Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About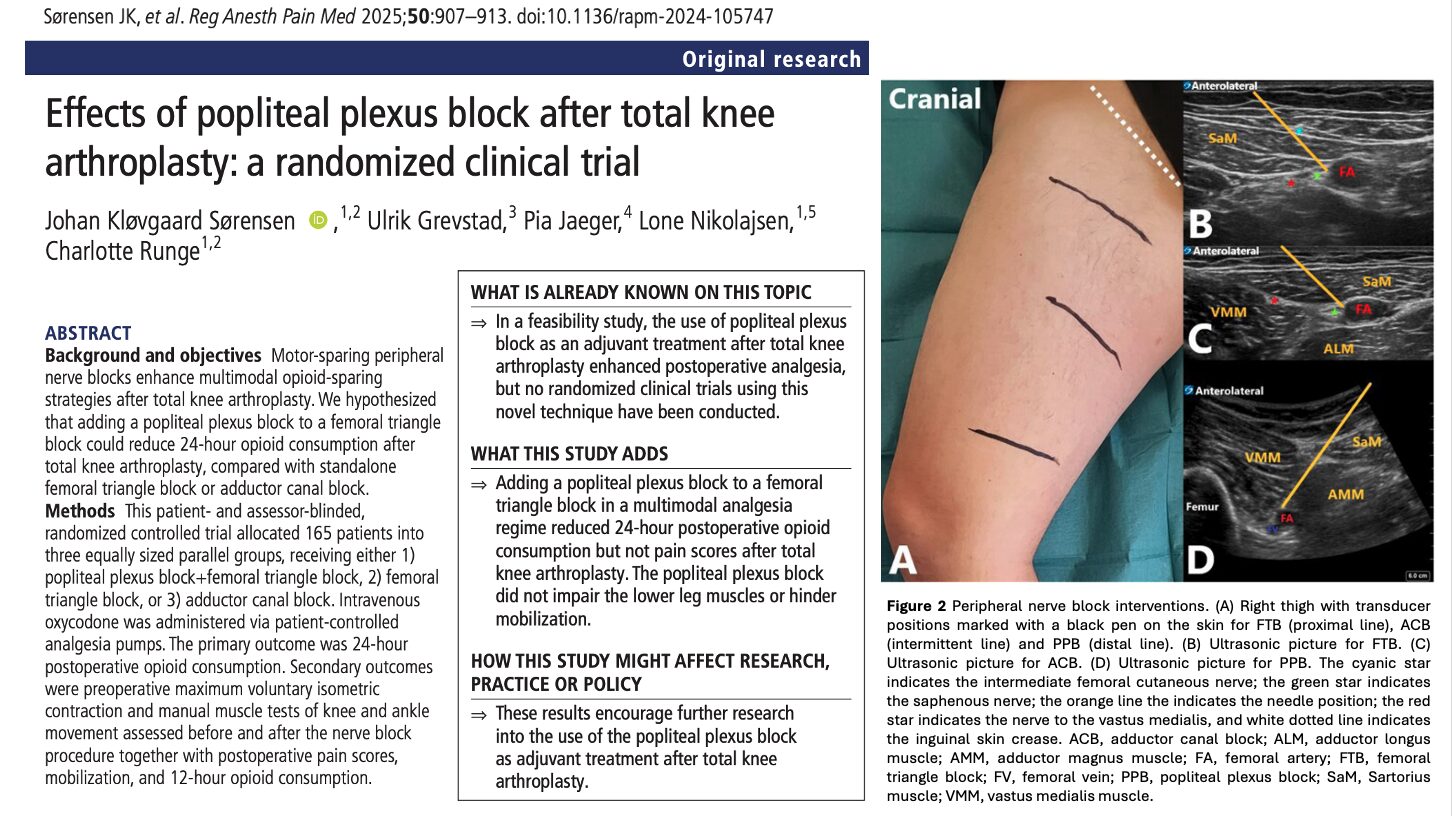





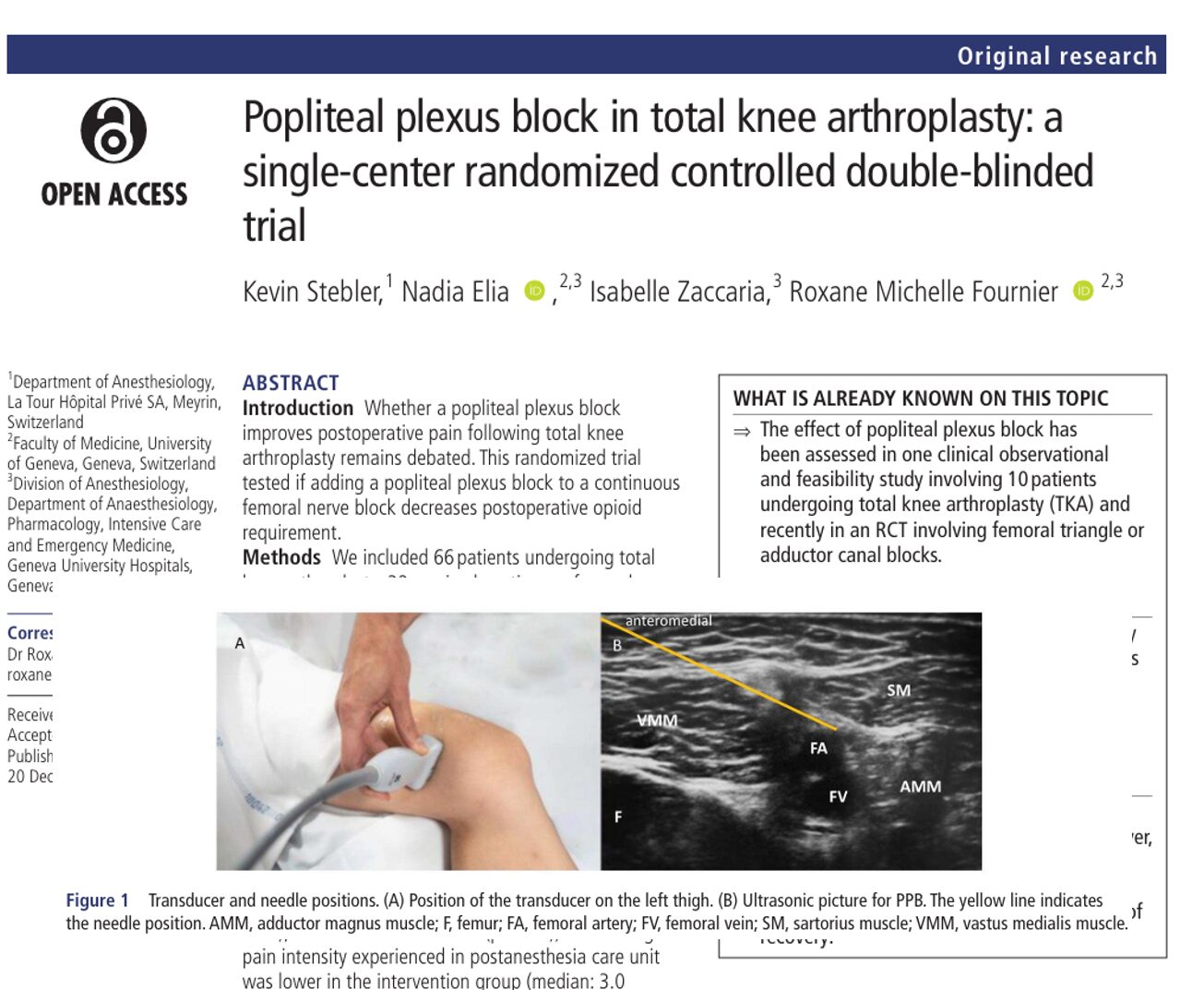
Effective postoperative analgesia after total knee arthroplasty (TKA) remains a major goal within enhanced recovery pathways. Motor-sparing strategies such as the adductor canal block (ACB) and femoral triangle block (FTB) have become standard because they provide anterior–medial knee analgesia while preserving quadriceps strength, supporting early mobilization and safer ambulation. Yet, many patients still experience posterior or intra-articular discomfort, reflecting the contribution of the popliteal plexus—formed by sensory branches of the tibial and posterior obturator nerves—to overall knee pain after TKA.
The popliteal plexus block (PPB) is a relatively new, motor-sparing technique that aims to selectively anesthetize these posterior sensory branches. Early feasibility data suggested that PPB might enhance analgesia without impairing lower-leg motor function, but no randomized trials had tested it within a real-world multimodal pathway. This study therefore evaluated whether adding PPB to FTB reduces early postoperative opioid consumption compared with standalone FTB or ACB.
