Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About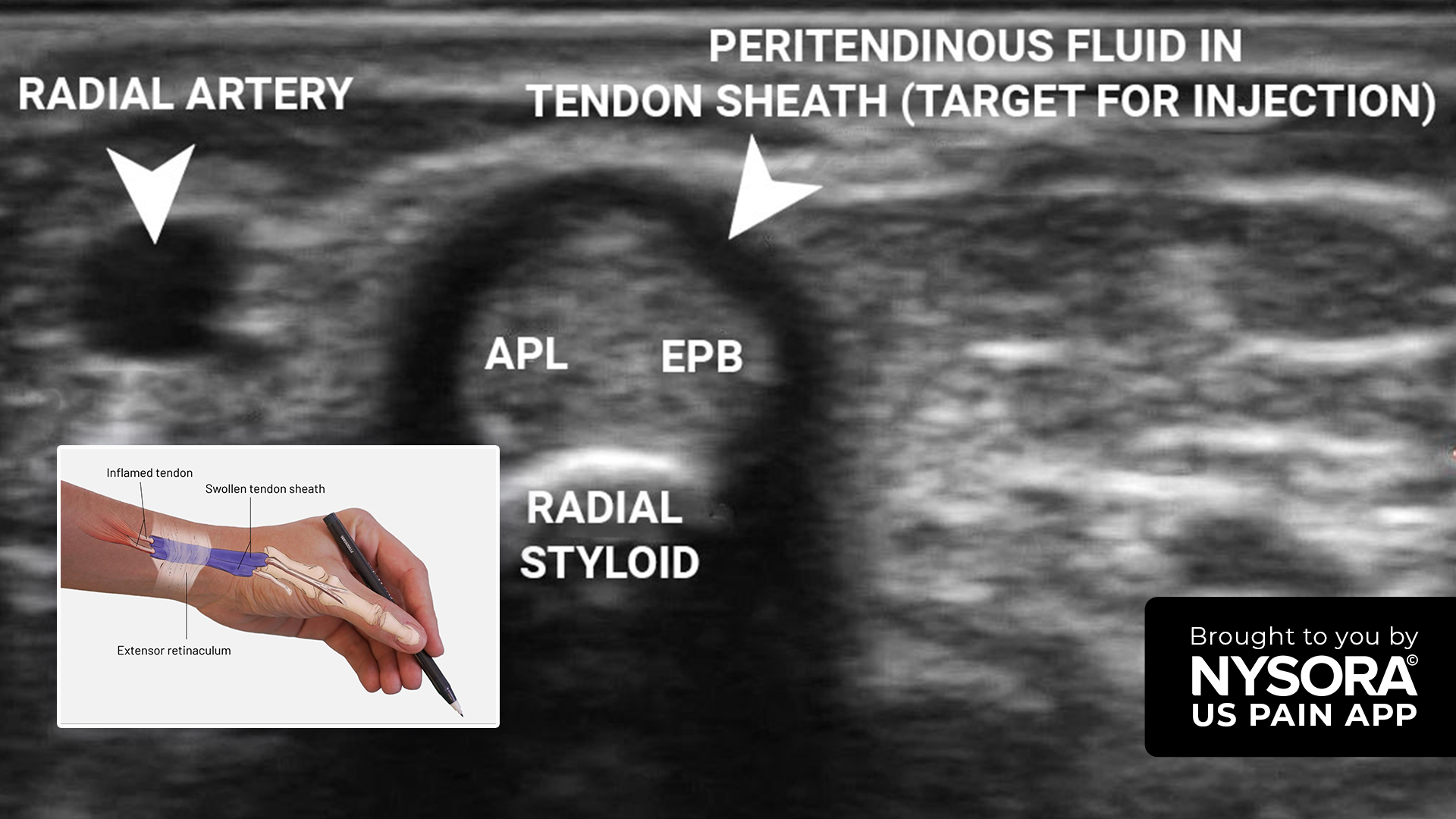





De Quervain’s tenosynovitis is a painful condition affecting the tendons on the thumb side of the wrist. It is particularly prevalent among individuals engaged in repetitive hand movements, such as those working in manual labor or with frequent use of the hands. This article presents a detailed case study of a 56-year-old woman diagnosed with De Quervain’s tenosynovitis.
