Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Pain after median sternotomy remains one of the most challenging aspects of cardiac anesthesia and recovery. Despite advances in surgical technique and multimodal analgesia, many patients experience moderate to severe discomfort in the early postoperative period. This pain is not merely distressing—it directly interferes with deep breathing, coughing, and mobilization, all essential components of enhanced recovery pathways. When pain limits these functions, pulmonary complications such as atelectasis and pneumonia become more likely, leading to longer mechanical ventilation and ICU stays.
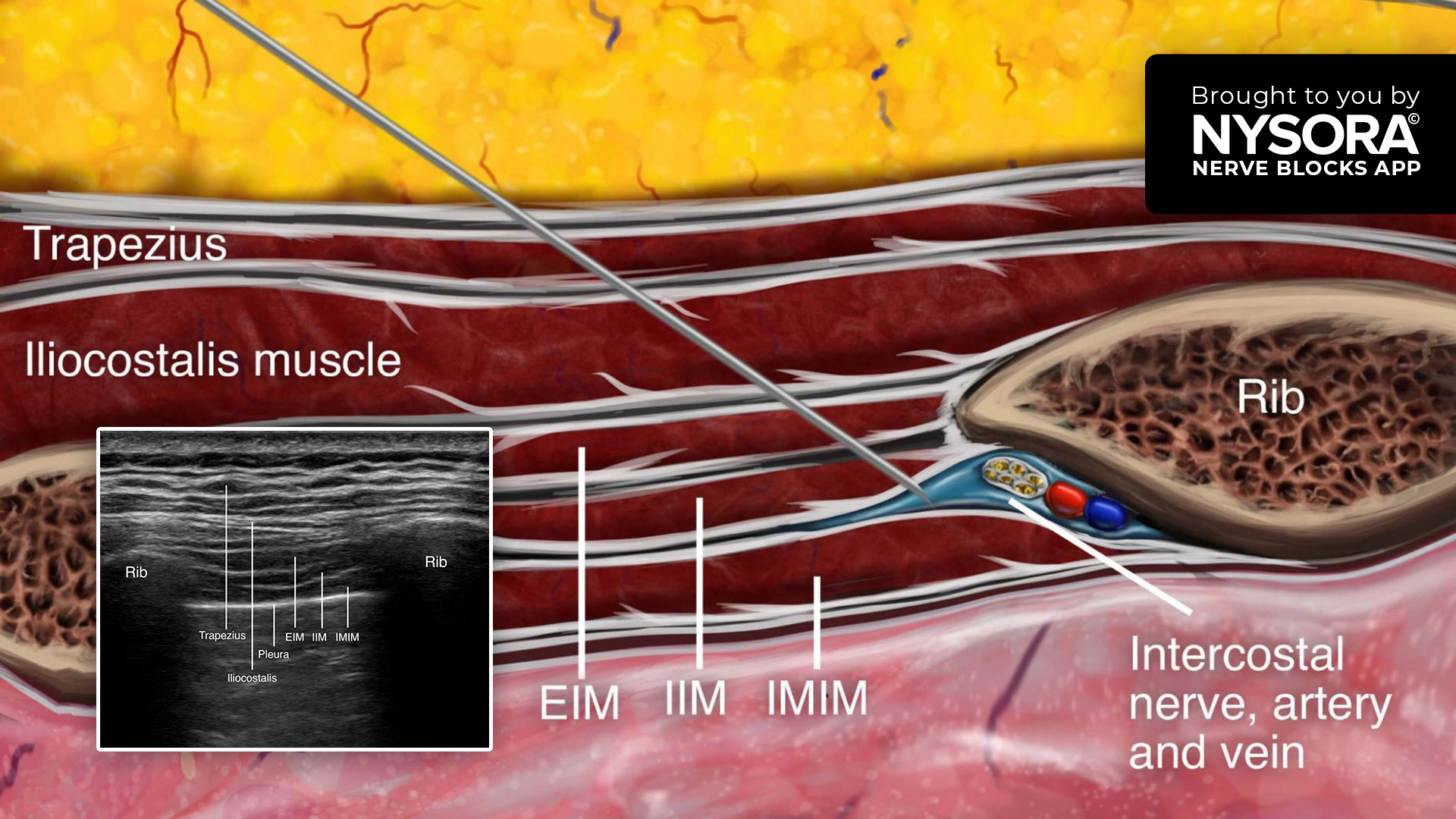
Regional anesthesia has become an increasingly important tool in addressing this issue, providing effective, targeted analgesia without the hemodynamic risks associated with neuraxial techniques. The ultrasound-guided parasternal (pecto-intercostal plane) block is one of the most widely adopted options for median sternotomy. By anesthetizing the anterior cutaneous branches of the intercostal nerves (T2–T6), it provides substantial relief from sternal pain and reduces opioid consumption.
