Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About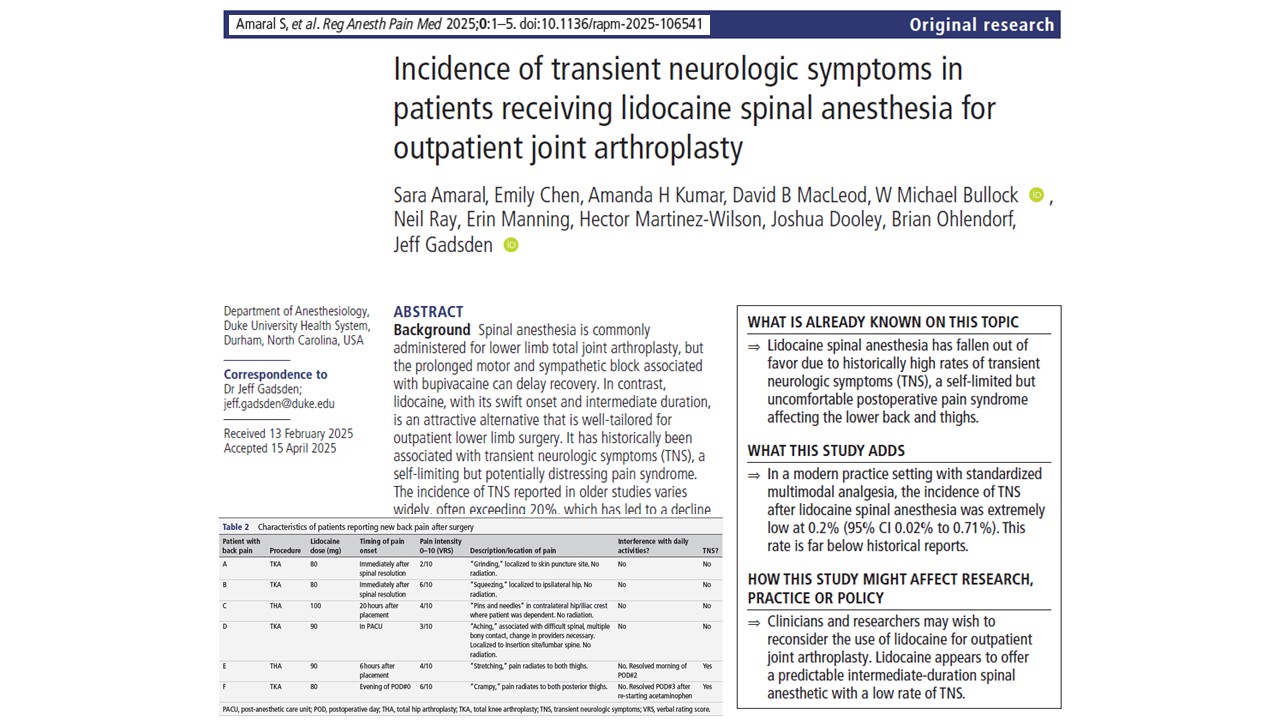





For decades, transient neurologic symptoms (TNS) have been one of the primary concerns limiting the use of lidocaine for spinal anesthesia. Early studies reported rates as high as 20–40%, leading many anesthesiologists to abandon intrathecal lidocaine in favor of longer-acting alternatives such as bupivacaine.
However, modern perioperative care has changed dramatically. Enhanced recovery protocols, multimodal analgesia, and outpatient joint replacement pathways have transformed postoperative patient management.
A new study by Amaral and colleagues in RAPM suggests that the historical concerns surrounding lidocaine spinal anesthesia may warrant reconsideration. In a retrospective review of more than 1,000 patients undergoing total hip and knee arthroplasty, investigators found an extremely low incidence of TNS following spinal lidocaine administration. Only two patients developed probable TNS, yielding an incidence of 0.2%. Both cases were mild and resolved completely within days.
The findings raise an important question: Has the risk profile of lidocaine spinal anesthesia changed in the era of modern multimodal analgesia?
Why transient neurologic symptoms remain important
Transient neurologic symptoms are characterized by new-onset pain involving the lower back, buttocks, or lower extremities following spinal anesthesia.
The syndrome typically develops within the first 24 hours after surgery and may present as:
- Lower back pain
- Buttock discomfort
- Pain radiating into the thighs
- Cramping sensations
- Stretching-type pain
- Musculoskeletal soreness without neurologic deficits
Importantly, TNS does not cause permanent nerve injury. Patients generally do not experience motor weakness, sensory loss, or lasting neurologic impairment.
Nevertheless, the condition can be distressing and may negatively affect recovery, mobility, and overall patient satisfaction.