The trial enrolled patients undergoing primary unilateral TKA under spinal anesthesia, all receiving standardized multimodal analgesia and unrestricted PCA oxycodone. By comparing PPB+FTB with FTB alone and ACB, the study provides the first randomized evidence on whether targeting the popliteal plexus meaningfully augments analgesia within a motor-preserving strategy.
Study objective and methods
The primary objective was to determine whether adding a popliteal plexus block to a femoral triangle block reduces 24-hour postoperative opioid consumption after TKA, compared with standalone FTB or ACB, while preserving motor function.
- Design: Patient- and assessor-blinded, randomized controlled trial (1:1:1).
- Setting: Silkeborg Regional Hospital, Denmark.
- Population: 165 adults undergoing primary unilateral TKA under spinal anesthesia.
- Groups:
- PPB + FTB (n = 55)
- FTB alone (n = 55)
- ACB alone (n = 55)
- Interventions: Ultrasound-guided PPB, FTB, or ACB; sham injections for blinding.
- Primary outcome: 24-hour IV oxycodone consumption.
- Secondary outcomes: 12-h opioid use, pain scores at rest & movement, MVIC, manual muscle testing, timed-up-and-go (TUG), mobilization, and block-related adverse events.
Key findings
-
PPB + FTB reduced opioid use at 24 hours
Patients receiving PPB + FTB used less IV oxycodone (median 6 mg) compared with FTB (10 mg) and ACB (12 mg). The between-group differences (−4 mg and −6 mg) were statistically significant (p < 0.01) and fall within ranges considered potentially clinically relevant.
-
No difference in pain scores
Despite lower opioid use, pain scores at rest and during knee flexion were similar across groups. Pain levels remained mild overall, likely reflecting effective multimodal therapy and free PCA access.
-
Motor strength and mobilization were preserved
Lower-leg motor function (MVIC and manual muscle testing) did not differ between groups. TUG performance and mobilization were also similar, confirming PPB did not impair distal motor function.
-
More opioid-free patients with PPB + FTB (post hoc)
Twelve patients in the PPB + FTB group required no opioids at all in the first 24 hours—compared with two in the FTB group and six in the ACB group.
Conclusion
Adding a popliteal plexus block to a femoral triangle block in patients undergoing TKA led to a statistically significant reduction in 24-hour opioid consumption compared with FTB or ACB alone, without worsening pain scores or compromising motor function. The technique appears to offer additional posterior/intra-articular coverage on top of standard motor-sparing anterior blocks, but in the context of effective multimodal analgesia, the absolute opioid reduction was modest and did not translate into lower pain ratings.