Case presentation
Patient background:
- Age/gender: 56-year-old woman
- Occupation: Worked in a printing press for 6 years
- Symptoms: Chronic pain in the left hand for six months
- History: No history of hand injury
The patient presented with chronic pain localized to the radial aspect of the wrist, which had progressively worsened over the past six months. Her occupational history involving repetitive hand movements suggested a potential overuse injury.
Diagnosis
Physical examination
- Finkelstein’s test: Positive.
Ultrasound Findings
- Transverse View: Shows a thin rim of inflammatory fluid surrounding the tendons in extensor compartment 1.
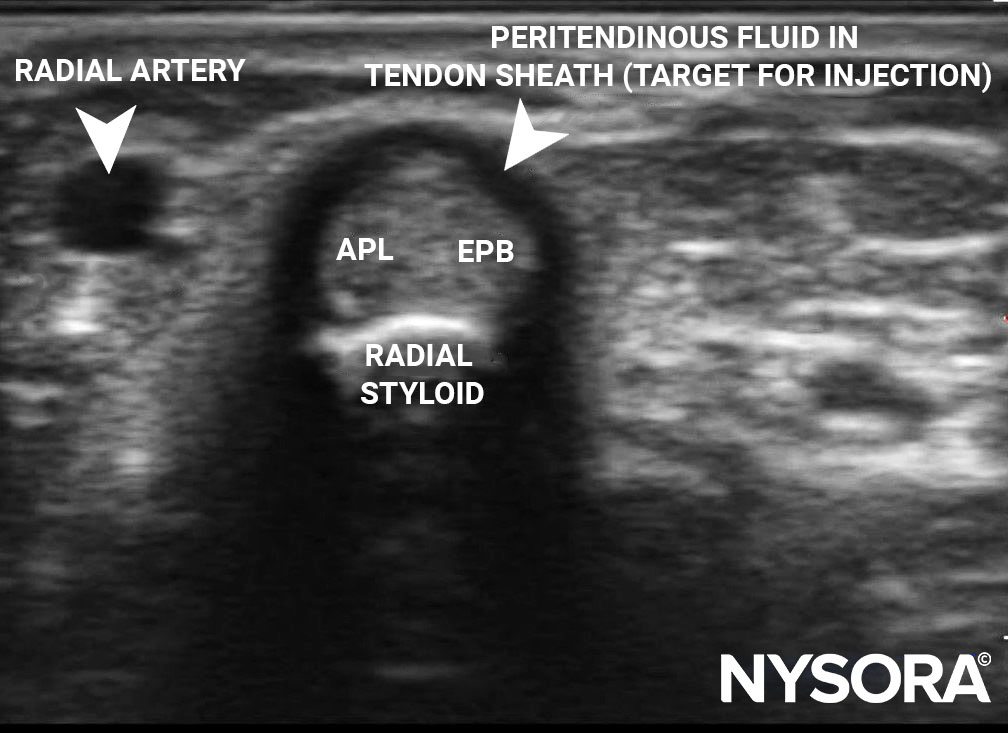
Transverse view of extensor compartment 1 showing a surrounding thin rim of inflammatory fluid. APL, abductor pollicis longus; EPB, extensor pollicis brevis.
- Longitudinal View: Reveals swollen tendons (abductor pollicis longus [APL] and extensor pollicis brevis [EPB]) with surrounding inflammatory fluid.
