Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe and classify mitral regurgitation
- Describe the causes and mechanisms of mitral regurgitation
- Manage patients with mitral regurgitation
Definition & mechanisms
- Mitral regurgitation (MR) can be acute or chronic in onset, and primary or secondary in nature
- Primary MR is due to pathology of the valve preventing normal closure
- Secondary MR is caused by left ventricle dysfunction that affects the closing of the mitral valve
- The left atrium dilates as blood is ejected back into it
- Atrial fibrillation is common
- Overload of the pulmonary circulation causes dyspnea
- The LV is volume overloaded in, with dilation of the ventricle further worsening MR
- Acute MR:
- Can be caused by any disruption to the normal mechanism of the valve (growth of vegetations on the leaflets in infective endocarditis, chordae rupture in patients with pre-existing degenerative disease, or papillary muscle rupture due to an ST-elevation)
- The left atrium is unable to compensate acutely for the increased pressure caused by blood refluxing back into it
- Patients can present with sudden-onset dyspnea and require rapid stabilization and treatment
- Chronic MR:
- Primary: Abnormality of the leaflets that prevents them from closing normally
- Secondary: Anatomy of the valve is normal, but its function is impaired due to left ventricle pathology
Classification
Transoesophageal echocardiography remains the gold standard for defining the severity of the MR:
| Mild | Moderate | Severe | |
|---|---|---|---|
| Regurgitant fraction | <30% | 30–49 | ≥50% |
| Regurgitant orifice area | <0.20 cm2 | 0.2–0.39 cm2 | ≥0.40 cm2 |
| Regurgitant volume | <30 mL/beat | 30–59 mL/beat | ≥60 mL/beat |
Treatment
- Medical
- Acute MR: Filling pressure reduction with nitrates or diuretics and afterload reduction with vasodilators or an intra-aortic balloon pump as bridging to definitive treatment
- Chronic MR: Treatment is in line with standard heart failure management including β-blockers, angiotensin-converting enzyme inhibitors, and aldosterone antagonists, with diuretics where heart failure is present
- Surgical
- Primary MR:
- Surgery is indicated if the MR is severe and acute in nature and if the MR is chronic and causing symptoms, with no contraindications to surgery
- Valve repair, rather than replacement, is preferred
- Secondary MR:
- In symptomatic patients with severe left ventricle failure, the benefits of surgery are controversial unless the underlying condition can be reversed
- Primary MR:
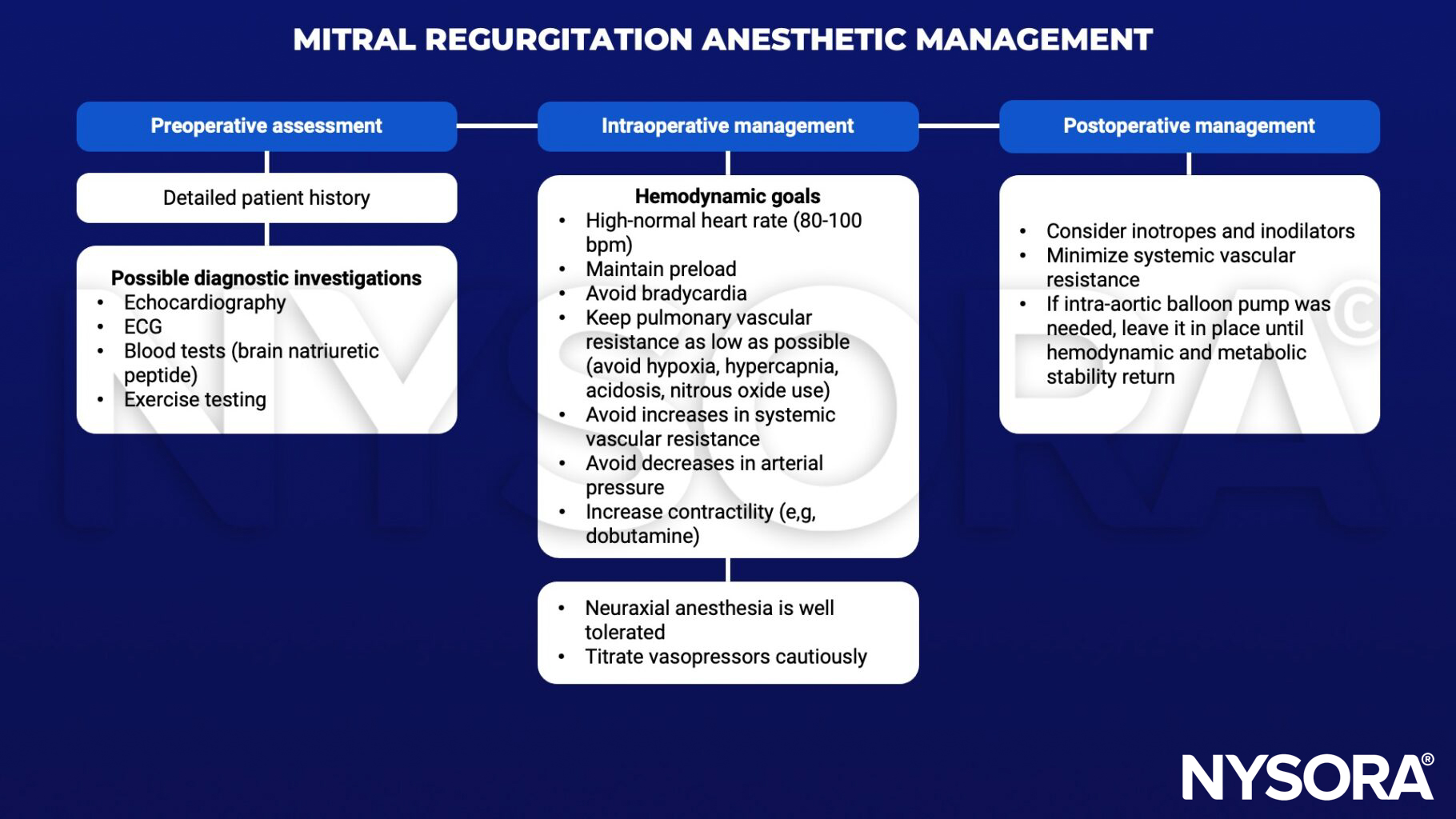
Anesthetic management
Suggested reading
- Holmes K, Gibbison B, Vohra HA. Mitral valve and mitral valve disease. BJA Education. 2017;17(1):1-9.