic shadow can almost completely obstruct the air-tissue interface.
- Trachea
Lastly, more distal, at the level of the suprasternal notch, the trachea is seen as inverted hypoechoic U-shaped rings with bright reverberation artifacts due to the air-tissue interface. Slightly more lateral to the trachea, the esophagus is visualized as a round (collapsed) muscular structure that lies posteriorly and usually slightly to the left of the trachea. The esophagus has a typical layered wall, differentiating serosal and mucosal layers. Peristaltic movement can be seen when swallowing. Anterior and lateral to the trachea, the thyroid gland can be seen with the isthmus and both lobes.
This view can be used to localize the ETT, guide its placement and depth, and measure the airway diameter.
![]()
Ultrasound and Reverse Ultrasound Anatomy: Trachea.
Notes
- If the esophagus lies directly posterior to the trachea, it will not be visible on ultrasound. In these cases, slide the transducer to the left of the trachea at the level of the first tracheal ring and angle medially to scan behind the trachea.
- In this highly vascularized area, color or power Doppler can be used to assess vascular structures surrounding the trachea.
Overview
Sagittal positions

Transverse positions
![]()
Clinical updates
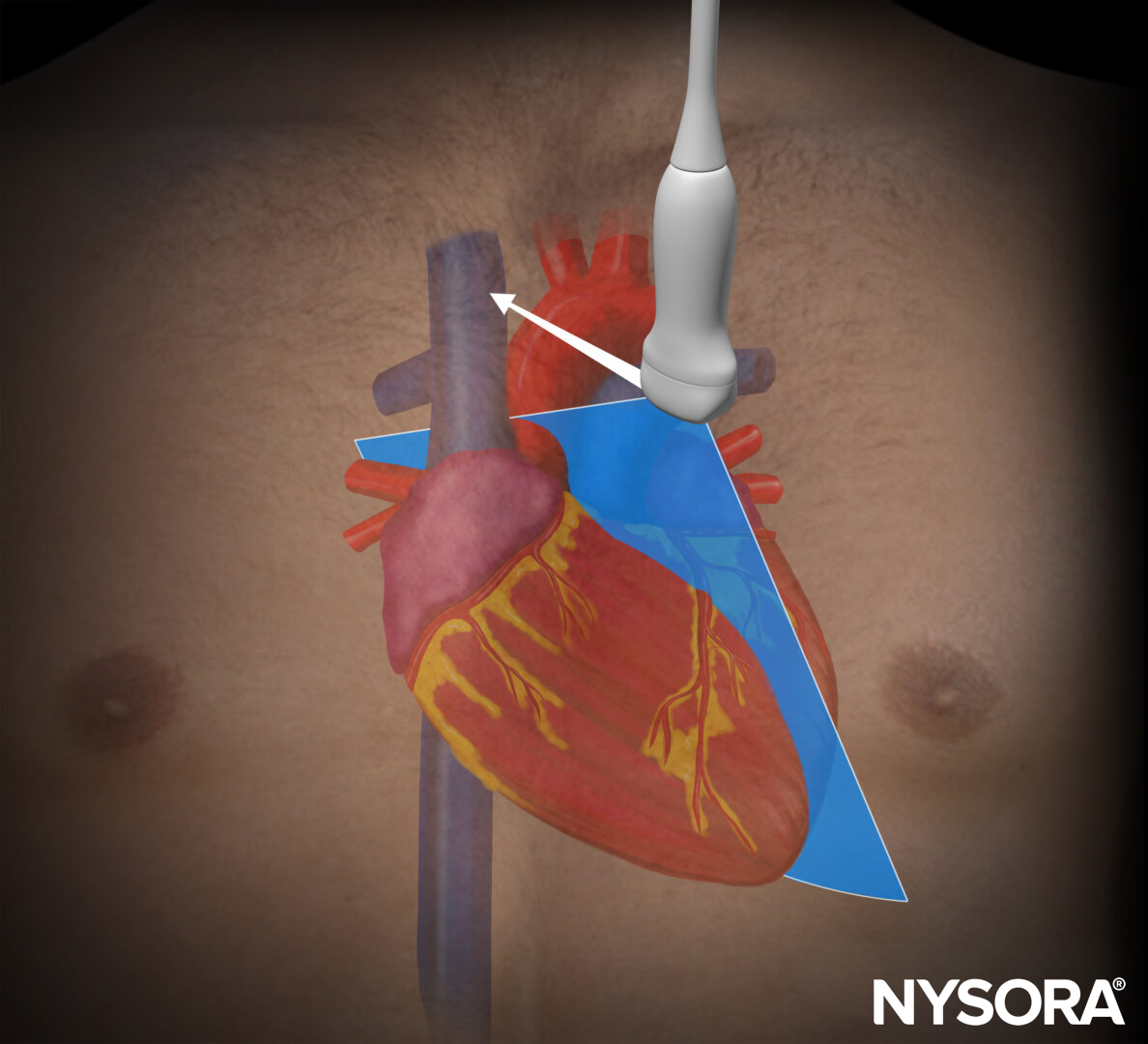
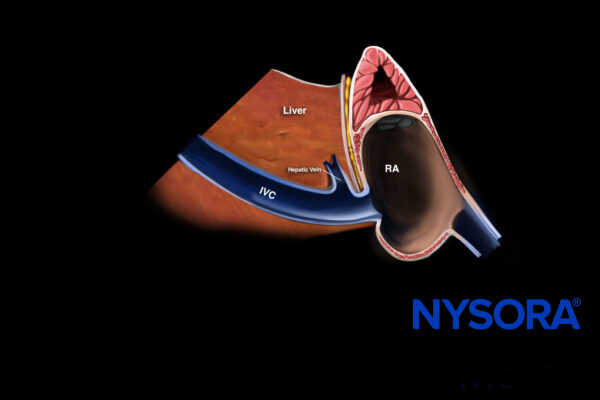
Khorsand et al. (Anesthesia & Analgesia, 2023) present a narrative review outlining a structured, system-based POCUS approach to the physiologically difficult airway, emphasizing pre-intubation assessment with RUSH (pump–tank–pipes), lung ultrasound (BLUE protocol), and gastric ultrasound to mitigate peri-intubation cardiovascular collapse, hypoxemia, and aspiration. They highlight that peri-intubation instability occurs in up to 42.6% of critically ill patients (INTUBE data) and propose integrating focused echocardiography (including subxiphoid-only EASy assessment), IVC evaluation for fluid responsiveness, RV strain recognition, and gastric antral cross-sectional area (>3.6 cm² indicating high aspiration risk) into an airway algorithm to guide tailored hemodynamic and respiratory optimization before tracheal intubation.
- Khorsand S, Chin J, Rice J, Bughrara N, Myatra SN, Karamchandani K. Role of Point-of-Care Ultrasound in Emergency Airway Management Outside the Operating Room. Anesth Analg. 2023;137(1):124-136.