Historically, TNS became strongly associated with spinal lidocaine. Numerous studies published during the 1990s reported widely varying incidence rates, ranging from approximately 4% to more than 40%, depending on patient population, surgical procedure, and study methodology. These reports substantially influenced anesthetic practice worldwide.
Why lidocaine fell out of favor
Lidocaine possesses several characteristics that make it attractive for spinal anesthesia.
Compared with longer-acting agents, it provides:
- Rapid onset of anesthesia
- Reliable surgical conditions
- Intermediate duration of action
- Faster motor recovery
- Earlier ambulation
- Potentially shorter recovery room stays
These characteristics are particularly appealing in ambulatory orthopedic surgery.
However, concerns regarding TNS dramatically reduced enthusiasm for spinal lidocaine. At the same time, reports of cauda equina syndrome associated with concentrated hyperbaric lidocaine formulations further damaged the drug’s reputation, despite the fact that TNS and cauda equina syndrome are fundamentally different conditions.
As a result, many clinicians shifted toward bupivacaine as their preferred spinal anesthetic.
Today, some anesthesiology textbooks still describe lidocaine as a drug that has largely disappeared from routine spinal anesthesia practice.
Why outpatient arthroplasty is changing the conversation
The growth of outpatient total joint replacement has created new challenges for anesthesiologists.
While bupivacaine remains highly effective, its prolonged duration can delay recovery.
Potential consequences include:
- Delayed ambulation
- Prolonged motor blockade
- Delayed voiding
- Orthostatic symptoms
- Longer post-anesthesia care unit stays
- Increased risk of unexpected overnight admission
These issues become increasingly important when same-day discharge is the goal.
In contrast, lidocaine’s duration of approximately 2.5 hours may better align with modern ambulatory surgical pathways.
This has prompted some centers to revisit the role of lidocaine in contemporary orthopedic anesthesia.
Study objective
The investigators sought to determine the modern incidence of transient neurologic symptoms following lidocaine spinal anesthesia in patients undergoing outpatient total hip and knee arthroplasty.
Specifically, they wanted to evaluate whether TNS rates remained consistent with historical reports or whether contemporary multimodal analgesic protocols had altered the clinical picture.
Study design and methods
Researchers conducted a retrospective review of a postoperative outcomes database at Duke University Health System.
The study included adult patients who:
- Underwent total knee arthroplasty
- Underwent total hip arthroplasty
- Received preservative-free 2% lidocaine spinal anesthesia
Patients receiving other spinal anesthetics or undergoing general anesthesia alone were excluded.
The review covered cases performed between August 2021 and May 2024.
Postoperative follow-up was conducted by telephone on postoperative days 2 or 3.
Importantly, the institution had incorporated specific TNS screening questions into its routine postoperative assessment process.
Patients were asked whether they experienced:
- New lower back pain
- New buttock pain
- Pain radiating into the legs
- Numbness
- Weakness
- Recovery limitations related to these symptoms
Investigators independently reviewed all reported symptoms to determine whether they were consistent with TNS.
Multimodal analgesia protocol
One of the most notable aspects of the study was the extensive use of multimodal analgesia.
Most patients received a standardized regimen that included:
Preoperative and postoperative medications
- Acetaminophen
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
Intraoperative medications
- Intravenous ketamine
- Dexamethasone
Regional anesthesia techniques
- Peripheral nerve blocks, when appropriate
Rescue analgesics
- Oxycodone or tramadol as needed
Compliance with prescribed medications was high throughout the cohort.
The authors hypothesized that this aggressive multimodal approach may have influenced the incidence and severity of TNS.
Key findings
- TNS was remarkably uncommon
A total of 1,026 patients initially met study criteria.
After excluding 15 patients lost to follow-up, investigators analyzed 1,011 complete patient records.
Among those patients:
- Six reported new non-surgical back or lower extremity pain
- Four cases were determined not to represent TNS
- Two cases were classified as probable TNS
The final incidence was 0.2% (95% confidence interval 0.02%–0.71%)
This rate is dramatically lower than historical estimates.
- Symptoms were mild and self-limited
Both patients diagnosed with TNS experienced symptom onset shortly after spinal block resolution.
One patient developed:
- Stretching-type pain
- Radiation into both thighs
- Symptom onset approximately six hours after surgery
Symptoms resolved completely by postoperative day two.
The second patient reported:
- Cramping pain
- Radiation into both posterior thighs
- Symptom onset on the evening of surgery
After restarting scheduled acetaminophen, symptoms resolved within 24 hours.
Neither patient experienced functional limitations.
- No major neurologic complications occurred
Investigators found no evidence of:
- Prolonged motor blockade
- Prolonged sensory blockade
- Cauda equina syndrome
- Local anesthetic systemic toxicity
- Persistent neurologic injury
- Significant spinal anesthesia complications
These findings further support the overall safety profile observed in the study population.
Why were rates so much lower than historical reports?
