Risk factors & signs
Risk factors
- Male gender
- Family history of AAA
- Age (above 65)
- Diabetes mellitus
- Smoking
- Arterial hypertension
- Coronary artery and/or peripheral vascular disease
- Obesity
Common signs
- Hypotension
- Abdominal pain (flank or back)
- Pulsatile abdominal mass
- Syncope
- Shock
- Cardiac arrest
- Thromboembolic events in the lower extremities
- Neurologic deficit of the lower extremities
Notes
- AAA is an uncommon, life-threatening vascular emergency
- Ruptured AAA = 90% mortality.
- Ultrasound scanning should never delay surgical intervention.
- Perform an aortic ultrasound on patients suspected of asymptomatic AAA.
Essential info
- There are two distinct morphological forms of AAA: Fusiform (symmetrical, circumferential) and saccular (asymmetrical outpocketings).
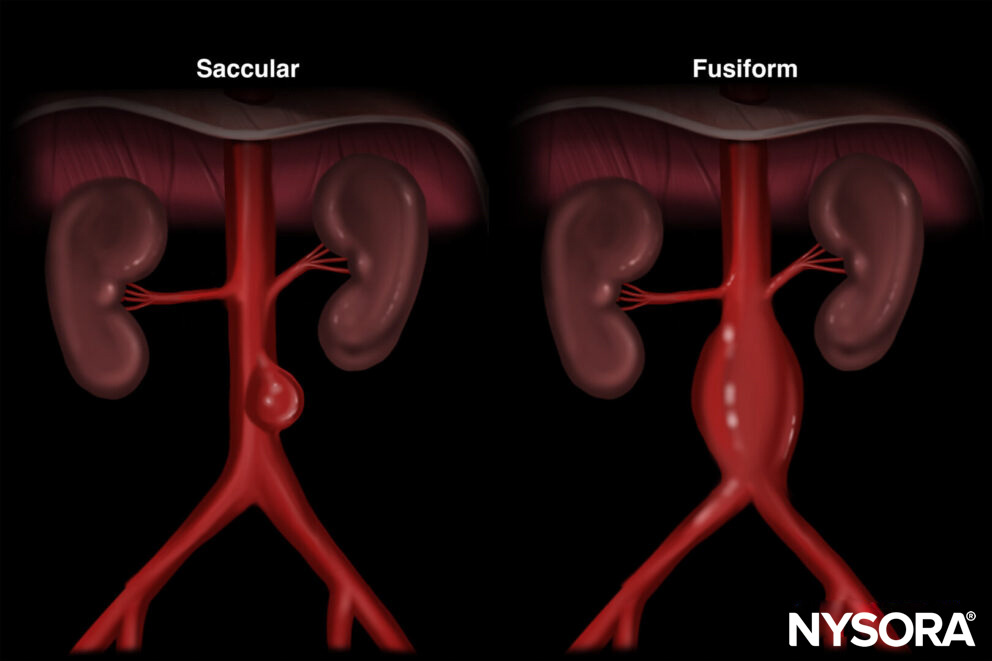
Morphological forms of AAA: Fusiform and saccular.
- Fusiform AAA is the most common and is less likely to cause symptoms compared to saccular AAA.
- US screening for AAA has a high sensitivity (94%) and a specificity (98%).
- Symptoms are often absent, nonspecific, or misleading. The classic triad of hypotension, abdominal pain, and a pulsatile abdominal mass is observed in 25% of patients with an AAA.
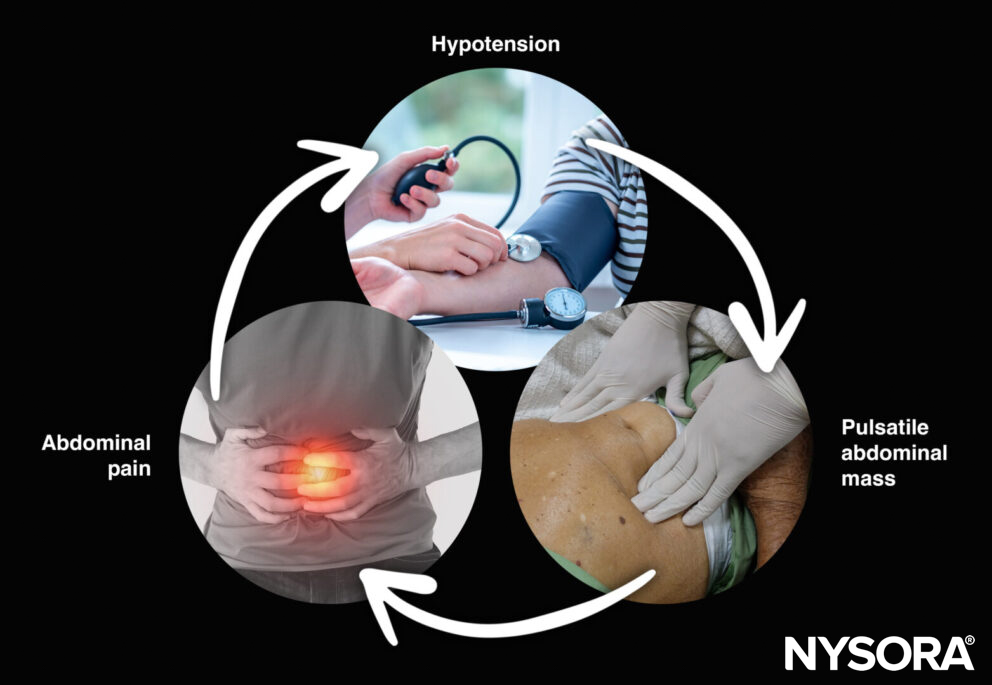
Triad of symptoms for AAA: Present in 25% of patients.
- A computerized tomography with intravenous contrast is indicated for inconclusive ultrasound findings.
