Learning objectives
- Recognize fat embolism syndrome (FES)
- Describe the presenting clinical features in patients with suspected FES
- Explain the management of FES, including the limited drug treatments
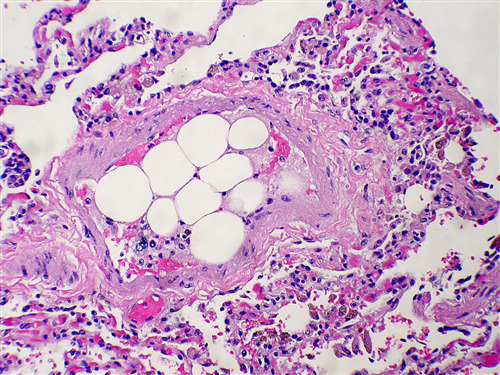
Definition and mechanism
- The presence of fat globules within the lung parenchyma or peripheral microcirculation
- Causes direct tissue damage as well as the induction of a systemic inflammatory response
- Result in pulmonary, cutaneous, neurological, and retinal symptoms
- Estimated to occur in 1-10% of patients
- Mortality is 10-20%
Signs and symptoms
| Respiratory | Tachypnea Hypoxemia Acute Respiratory Distress Syndrome |
| Neurological | Confusion Seizures Altered level of consciousness Focal neurological deficits |
| Dermatological | Petechial rash |
| Systemic | Fever |
| Cardiovascular | Tachycardia Hypotension Intraoperative arrhythmias Myocardial ischemia Pulmonary hypertension (PH) Right-sided heart failure |
| Ophthalmic | Purtscher’s retinopathy (cotton wool exudates, macular edema and hemorrhage) |
| Renal | Oliguria Proteinuria Lipiduria Hematuria |
| Hepatic | Jaundice |
| Haematological | Perioperative anemia Thrombocytopenia Coagulopathy Fat macroglobulinemia |
Causes
- Trauma to long bone/pelvis
- Prosthetic joint replacement
- Liposuction
- Bone marrow harvest or transplant
- Bone tumor lysis
- Acute pancreatitis
- Hepatic necrosis and fatty lever
- Acute sickle cell crisis
- Major soft tissue injury
- Recent orthopedic procedure
- Recent lipid infusion
- Severe burns
Diagnosis
One major and 4 minor of Gurd’s Diagnostic Criteria are proposed, together with fat macroglobulinemia, as sufficient to diagnose fat embolism syndrome
Gurd’s diagnostic criteria
| Diagnosis | Criteria |
|---|---|
| Major criteria | Respiratory insufficiency Cerebral involvement Petechial rash |
| Minor criteria | Tachycardia Fever Jaundice Retinal changes Renal changes ↓ Hemoglobin Thrombocytopenia ↑ Erythrocyte sedimentation rate Fat globulus in sputum |
| Laboratory findings | ↓ in hematocrit at 24 to 48 hours Thrombocytopenia Fat globulus in blood and urine Fat macroglobulinemia raised free fatty acids and triglyceride in serum |
Management
- Respiratory support: intubation/ventilation, indications for respiratory support:
- Sustained SaO2 <90% and PaO2 <8 kPa on oxygen
- Respiratory rate of >35 breaths/min
- Hemodynamic support:
- Maintain a systolic blood pressure > 90 mmHg
- Avoid hypovolemia with fluid resuscitation and vasopressors
- Apply invasive monitoring
- TEE
- Early surgical stabilization of fractures
- Perform operative correction rather than traction alone
- Limit the intraosseous pressure during an orthopedic procedure
Pharmacological treatment
- Corticosteroids may reduce the risk of a fat embolism in patients with long bone fractures of the lower limbs
- Heparin clears lipemic serum by stimulating lipase activity, thereby reducing pulmonary complications
- Albumin use is considered potentially therapeutic in its ability to bind free fatty acids
Suggested reading
- Luff D, Hewson DW. Fat embolism syndrome. BJA Educ. 2021;21(9):322-328.
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
Clinical updates
Kiaei et al. (Archives of Anesthesiology and Critical Care, 2026) report a fatal perioperative case in a 48-year-old man with a femoral fracture who developed acute hypoxemia, generalized seizure, petechiae, right ventricular dilation on echocardiography, and cardiovascular collapse shortly after spinal anesthesia, raising a strong suspicion for fat embolism syndrome (FES). The authors emphasize the diagnostic overlap with local anesthetic systemic toxicity (LAST) and possible inadvertent intrathecal drug error, noting lipid emulsion was administered despite uncertain benefit in FES, and conclude that early echocardiography, consideration of ECMO in refractory cases, and meticulous medication verification are critical in high-risk perioperative trauma patients.
Baba et al. (Internal Medicine, 2025) describe a 74-year-old woman who developed acute shock and right ventricular dilatation 22 h after total hip arthroplasty; despite high-dose norepinephrine and dobutamine, she remained unstable until receiving 250 mg intravenous methylprednisolone, after which blood pressure normalized within ~15 minutes. Diagnosis of fat embolism syndrome (FES) was supported by urinary fat globules, pulmonary perfusion defects, and brain MRI showing cerebral fat emboli, and a second 250 mg dose was given on POD 2 with sustained recovery, suggesting high-dose short-course methylprednisolone may provide rapid hemodynamic benefit in severe FES, although evidence remains limited to case-based data.
Al Bshabshe et al. (Journal of Clinical Medicine, 2025) conducted a 20-year mini-review of published cases describing ECMO use in severe fat embolism syndrome (FES), finding that most patients with refractory hypoxemia or cardiogenic compromise experienced substantial improvement in oxygenation and survived to hospital discharge. Although complications such as acute kidney injury, infection, hemolysis, and circuit-related issues were common, they were generally manageable, supporting early ECMO as a bridge-to-recovery strategy in carefully selected patients with life-threatening FES unresponsive to conventional therapy.
Luff and Hewson (BJA Education, 2021) review fat embolism syndrome (FES) as a rare but potentially fatal complication of long bone trauma, typically presenting 24–72 h after injury with hypoxia (≈96%), neurological disturbance (≈59%), and petechial rash (≈33%), and mortality reported between 7–36%. They outline three complementary pathogenetic mechanisms—mechanical embolisation, free fatty acid–mediated endothelial injury, and inflammation-driven coagulation activation—and emphasise supportive critical care management (lung-protective ventilation, early fracture fixation), noting that although meta-analysis suggests prophylactic corticosteroids may reduce FES risk (RRR 78%; NNT≈8), routine use remains controversial given potential adverse effects and limited high-quality data.