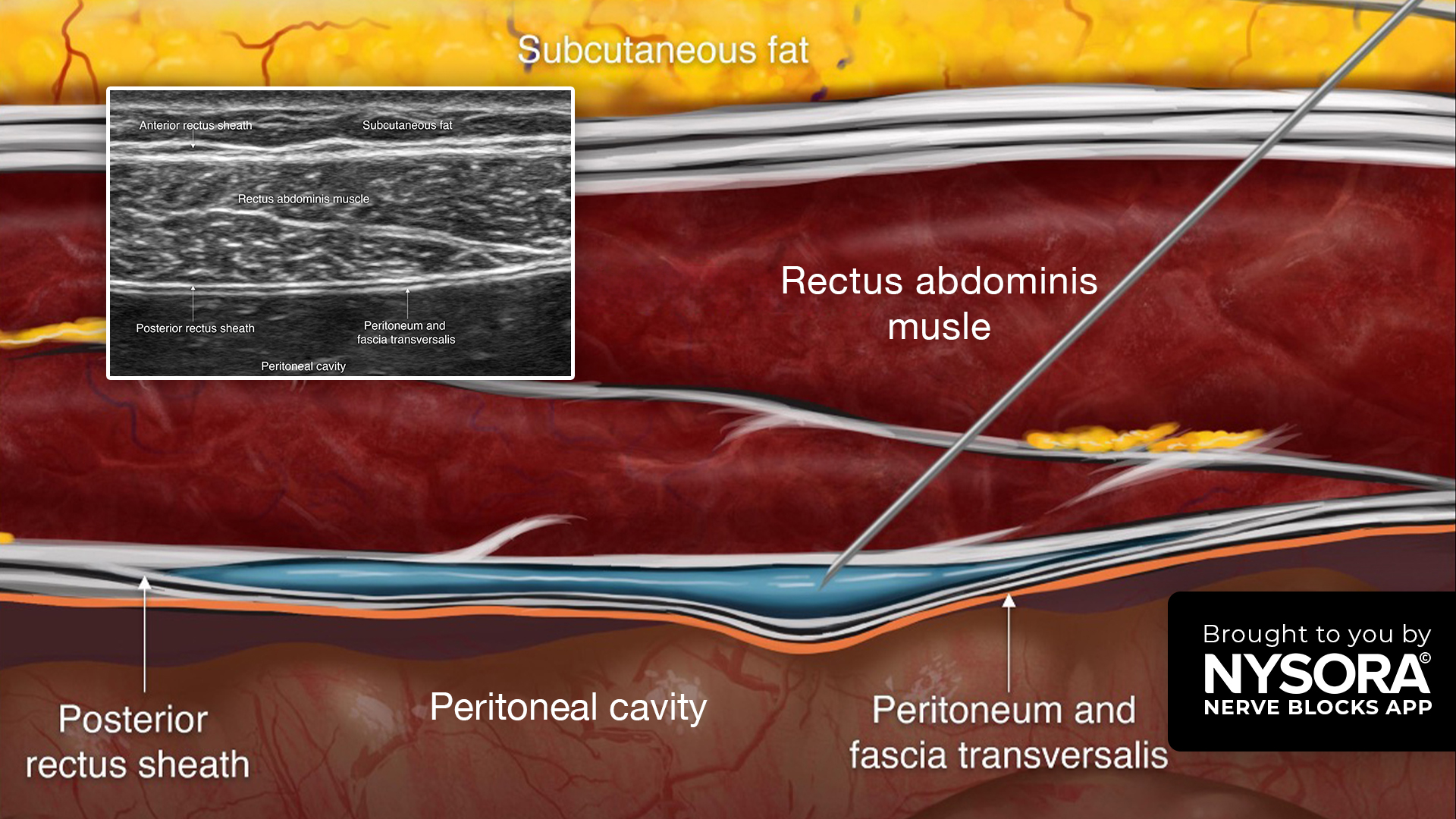
However, the parasternal block does not consistently cover the lower sternum and epigastric region—precisely where mediastinal and pleural drains emerge. Pain at these drain exit sites can persist even when the sternum itself is well controlled, compromising respiratory exercises and delaying extubation. The rectus sheath block (RSB), traditionally used for midline abdominal incisions, targets the anterior cutaneous branches of T6–T9 and may therefore complement the parasternal block by extending coverage to this critical epigastric zone.
This study set out to determine whether combining the rectus sheath block with the parasternal block could improve pain control and respiratory recovery after cardiac surgery via median sternotomy.
Study objective and methods
The primary objective of the study was to determine whether parasternal and rectus sheath blocks improve pain at rest at extubation compared to parasternal and epigastric infiltration.
- Design: Single-centre, single-blinded, randomized controlled superiority trial.
- Setting: University Hospital, Italy.
- Population: 58 adult patients (ASA I–IV) undergoing elective cardiac surgery via median sternotomy.
- Parasternal + rectus sheath block group (n = 29): Bilateral parasternal block plus bilateral rectus sheath block.
- Parasternal + infiltration group (n = 29): Bilateral parasternal block plus surgical infiltration of local anesthetic at epigastric drain exit sites.