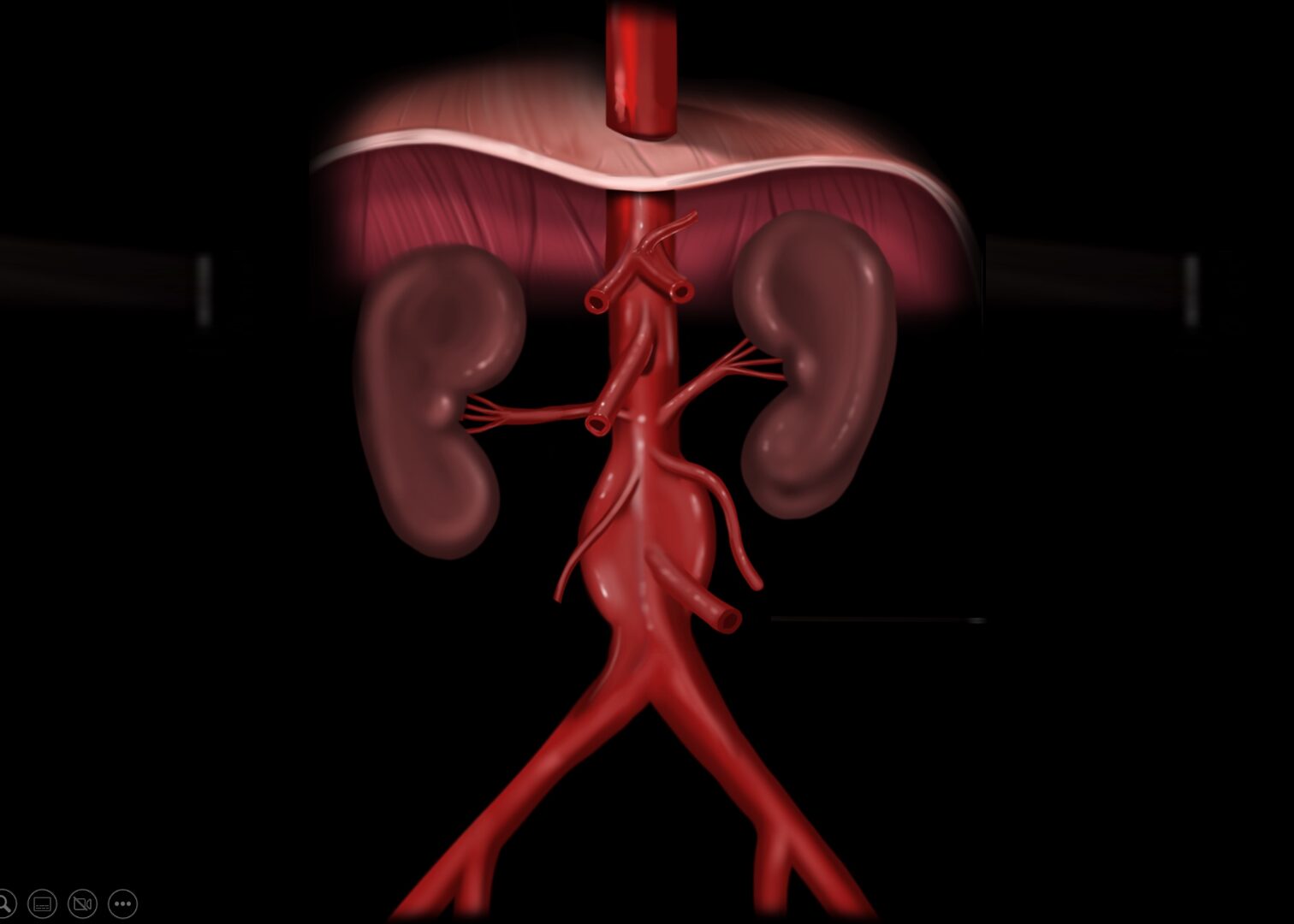
Functional anatomy
Note
The gonadal arteries and the inferior mesenteric artery are usually more difficult to observe with ultrasound.
The classification of AAA is made in relation to the branches of the aorta, usually the renal arteries.
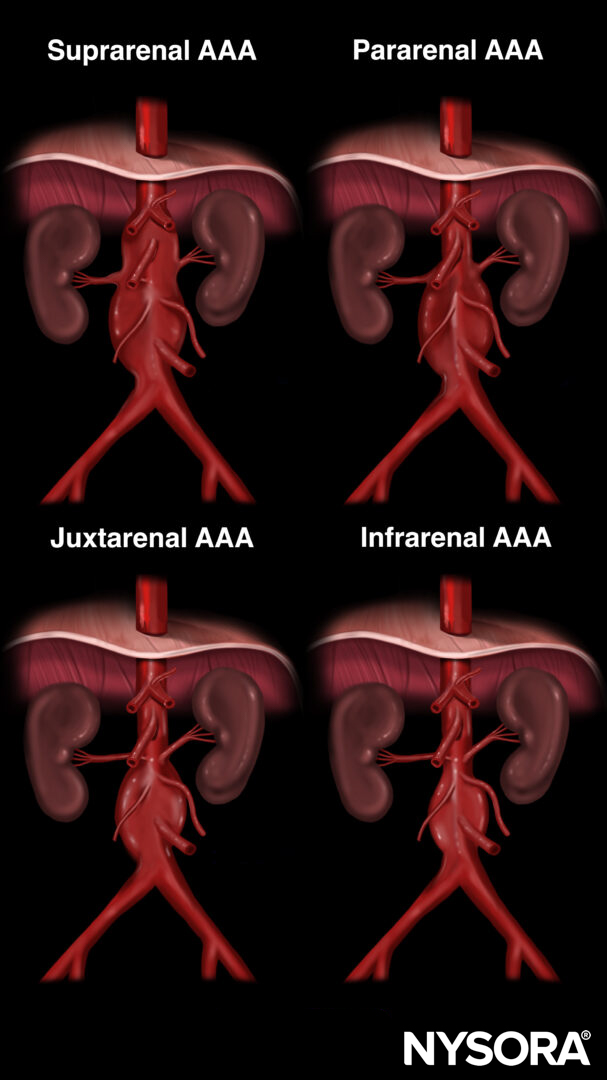
Classification of abdominal aortic aneurysms in relation to the renal arteries.
Note
Ultrasound, while a valuable diagnostic tool, has limitations in accurately pinpointing the precise location of an aneurysm relative to the aortic branches; it cannot always provide clear differentiation between proximal, mid, and distal abdominal aortic aneurysms. Ultrasound is a quick, non-invasive tool for detecting an aneurysm. However, further imaging modalities are necessary to provide a more complete anatomical understanding and guide surgical decision-making.
Different sections of the abdominal aorta:
- Proximal aorta: Celiac artery to superior mesenteric artery.
- Mid aorta: Superior mesenteric artery to renal arteries.
- Distal aorta: Below the renal arteries until the bifurcation into the iliac arteries.
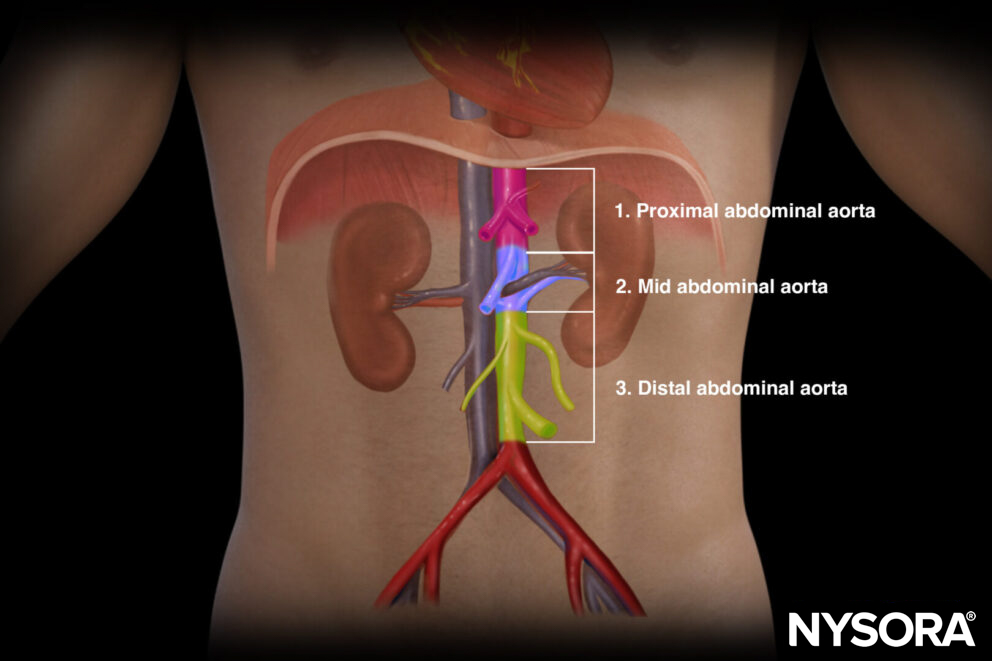
Proximal, mid, and distal sections of the abdominal aorta.
Notes
- 90 percent of all AAAs will occur distal to the renal arteries, i.e., infrarenal or distal aorta.
