Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the risk factors and pathophysiology of TRALI
- Diagnose and manage TRALI
- Prevent TRALI
Background
- Transfusion-related acute lung injury (TRALI) is a transfusion reaction characterized by an acute, noncardiogenic pulmonary edema associated with hypoxia
- The leading cause of death from transfusion
- Caused by damage to pulmonary vasculature due to the immune response to antibodies or proinflammatory factors from the transfusion product that bind to antigens of the recipient
- Symptoms include acute dyspnea, fever, hypotension, and tachycardia
Risk factors
- Mechanical ventilation
- Sepsis
- Massive transfusion
- Coronary artery bypass graft
- End-stage liver disease
- Positive fluid balance
- Critically ill patient
- Blood products with high plasma contents
Pathophysiology
- Two-hit hypothesis:
- Threshold hypothesis
- No first hit, a threshold must be overcome to induce TRALI
- Threshold depends on the susceptibility of the patient and the quantity of antibodies/proinflammatory factors in the transfusion product
Diagnosis
- Diagnostic criteria:
- Symptoms develop during or within 6 hours of transfusion without any risk factors for developing acute lung injuries (sepsis from pneumonia, aspiration, shock)
- Clinical findings:
- Exudative bilateral infiltrates on chest radiograph
- No evidence of pulmonary vascular overload
- Hypoxemia: SpO2 <90% on room air, ratio of partial oxygen pressure to fractional inspired oxygen concentration <300 mmHg
- Possible TRALI: Other risk factors for acute lung injury
- Delayed TRALI: 6 – 72 hours after transfusion
Differential diagnosis
- Septic transfusion reaction: Signs of sepsis
- Anaphylactic transfusion reaction: Laryngeal and bronchial edema
- Transfusion-related circulatory overload: Increased pulmonary artery occlusion pressure (>18 mmHg)
Treatment
- There is no treatment, management is supportive
- Stop transfusion
- Additional oxygen
- Restrictive tidal volume ventilation
- Diuretics may be considered
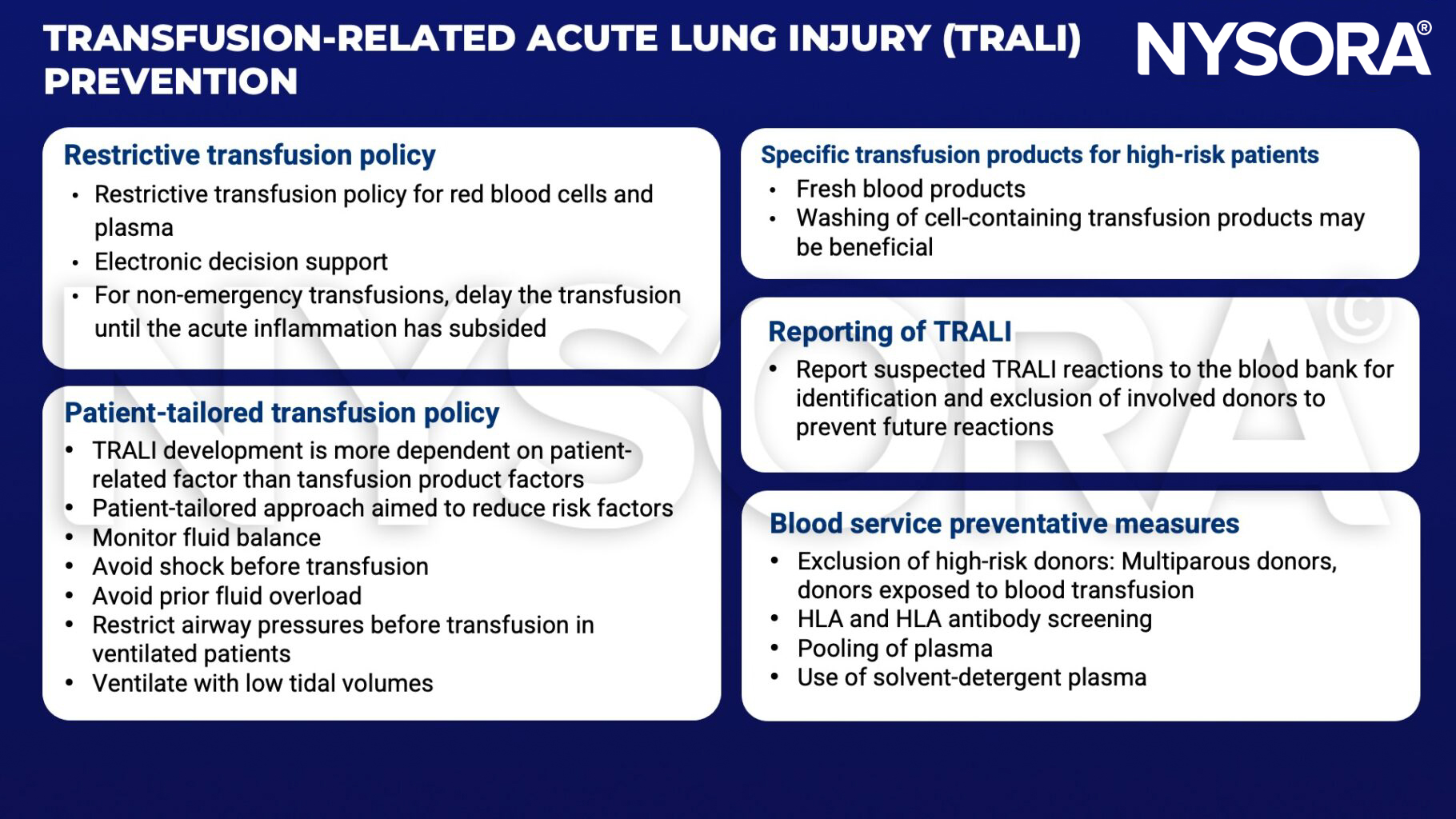
Prevention
Suggested reading
- Cho MS, Modi P, Sharma S. Transfusion-related Acute Lung Injury. [Updated 2022 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507846/
- Vlaar AP, Juffermans NP. Transfusion-related acute lung injury: a clinical review. Lancet. 2013;382(9896):984-994.
Clinical updates
Kor et al. (Anesthesiology, 2025) investigate whether point-of-care washing of allogeneic red blood cells reduces biological markers associated with transfusion-related respiratory complications, including pathways implicated in TRALI. The study shows that RBC washing significantly reduces proinflammatory mediators, cell-free hemoglobin, and microparticles that are thought to contribute to neutrophil activation and endothelial injury in TRALI.