Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Outline the risks of having a full stomach in combination with anesthesia
- Describe the factors that delay gastric emptying
- Anesthetic management of a patient with a full stomach
Definition and mechanisms
- In anesthesia, the term “full stomach” applies to patients that have recently ingested foods and/or have pharmacologic, metabolic, anatomic, or hormonal conditions, which impair gastric emptying
- A full stomach and any reduction in the functional integrity of the lower esophageal sphincter (LES) predispose a patient to regurgitation
- The active process of vomiting and the passive process of regurgitation of gastric contents are more hazardous in a patient with a full stomach
- No patient can ever be assumed to have a completely empty stomach
General anesthesia suppresses the upper airway reflexes that prevent pulmonary aspiration of active or passively regurgitated gastric contents
- Aspiration of solid material can cause a mechanical obstruction with subsequent lung collapse, pneumonia, or abscess formation
- Aspiration of liquid (>25 mL, pH <2.5) can cause bronchospasm, pneumonitis, bronchopneumonia, and acute respiratory distress syndrome
Strategies to reduce the risk of pulmonary aspiration
- Minimize residual gastric volumes → fasting (stomach is considered “empty” within 6 hours after food and milky drinks, 4 hours after breast milk, and 2 hours after water)
- Rapidly secure the anesthetized airway
Emergency patients are more likely to have a full stomach as
- Presenting pathology causes a mechanical obstruction (e.g., laparotomy for small bowel obstruction)
- Surgery is urgent and cannot wait for the full fasting time
- The surgical pathology results in pain and anxiety
Risk factors
Factors delaying gastric emptying
- Mechanical obstruction of the gastrointestinal tract
- Ileus
- Following surgical manipulation of the bowel (postoperative)
- Recent trauma
- Electrolyte imbalance
- Peritonitis
- Pain
- Fear and anxiety
- Third trimester of pregnancy
- Drugs
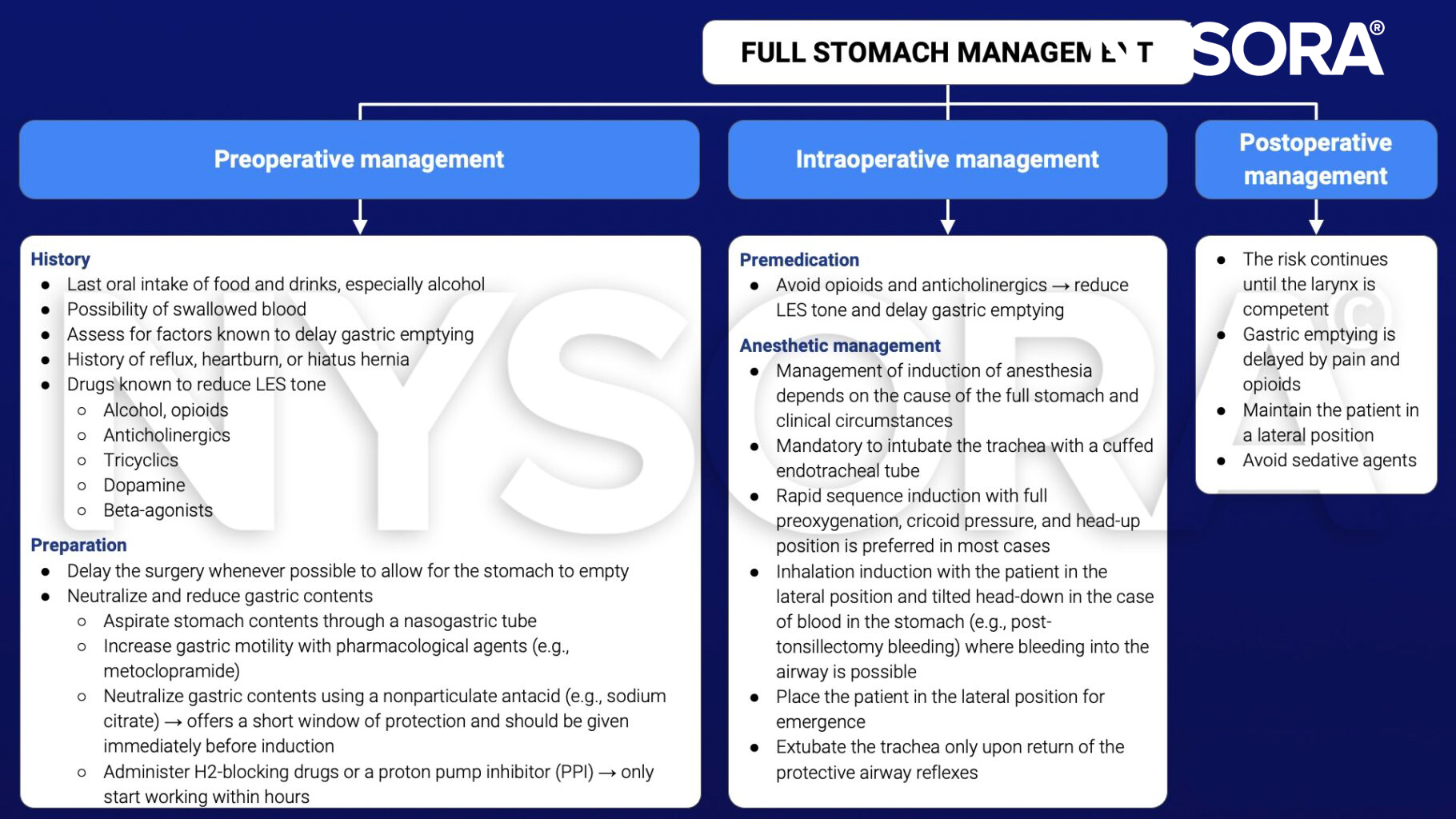
Management
Suggested reading
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 4 Gastrointestinal tract, Jackson MJ.
Clinical updates
Sastre et al. (A&A, 2024) report that diabetic patients with dysautonomia have a significantly higher prevalence of a full stomach on preoperative gastric ultrasound (22.9%) compared with diabetics without dysautonomia and healthy controls, despite standard fasting. Solid gastric contents were also more frequent in this group, while gastroparesis symptoms alone were poor predictors of aspiration risk.
- Read more about this study HERE.