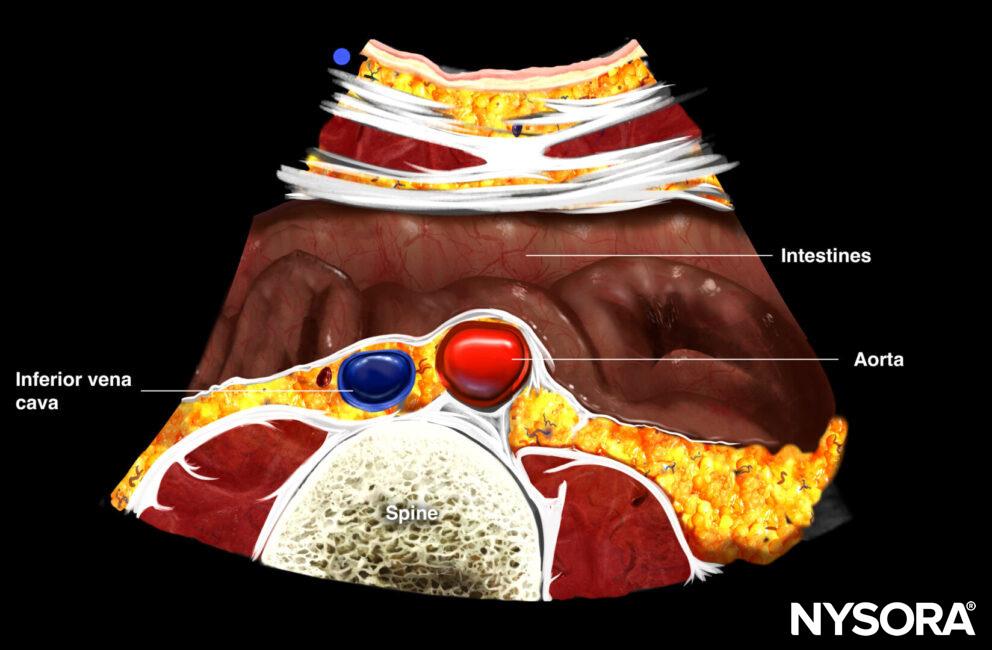
- Always distinguish the aorta from the inferior vena cava (IVC)
- Due to its close proximity to the aorta and the regular respiratory cycle, the IVC may mimic the aorta, pulsating with each breath. However, pulsed wave Doppler easily distinguishes the aorta’s pulsatile flow from the IVC’s venous flow.
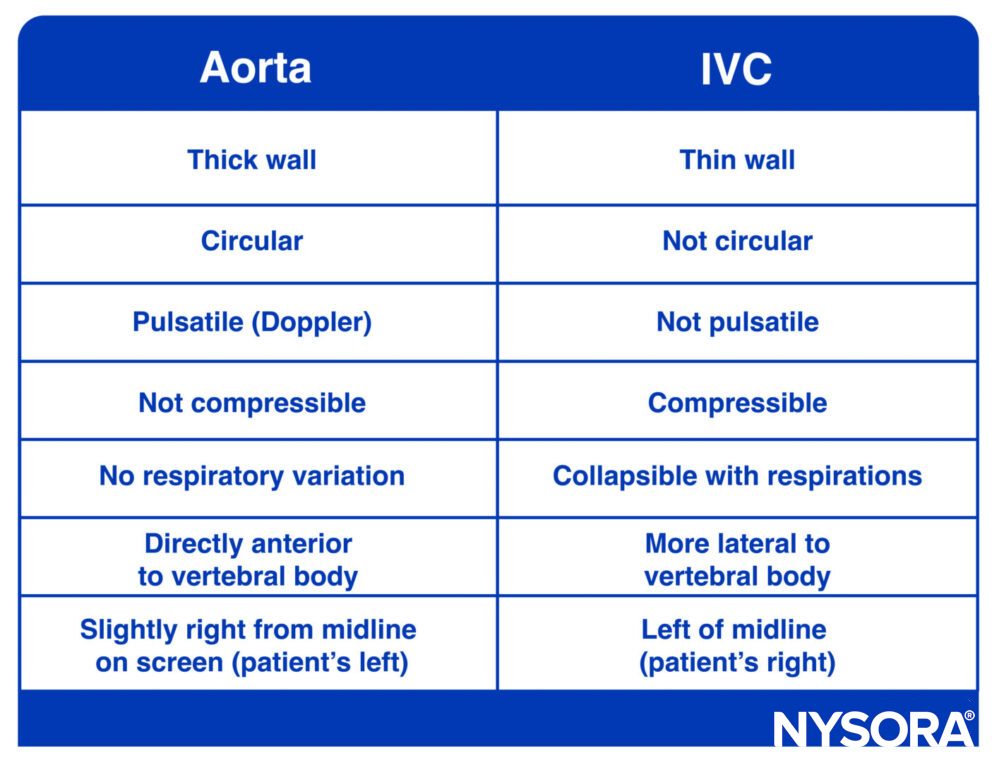
Differences between the aorta and IVC.
Ultrasound machine setup
- Transducer: Curvilinear (or a linear transducer in slim adults)
- Ultrasound preset: Abdominal
- Orientation: Index mark toward the right side of the patient
- Depth: 10 – 15 cm
Note
- Alternatively, a phased array transducer can be used.
- Deeper settings may be needed for large patients.
Patient position
Position the patient supine and completely flat.
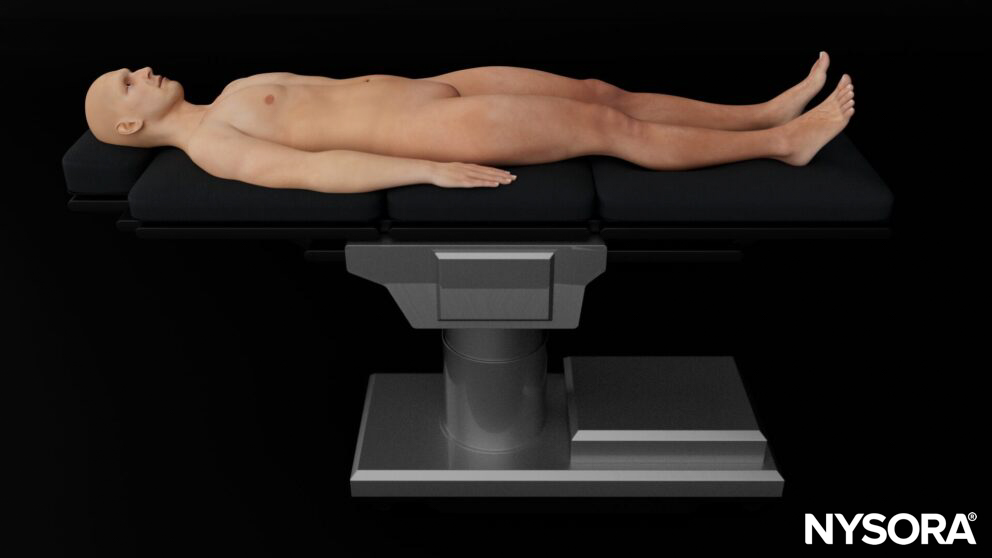
Note
Bend the knees if possible to relax the abdominal muscles.
Landmarks
Key landmarks to identify:
- Costal margin: Ribs in the upper abdomen may limit the acoustic window to the liver, spleen, and kidneys.
- Xiphoid process: The upper border of the abdomen.
- Linea alba: Midline of the abdomen that separates the rectus abdominis muscles and connects the xiphoid process with the pubic bone. The aorta is positioned slightly left to the midline.
- Umbilicus: Virtually separates the abdomen in four quadrants. The bifurcation of the aorta starts at the level of the 4th or 5th lumbar vertebral body. This correlates with the position of the umbilicus in adults with a normal body mass index.