One of the most important questions raised by this study is why TNS rates were dramatically lower than those reported decades ago.
Based on historical literature, investigators estimated they should have observed approximately 141 TNS cases in a cohort of this size.
Instead, only two cases occurred.
Several explanations may account for this discrepancy.
Modern multimodal analgesia
Perhaps the most obvious difference between contemporary and historical practice is the widespread use of multimodal pain management.
Patients in the late 1990s often did not receive:
- Scheduled acetaminophen
- Routine NSAIDs
- Intravenous ketamine
- Dexamethasone
- Enhanced recovery pathways
Because NSAIDs and acetaminophen are commonly used to treat TNS, it is possible that these medications may also help prevent symptom development or reduce symptom severity.
Different surgical populations
Previous research identified several risk factors for TNS, including:
- Knee arthroscopy
- Lithotomy positioning
Neither of these situations was common in the present study.
Joint replacement procedures involve different positioning requirements that may reduce stress on lumbar and posterior thigh structures.
Enhanced recovery pathways
Modern arthroplasty pathways incorporate multiple strategies designed to improve recovery and reduce postoperative pain.
These include:
- Earlier mobilization
- Standardized analgesia
- Better patient education
- Regional anesthesia optimization
Collectively, these improvements may contribute to lower TNS rates.
Understanding the possible mechanism of TNS
The exact mechanism underlying TNS remains controversial.
Despite its name, evidence suggests that TNS does not involve actual nerve root injury.
One leading theory proposes that profound muscle relaxation following lidocaine spinal anesthesia may alter the normal curvature of the lumbar spine.
This could lead to:
- Increased stretching of lumbar myofascial tissues
- Posterior thigh tension
- Musculoskeletal discomfort resembling delayed-onset muscle soreness
Several observations support this theory:
- Symptoms are temporary
- Neurologic deficits are absent
- Anti-inflammatory medications are often effective
- Certain patient positions increase risk
The current findings are consistent with the concept that TNS may represent a transient musculoskeletal phenomenon rather than true neurotoxicity.
Clinical interpretation
Although this was not a randomized clinical trial, the findings provide important insights for practicing anesthesiologists.
Historical concerns may deserve re-evaluation
The extremely low incidence observed in this study challenges long-standing assumptions regarding spinal lidocaine.
While historical data cannot be ignored, contemporary outcomes appear substantially different from those reported several decades ago.
Lidocaine may fit modern outpatient surgery better
As same-day discharge becomes increasingly common, the duration of anesthesia becomes more important.
Compared with bupivacaine, lidocaine offers:
- Faster recovery
- Earlier ambulation
- More predictable discharge timelines
- Shorter duration of motor blockade
These characteristics may make it particularly attractive for ambulatory arthroplasty programs.
Safety should remain multimodal
The study should not be interpreted as evidence that TNS no longer exists.
Rather, it highlights the importance of modern perioperative care and multimodal pain management strategies.
Careful patient selection, optimized analgesia, and appropriate anesthetic technique remain essential.
Important limitations
The authors acknowledge several limitations.
Retrospective design
The study was observational and retrospective, limiting causal conclusions.
No comparison group
Investigators did not directly compare lidocaine with bupivacaine, mepivacaine, or chloroprocaine.
Medication adherence variability
Although compliance was generally high, researchers could not guarantee perfect adherence to prescribed postoperative medications.
Single-center experience
Results may not be generalizable to all institutions or patient populations.
Despite these limitations, the study is among the largest contemporary evaluations of lidocaine spinal anesthesia in patients undergoing joint arthroplasty.
Conclusion
This large retrospective study suggests that transient neurologic symptoms following lidocaine spinal anesthesia may be far less common than historical reports have suggested.
Among more than 1,000 patients undergoing total hip and knee arthroplasty, investigators observed only two cases of probable TNS, corresponding to an incidence of just 0.2%. Both cases were mild, self-limited, and resolved completely within days. No major neurologic complications were identified.
While additional prospective studies are needed, these findings challenge long-standing concerns regarding spinal lidocaine and suggest that, in the setting of modern multimodal analgesia, lidocaine may represent a safe and effective option for outpatient joint replacement surgery.
For more information, refer to the full article by Amaral et al. in Regional Anesthesia & Pain Medicine.
Amaral S, Chen E, Kumar AH, MacLeod DB, Bullock WM, Ray N, Manning E, Martinez-Wilson H, Dooley J, Ohlendorf B, Gadsden J. Incidence of transient neurologic symptoms in patients receiving lidocaine spinal anesthesia for outpatient joint arthroplasty. Reg Anesth Pain Med. 2026 May 5;51(5):579-583.
Read more about spinal anesthesia in our Regional Anesthesiology Module on NYSORA 360 on NYSORA360 – an essential learning resource for residents with practical, up-to-date guidance.