Learning objectives
- Assessment of the injury severity score of trauma
- Immediate treatment of trauma
- Anesthetic management of trauma
Definition and mechanisms
- Defined as a body wound resulting from a sudden physical injury from impact, violence, or accident
- Minor, serious, life-threatening, or potentially life-threatening injuries
- Blunt or penetrating wound
- The severity of trauma is classified according to the injury type, the physical location of the injury, and how many injuries there are
- Immediately life-threatening injuries:
- Airway obstruction
- Tension pneumothorax
- Open pneumothorax
- Cardiac tamponade
- Massive hemothorax
- Flail chest
- Delayed/hidden injuries:
- Thoracic aortic disruption
- Tracheobronchial disruption
- Myocardial contusion
- Traumatic diaphragmatic tear
- Esophageal disruption
- Pulmonary contusion
Complications
- Hemorrhage
- Infection
- Sepsis
- Multi-organ failure
Injury severity score
- Individual body regions are assigned an abbreviated injury scale (AIS) score
- The three most severely injured body regions then have their score squared and added together to produce the AIS score
| Abbreviated injury scale | Injury |
|---|---|
| 1 | Minor |
| 2 | Moderate |
| 3 | Serious |
| 4 | Severe |
| 5 | Critical |
| 6 | Unsurvivable |
Immediate treatment
- Cardiovascular reuscitation
- Cervical collars:
- May increase secondary neurological injury, intracranial pressure
- May worsen intubation conditions
- Secure the airway
- Proactive early treatment to counter the ‘lethal triad’ of acidosis, hypothermia, and coagulopathy
- Warm the OR
- Warmed IV line
- Rapid infuser with warming capability
- Permissive hypotension and establishment of a massive transfusion protocol
- Early treatment of anticipated coagulopathy with blood products
- Other injuries, considerable pain, or distal ischemia may complicate the management
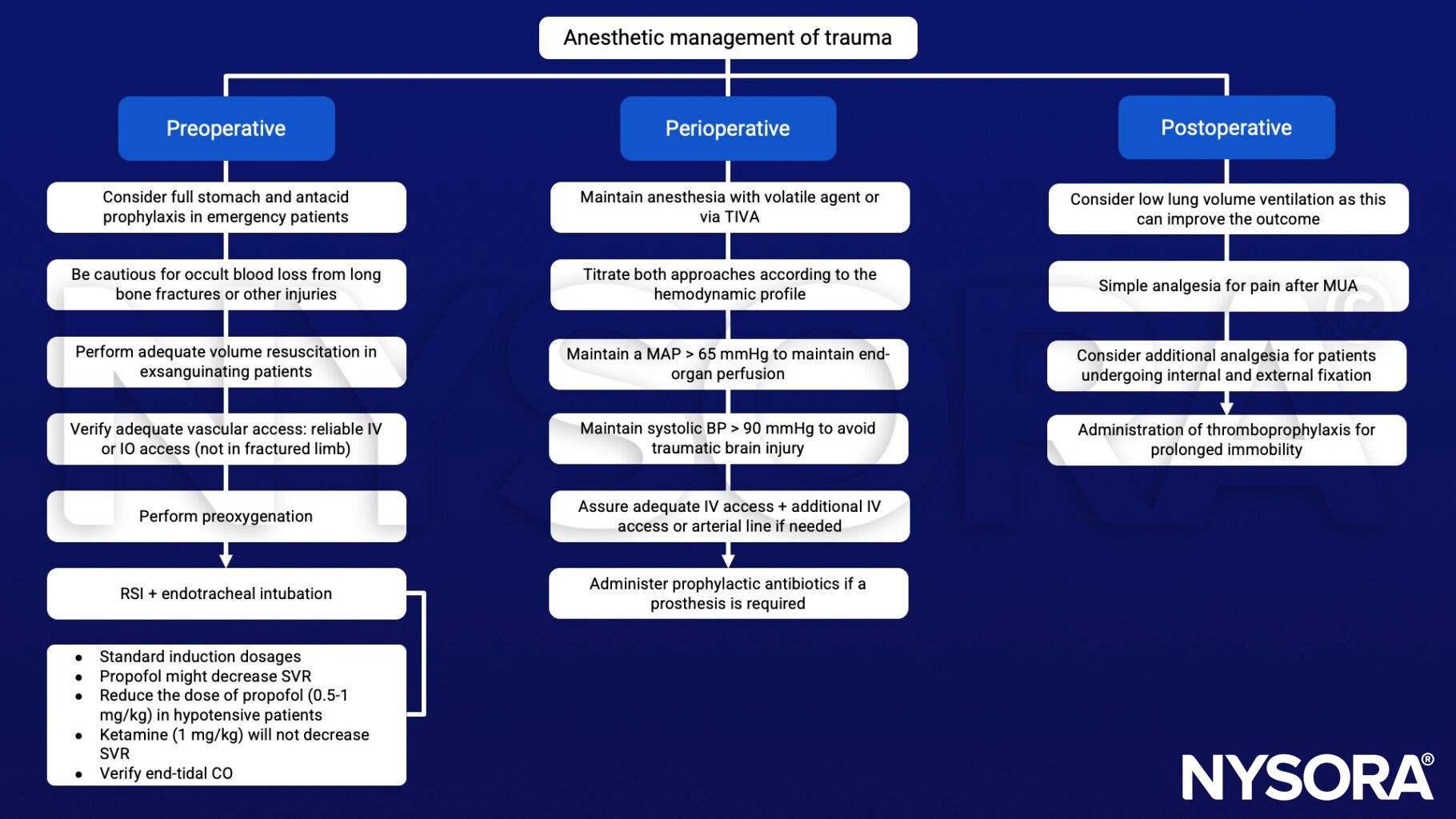
Anesthetic management
- Fracture reduction requires general or regional anesthesia
- Proximal fracture reduction or joint relocation performed under GA may require a small dose of a neuromuscular blocker to facilitate manipulation
- Manipulation under anesthesia (MUA)
- Relocation of dislocated joints
- Correct fracture deformity
- Improve mobility of fixed joints
- Improve mobility after arthroplasty:
- Internal fixation
- Distal long bone fracture plating
- Intramedullary nailing procedures
- External fixation
Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Tobin JM, Barras WP, Bree S, et al. Anesthesia for Trauma Patients. Mil Med. 2018;183(suppl_2):32-35.
- Uday Jain, Maureen McCunn, Charles E. Smith, Jean-Francois Pittet; Management of the Traumatized Airway. Anesthesiology 2016; 124:199–206.
Clinical updates
Voelckel (Current Opinion in Anaesthesiology, 2025) reviews the role of arginine vasopressin (AVP) in traumatic hemorrhagic shock and reports that while 23 animal studies consistently show improved arterial pressure, reduced fluid requirements, and enhanced survival, human data remain inconclusive. Two randomized controlled trials in trauma patients demonstrated reduced fluid needs, but no clear survival benefit, and observational studies failed to confirm improved outcomes. Current trauma guidelines therefore, continue to recommend norepinephrine as first-line vasopressor therapy, reserving vasopressin as a potential rescue agent in catecholamine-refractory shock pending further high-quality trials to define optimal timing, dosing, and safety.
- Read more about this study HERE.