- Pubic bone: Bony structure and lower margin of the abdomen. The pelvis starts at the level of the pubic bone.
- Anterior superior iliac spine: Bony structure that forms the lateral border of the pelvis.
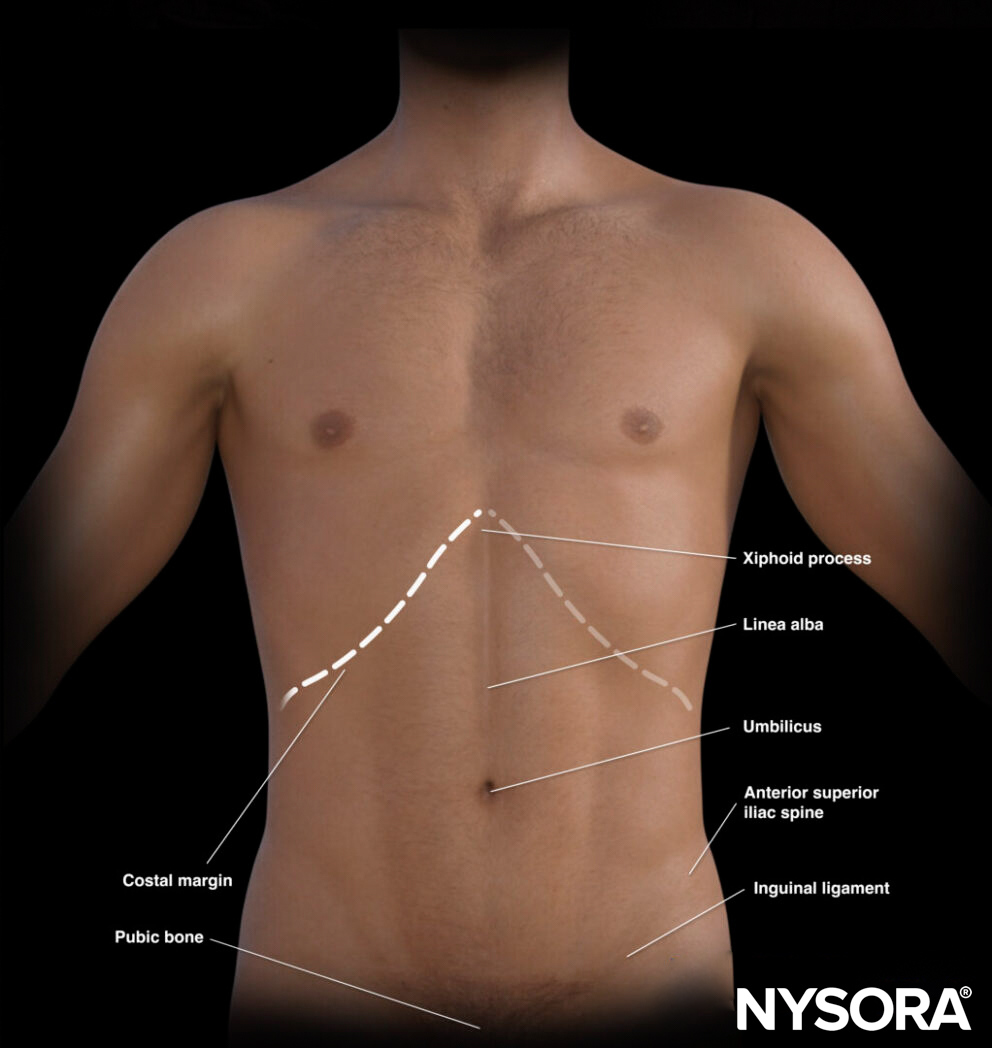
External landmarks of the abdomen.
The umbilicus divides the abdomen into quadrants, each of which contains specific organs:
- Right upper quadrant: Liver, gallbladder, kidney
- Left upper quadrant: Stomach, spleen, kidney
- Pelvic/paracolic region (lower quadrants): Colon, small intestines, rectum, bladder, male or female reproductive organs
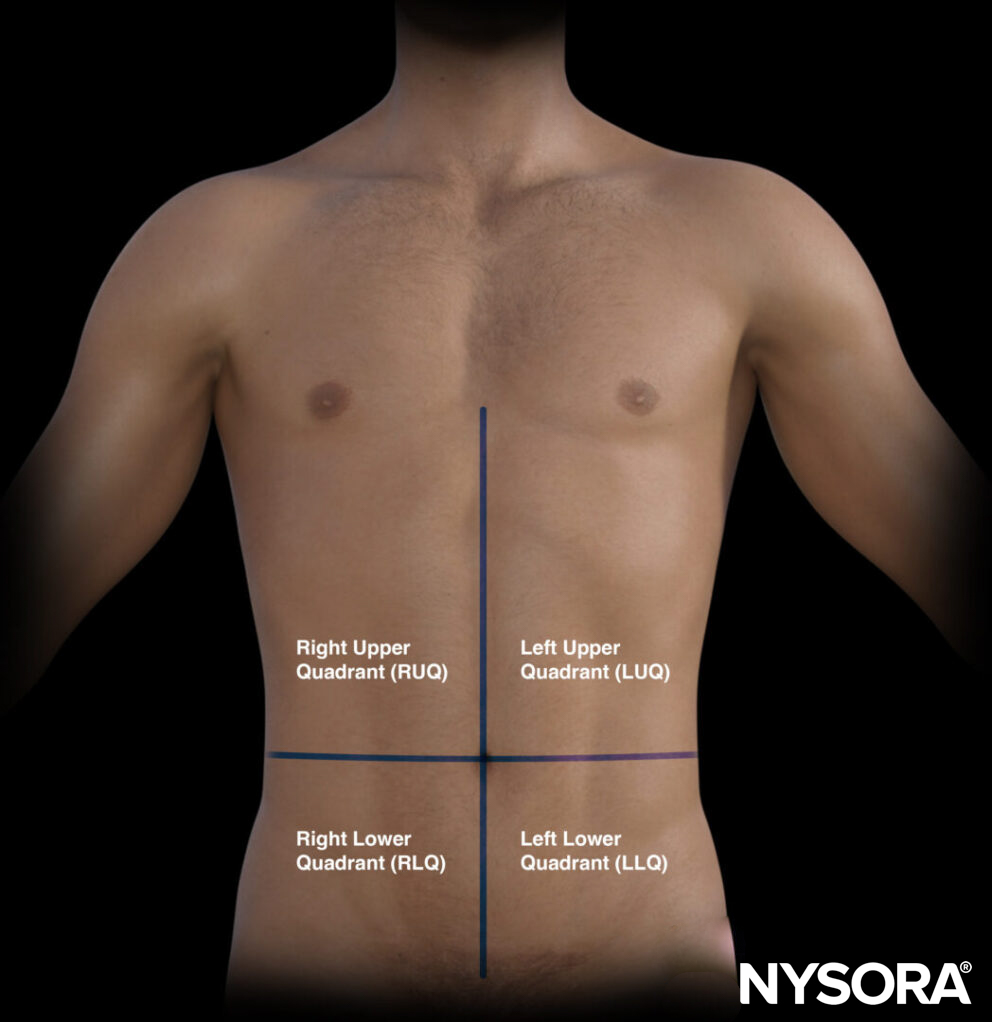
The four quadrants of the abdomen.
Transducer position
In the AAA scan, the transducer is positioned transversely underneath the xiphoid and on the midline or linea alba. The aorta usually positions itself slightly to the left of the midline.
Transducer position and scanning motion for AAA assessment.
Tips
- Make sure the transducer is placed perpendicular to the aorta.