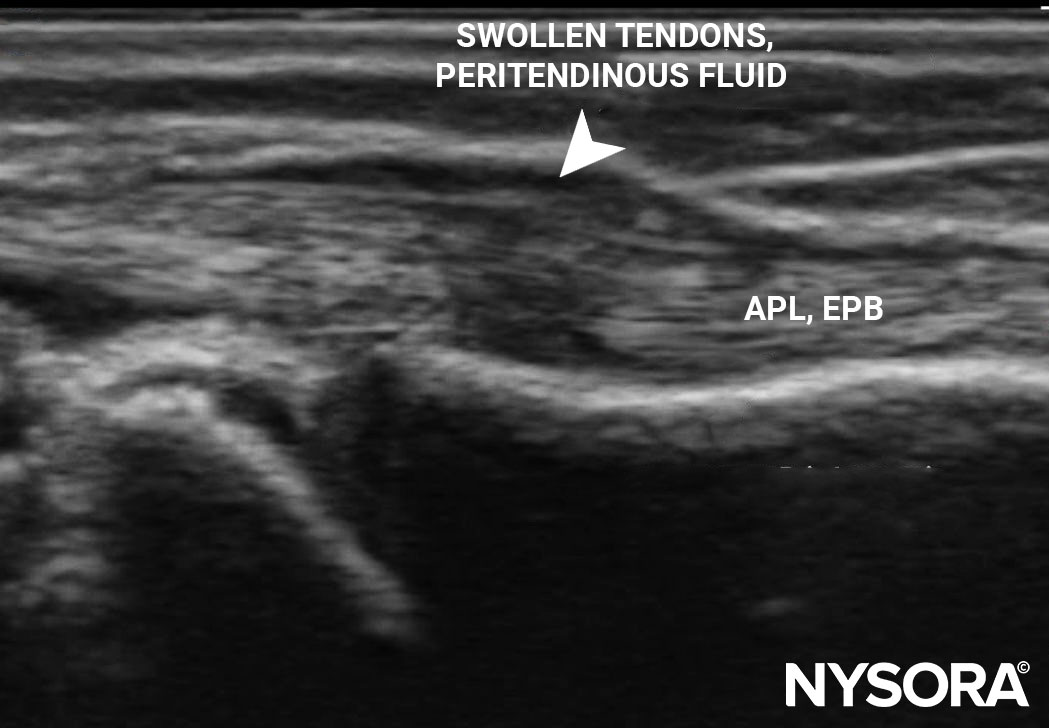
Longitudinal view of extensor compartment 1 showing swollen tendons and a surrounding thin rim of inflammatory fluid. APL, abductor pollicis longus; EPB, extensor pollicis brevis.
Imaging Summary:
- Diagnosis: De Quervain’s tenosynovitis.
- Ultrasound role: Provides detailed imaging of the inflamed tendons and surrounding structures, allowing for precise diagnosis and treatment planning.
Treatment
Corticosteroid injection overview:
- Objective: Pain relief and reduction of inflammation in the affected tendons.
- Target area: Extensor compartment 1 tendon sheath over the wrist.
Ultrasound-guided injection technique:
- Ultrasound setup:
- Transducer: 3-13 MHz linear transducer, preferably a hockey stick probe for better needle visualization.
- Preset: Musculoskeletal.
- Orientation: Axial.
- Depth: 1 cm.
- Patient positioning:
- Position: Patient supine with wrist in a semi-pronated position. A gel tube is placed under the wrist to achieve minimal ulnar deviation for better imaging.
- Landmarks identification:
- Key landmarks: APL, EPB tendons, and surrounding inflammatory fluid.
- Needle insertion:
- Sterile preparation: Sterilize the wrist, hand, and transducer.
- Local anesthetic: Infiltrate with 0.5 mL of 2% lidocaine to avoid distorting the plane of injection.
- Needling technique: A 24-gauge, 1.25-inch needle is inserted laterally to medially, avoiding the radial artery and tendons.
- Injection: 1 mL of 1% lidocaine with 10 mg of triamcinolone is injected into the tendon sheath. Needle fenestration may be performed to release the extensor retinaculum over the APL and EPB tendons.
Important considerations:
- Avoid injecting into tendon: Care should be taken to inject within the sheath rather than into the tendon itself to prevent tendon damage.
Interested in more detailed information and the outcome for this patient? Download NYSORA’s US Pain App!