- Clarify the patient-centered impact of the observed opioid reduction, using anchors such as opioid-related side effects, sleep quality, and functional recovery.
- Explore optimal local anesthetic volumes and spread for PPB, including imaging or sensory mapping to better characterize coverage.
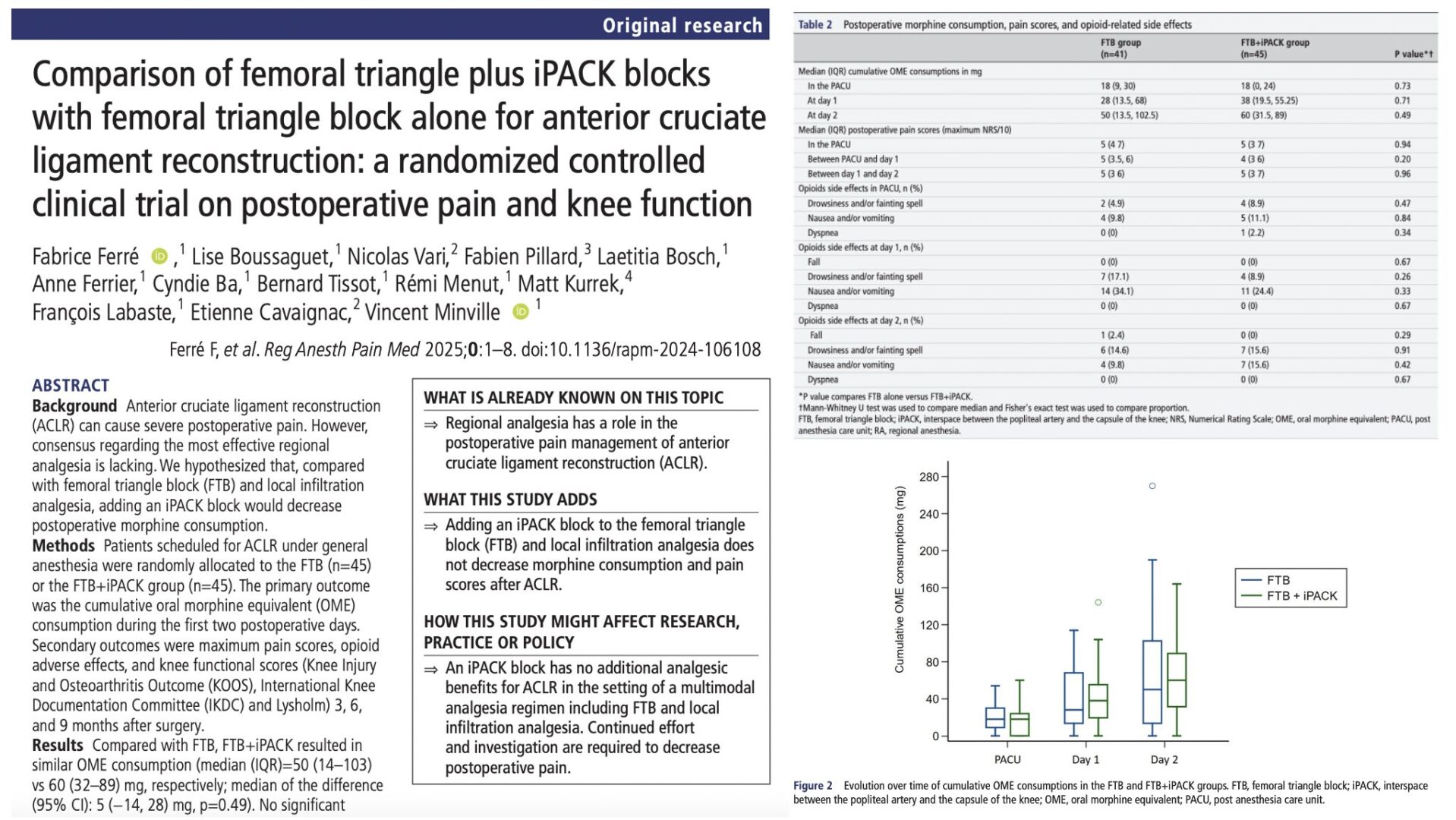
- Compare PPB + FTB directly with ACB + iPACK or with local infiltration analgesia–based strategies to understand where PPB fits in current practice.
- Evaluate PPB’s effect in higher-risk or high-pain phenotypes (e.g., opioid-tolerant patients, severe baseline pain) where incremental opioid-sparing could be more clinically impactful.
Clinical implications
This trial suggests that adding a popliteal plexus block to a femoral triangle block can meaningfully reduce early opioid use after TKA without compromising quadriceps strength or mobilization—a key requirement in modern recovery protocols. Although absolute opioid savings were modest and did not translate into lower pain scores, the finding that more patients remained entirely opioid-free at 24 hours indicates a potential benefit for individuals sensitive to opioid-related side effects.
The PPB may therefore serve as a useful adjunct within multimodal, motor-sparing analgesic pathways, particularly for patients in whom opioid minimization is clinically important. However, given that overall pain control remained similar across groups, routine adoption of PPB for all TKA patients is not yet supported, and its role should be individualized until larger or comparative studies clarify where it best fits relative to other posterior knee–targeting techniques such as iPACK or high-volume ACB.
Clinical pearls
- PPB + FTB reduced 24-h oxycodone use vs FTB and ACB.
- Pain scores remained similar across groups—overall mild.
- No meaningful impact on quadriceps or distal leg strength.
- More patients were completely opioid-free at 24 h with PPB + FTB.
- Technique is promising but not yet ready as a universal standard.
Practical tip: If your TKA pathway already includes a femoral triangle or adductor canal block, consider PPB as an add-on for selected patients where even small opioid reductions are desirable and motor preservation is essential.
For more detailed information, refer to the full article in RAPM.
Sørensen JK. et al. Effects of popliteal plexus block after total knee arthroplasty: a randomized clinical trial. Reg Anesth Pain Med. 2025;50:907-913.
Download the Nerve Blocks App HERE for in-depth insights on the femoral triangle and adductor canal blocks. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!