- The aorta is slightly left of midline. Therefore, sliding or rocking the transducer towards the patient’s left may improve the ultrasound image.
Scanning
Scanning the abdominal aorta should include a systematic scan from proximal to distal, also called the sweep technique:
- Position the transducer in the starting position underneath the xiphoid.
- Identify the aorta, IVC, and the vertebral body with its acoustic shadow. Adjust depth if needed to identify these 3 structures.
- Sweep from cranial to caudal and focus on the diameter and morphology of the aorta. Three different sections should be distinguished: proximal, mid, and distal aorta.
- The maximal diameter from outer to outer wall should never exceed 3 cm for normal aorta findings.
Sweep technique for abdominal aorta scanning.
Four different cross-sectional views can be obtained to differentiate the proximal, mid, and distal abdominal aorta. At the level of the:
- Celiac artery (‘Seagull sign’)
- Renal artery and veins
- Distal or infrarenal aorta
- Bifurcation into the iliac arteries
Notes
- Always evaluate the entire aorta.
- Excessive transducer tilt may result in a falsely larger aortic diameter. To avoid this, the transducer should be placed perpendicular to the aorta for the most accurate measurement. Here’s an example:
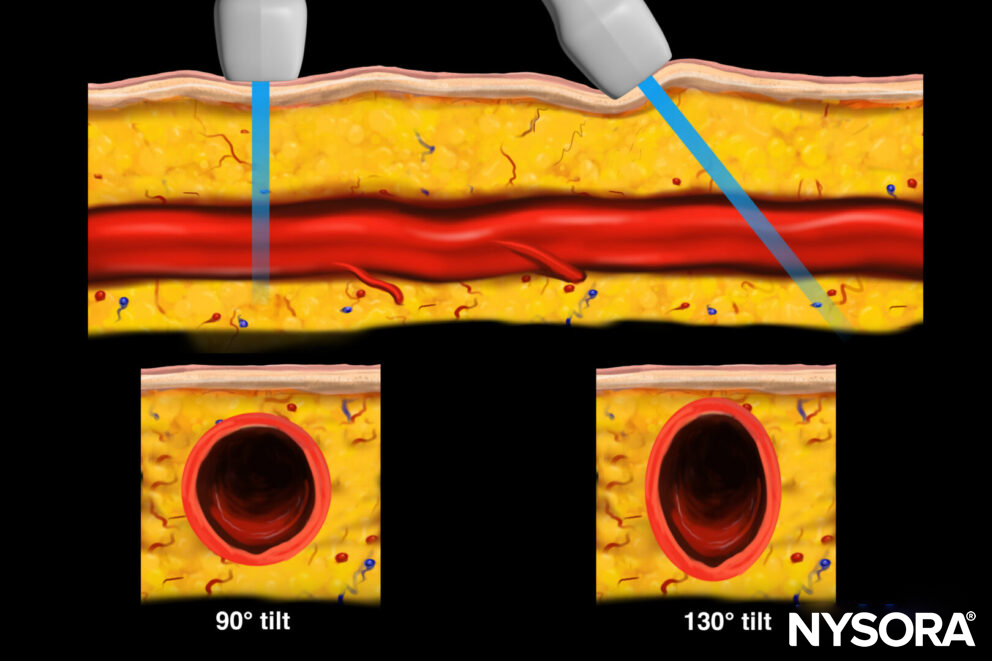
Transverse view ot the aorta with 90° and 130° tilt.
Notes
- Aneurysms often contain a thrombus. These thrombi in the wall can appear as the outer wall and falsely reduce the diameter. Only measuring the lumen, rather than the outer borders of the real aorta, may lead to misinterpretations or even missed aneurysms.
- Superpositioned bowel gas can obstruct imaging of the aorta: apply constant downward pressure and rock the transducer back and forth to displace the bowel loops and gas in the bowels.
Proximal aorta
Transverse view of proximal aorta: aorta, IVC, celiac artery: splenic and hepatic artery (seagull sign), spine, liver, gallbladder
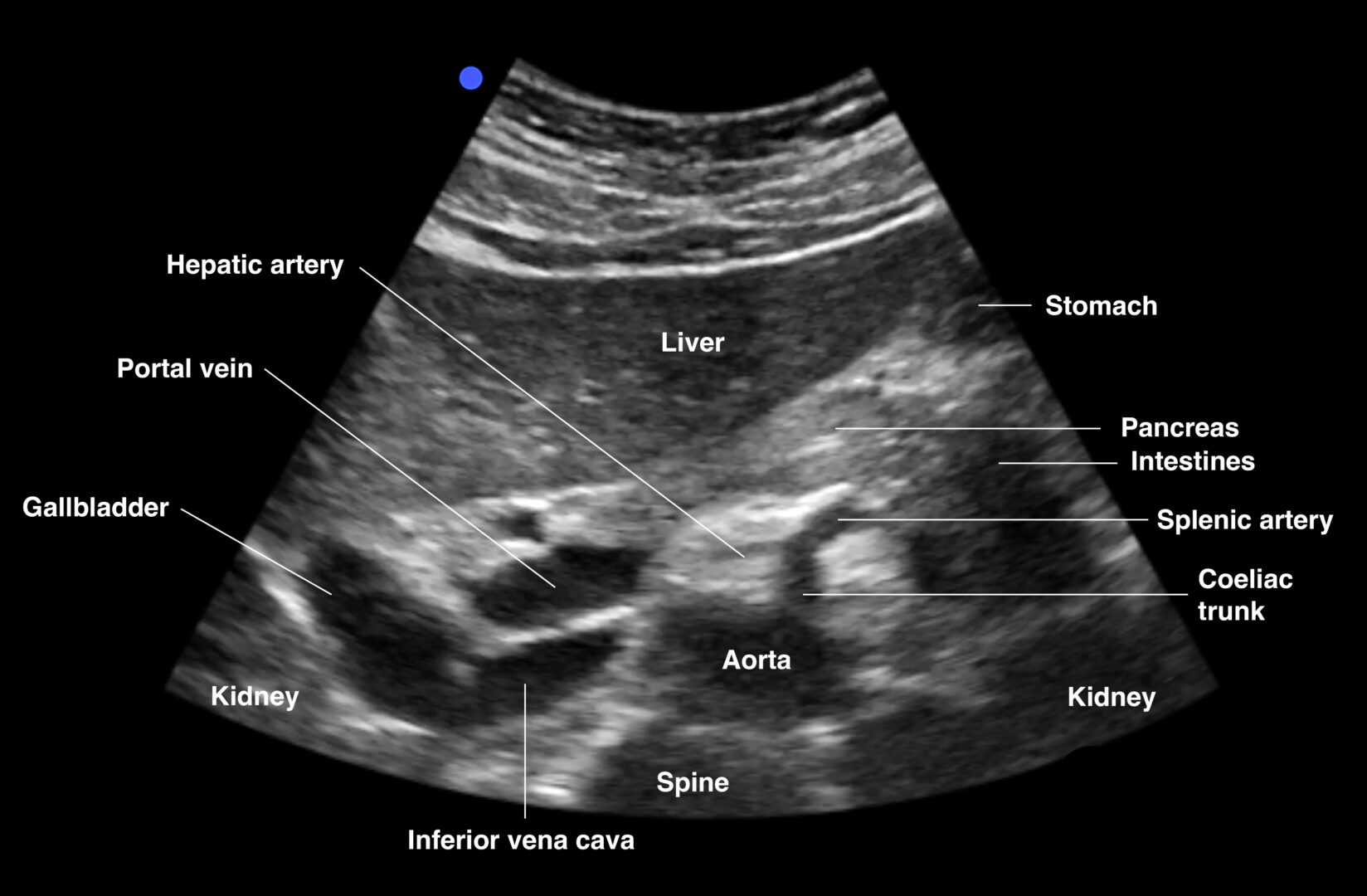
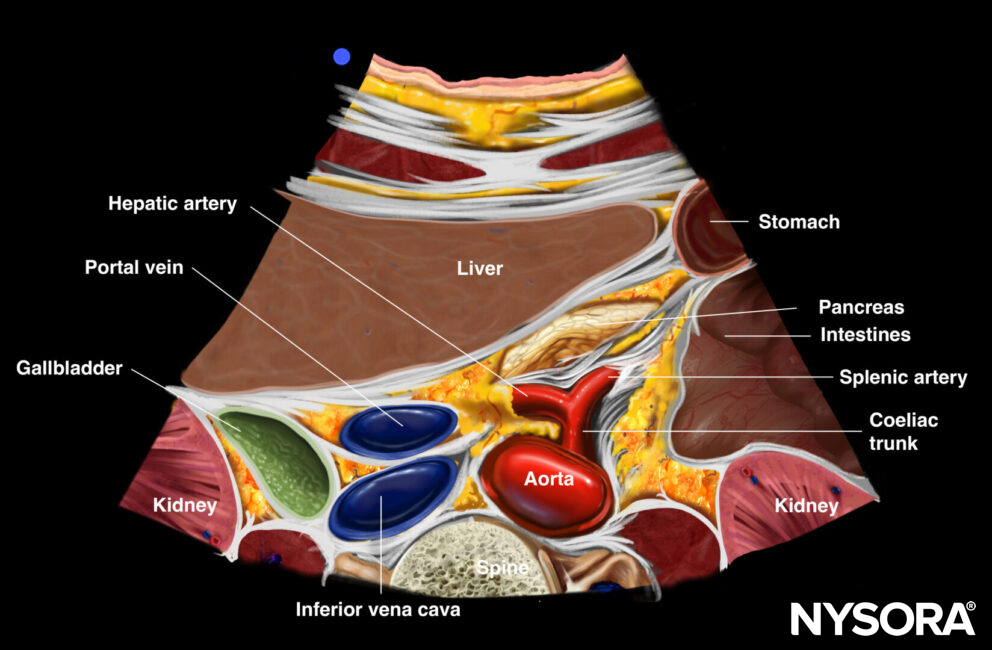
Transverse view of the proximal abdominal aorta.
Notes
- The left gastric artery is usually not visualized
- The seagull sign refers to the celiac trunk and its division into the hepatic and splenic arteries, which appear like the wings of a seagull.
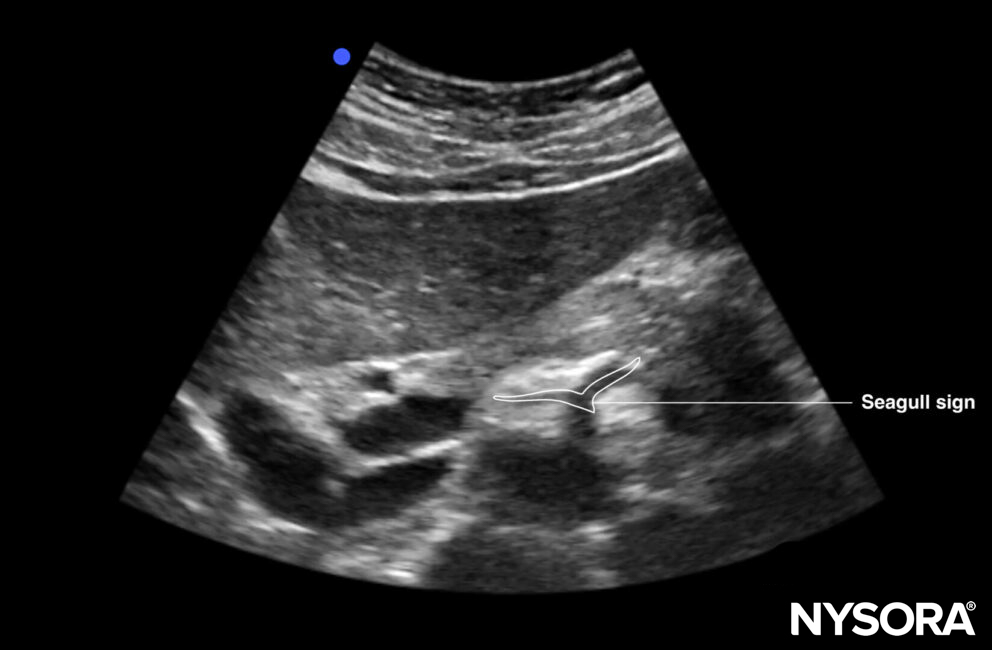