Interventions
- Parasternal block: Performed under ultrasound guidance after induction. 20 mL of 0.5% ropivacaine with 1 mg dexamethasone per side, divided between the 2nd and 4th ribs (targeting T2–T6).
- Rectus sheath block: Ultrasound-guided, 10 mL of 0.25% ropivacaine per side injected between the rectus muscle and posterior sheath (targets T6–T9).
- Control group: 20 mL of 0.25% ropivacaine infiltrated by the surgeon at the epigastric drain exit sites.
Outcomes
- Primary: Pain at rest (NRS 0–10) at extubation.
- Secondary: Pain at rest and during respiratory effort at 0–6, 6–12, and 12–24 h; opioid consumption during the first 24 h; respiratory performance using TriFlow incentive spirometry (number of spheres lifted); postoperative nausea and vomiting (PONV); extubation time; ICU and hospital length of stay.
Key findings
-
Improved pain control at rest and during breathing
Adding an RSB to the parasternal block produced small but consistent improvements in postoperative pain control. At extubation, median NRS pain at rest was 4 (IQR 4–4) versus 5 (4–5) with infiltration (p = 0.03), and this ~ 1-point advantage persisted at 6, 12, and 24 hours.
Pain during respiratory effort (TriFlow testing) was also lower across all time intervals (all p < 0.01, except at extubation, p = 0.04), confirming better comfort during deep breathing and coughing—key to early pulmonary recovery.
-
Reduced opioid requirement and fewer side effects
Although total morphine use was low overall, patients in the RSB group required significantly less: 0 mg [0–2] vs 2 mg [0–4] in 24 hours (p < 0.01). Fewer RSB patients needed opioids at all (34.5% vs 55%), and the incidence of PONV was markedly lower (7% vs 34.5%; p < 0.01), likely due to reduced opioid exposure.
-
Faster respiratory recovery
Inspiratory performance, measured with the TriFlow incentive spirometer, improved earlier in the RSB group. At 6 and 12 hours post-extubation, patients lifted more spheres (median 2 vs 1; p < 0.01 and p < 0.001, respectively), reflecting higher inspiratory flow rates and better participation in respiratory exercises. By 24 hours, values aligned, but IQR separation remained statistically significant, indicating smoother early recovery.
-
Safety and resource outcomes
No differences were observed in extubation time, ICU stay, or hospital stay between groups, and pneumonia was rare in both. No block-related complications were reported, underscoring the safety of the combined approach when performed under ultrasound guidance by experienced operators.
-
Anatomical rationale confirmed
The parasternal block anesthetizes anterior cutaneous branches from T2–T6, while the RSB covers T6–T9, extending coverage to the lower sternum and epigastric drain sites. This complementary pattern likely explains the consistent improvements in drain-site pain and effort-related discomfort.
Conclusion
In patients undergoing cardiac surgery via median sternotomy, combining a rectus sheath block with a parasternal block improved early pain control, reduced opioid consumption, decreased PONV, and enhanced inspiratory performance during the first 12 hours after extubation. Although the effect sizes were small, the findings were consistent and clinically relevant for epigastric and drain-site pain—areas often inadequately covered by a parasternal block alone.
Future research
- Larger, multicentre, double-blind trials powered for patient-centred outcomes (e.g., time to effective cough, extubation, ICU stay).
- Studies comparing single-shot vs continuous techniques for sustained benefit.
- Dose and volume optimization, especially for different body weights.
- Objective respiratory measures such as cough peak flow or pulmonary complication scores.
- Identification of patient groups most likely to benefit (e.g., high drain burden, bilateral internal mammary harvest).
Clinical implications
For centres already using parasternal blocks, adding RSB is a practical way to address residual pain from lower sternotomy and epigastric drain sites. Expect roughly a one-point reduction in NRS pain, less effort-related discomfort, reduced morphine use by about 2 mg, and less PONV. These differences may not alter length of stay but can make early recovery smoother—especially in older or pulmonary-compromised patients. Both blocks require ultrasound expertise and clear anatomical confirmation to ensure safety and efficacy. If time or skill set is limited, RSB can be reserved for patients with significant drain-related discomfort.
Clinical pearls
- Adding RSB to parasternal reduced pain scores by ~ 1 point at rest and during breathing.
- Early respiratory recovery: Higher TriFlow performance at 6–12 h post-extubation.
- Lower 24-h morphine use (~ 2 mg less) and markedly reduced PONV (7% vs 34.5%).
- Parasternal covers T2–T6; RSB extends to T6–T9, targeting the drain-site and lower sternal pain.
Practical tip: When drains exit epigastrically, add bilateral RSB to parasternal block to reduce drain-site pain and support early breathing exercises.
For more detailed information, refer to the full article in RAPM.
Strumia A. et al. Rectus sheath block added to parasternal block may improve postoperative pain control and respiratory performance after cardiac surgery: a superiority single-blinded randomized controlled clinical trial. Reg Anesth Pain Med. 2025;50:712-718.
Download the Nerve Blocks App HERE for in-depth insights on the parasternal and rectus sheath techniques. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!