The seagull sign: the celiac trunk and its division into the hepatic and splenic arteries, which appear like the wings of a seagull.
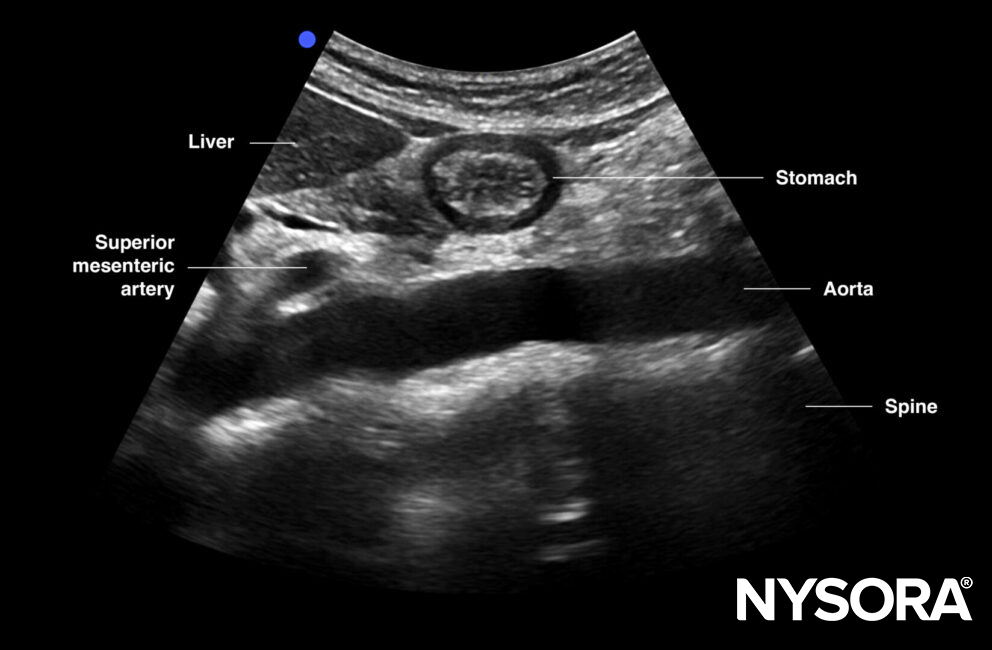
Mid aorta
Transverse view of mid aorta: superior mesenteric artery, aorta, renal vein, splenic vein (anterior to SMA), and left renal vein (between SMA and AA), spine, transverse colon, pancreas, liver
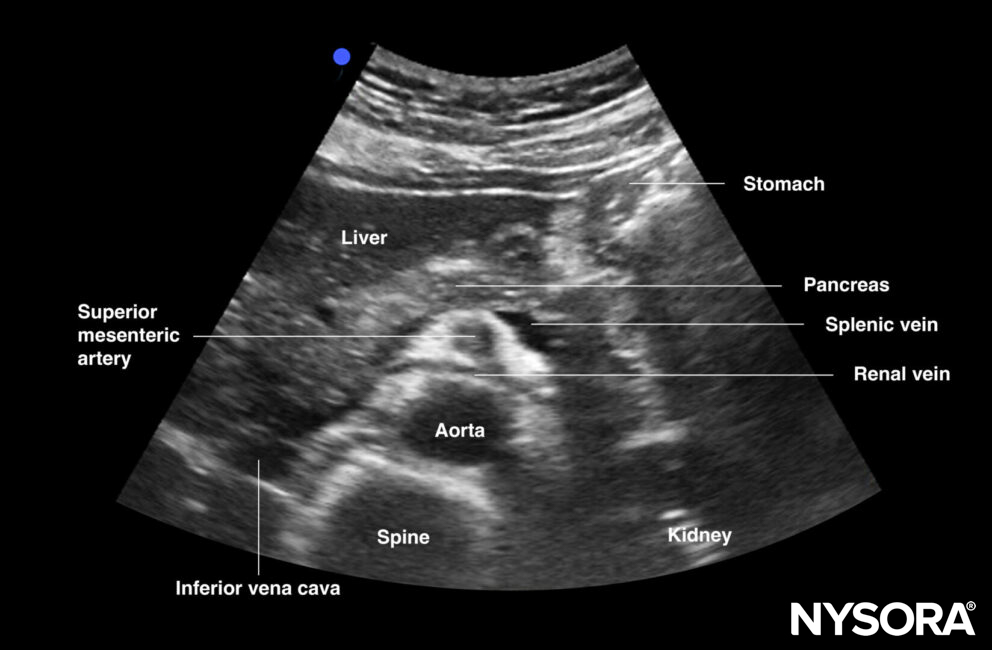
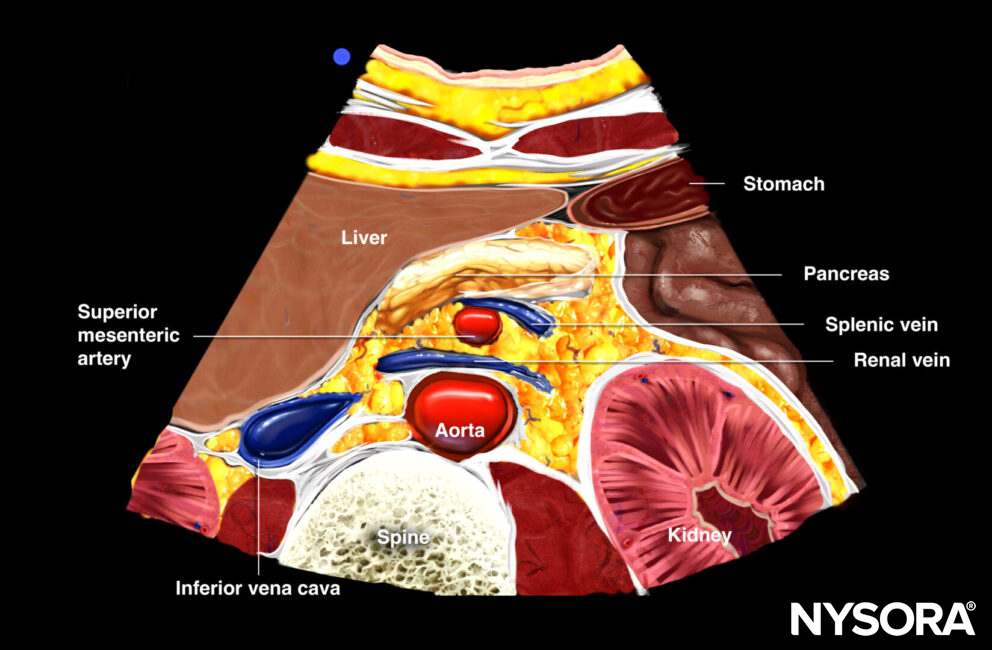
Transverse view of the mid abdominal aorta.
Distal aorta
Transverse view of the distal aorta: transition of the aorta into the bifurcation of the iliac arteries, iliac veins, spine, and intestines.
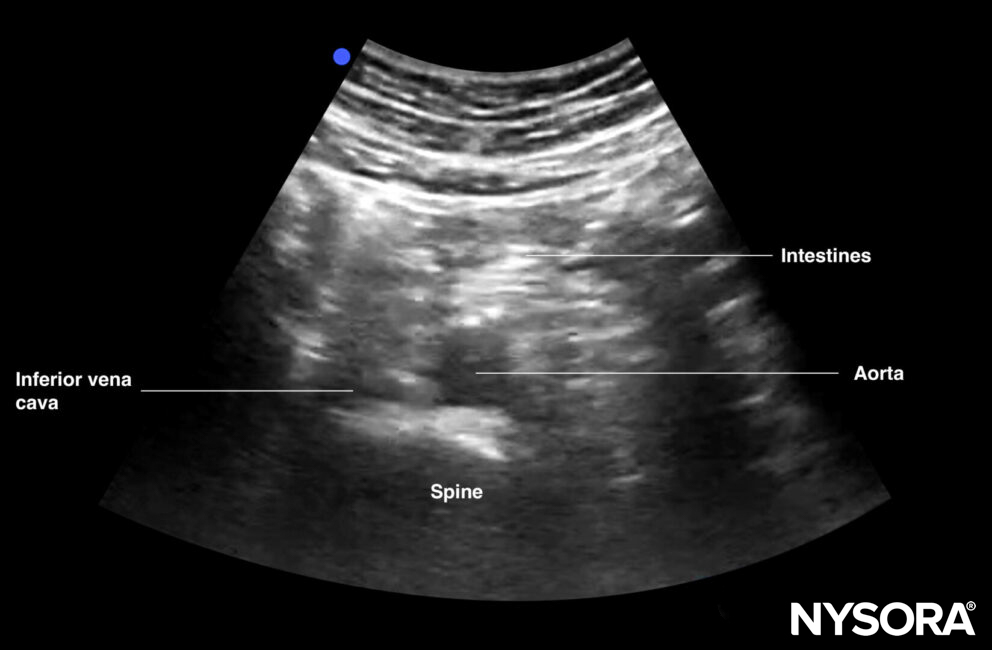
Transverse view of the distal aorta.
Notes
- The umbilicus corresponds to L4. This is the point where the aorta bifurcates into the iliac arteries.
- The umbilicus may be air-filled, leading to scattering artifacts. Use plenty of gel to fill the umbilicus and eliminate air for better images. Scanning distally or proximally toward the belly button while tilting the transducer may also help eliminate artifacts and visualize the aorta.
Interpretation
A normal abdominal aorta is 2 cm in diameter.
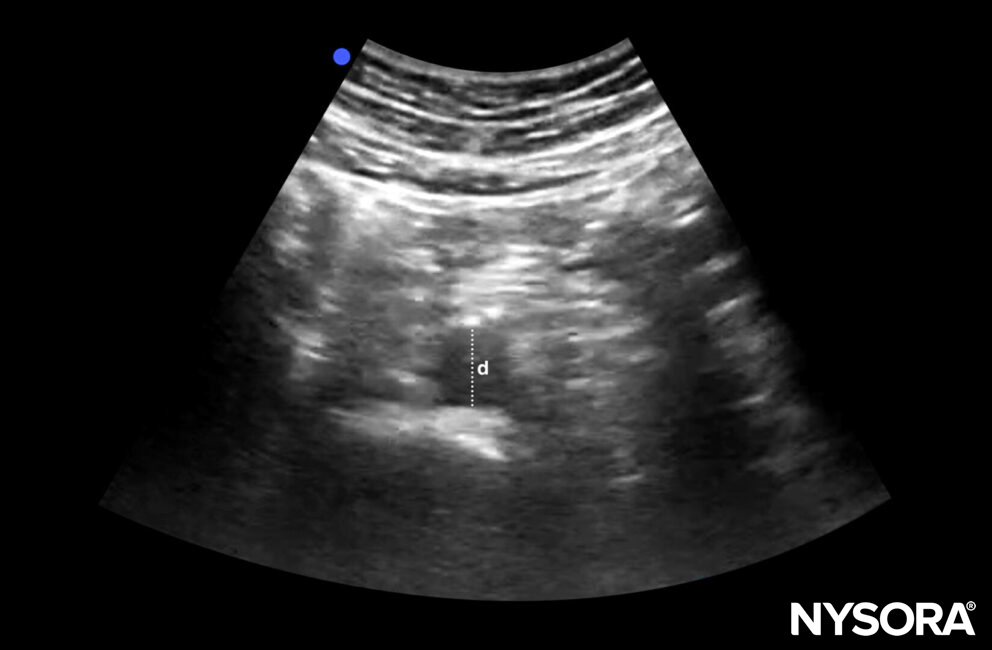
Diameter (d) of a normal abdominal aorta: 2 cm.
AAAs have a diameter of ≥ 3 cm
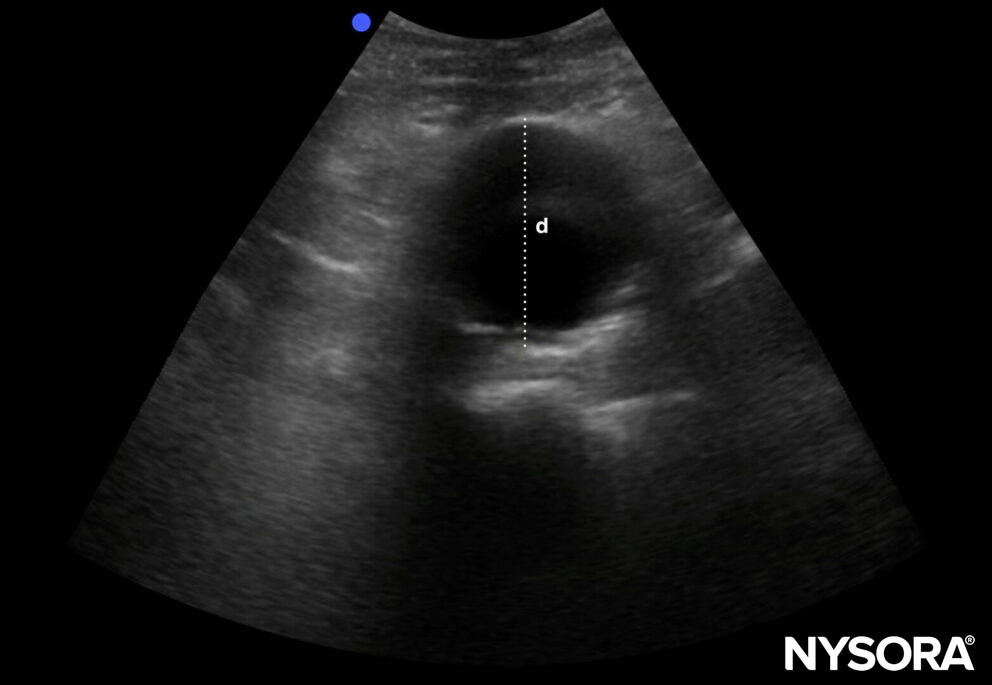
Diameter of an AAA: ≥ 3 cm.
Notes
- Iliac arteries ≥ 1,5 cm are abnormal
- The risk of rupture increases with the diameter of the aneurysm.
- AAAs of ≥ 5,5 cm have an increased risk of rupture and should be considered as an emergency. (co-existing other pathology, such as Marfan’s disease, decreases the risk cut-off to < 5 cm)
- An additional sagittal view can be added to increase sensitivity or as an add-on.
Sagittal view of the abdominal aorta.
Longitudinal/sagittal view of aorta: celiac artery, superior mesenteric artery branching of anteriorly from the aorta, liver, spine
If a dissection flap is observed, aortic dissection is ruled in. However, aortic dissection is not ruled out when no flap is seen.
Note
Do not forget to focus on the outer borders of the aorta.
Decision making
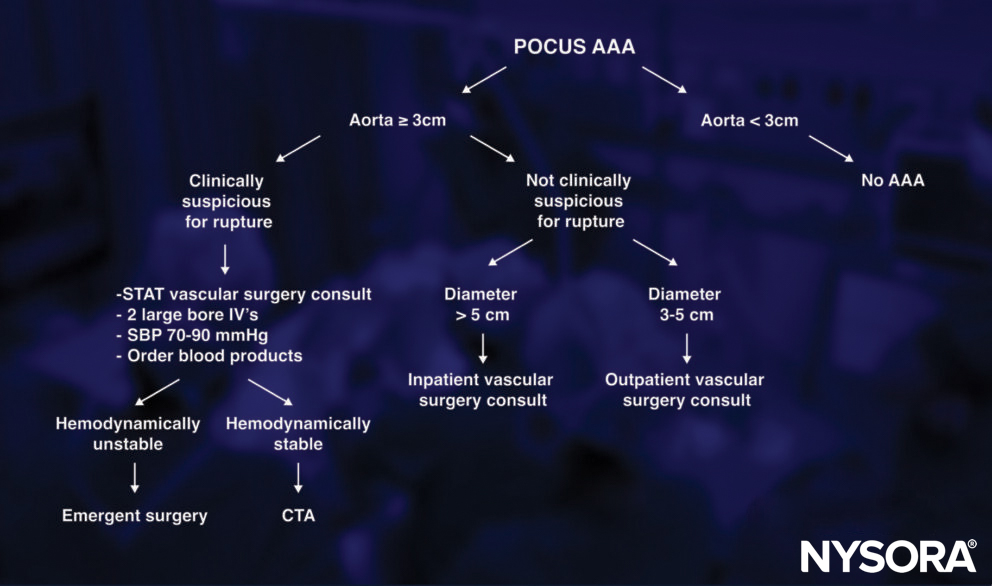
Notes
- Ultrasound’s sensitivity for ruptured AAA is low. The aorta is a retroperitoneal vascular structure. A leak from the aorta and smaller volumes of retroperitoneal blood may be more difficult to visualize.
- A patient with suspected ruptured AAA should be evaluated for the presence of free fluid. Go to the ‘abdominal free fluid course’ to learn how to do this scan.
Clinical updates
Fernando et al. (Academic Emergency Medicine, 2022) performed a systematic review and meta-analysis of 20 studies (n=2,077) and found that classic rAAA features have poor sensitivity: abdominal pain 61.7%, back pain 53.6%, syncope 27.8%, hypotension 30.9%, and pulsatile mass 47.1%, meaning the absence of these findings cannot exclude rupture. CTA demonstrated good but imperfect accuracy (sensitivity 91.4%, specificity 93.6%), while PoCUS was highly accurate for detecting AAA in suspected cases (sensitivity 97.8%, specificity 97.0%) but cannot directly confirm rupture, supporting its role in rapid risk stratification rather than definitive diagnosis.
- Fernando SM, Tran A, Cheng W, et al. Accuracy of presenting symptoms, physical examination, and imaging for diagnosis of ruptured abdominal aortic aneurysm: Systematic review and meta-analysis. Acad Emerg Med. 2022;29(4):486-496.