Etiology
Intracranial hypertension can be caused by
- Traumatic brain injury
- Stroke
- Ruptured cerebral aneurysm
- Infection (abscess, meningitis, encephalitis)
- Tumor
- Arterial hypertension
- Unknown reason (idiopathic)
View
Transducer position for transcranial Doppler examination of intracranial hypertension.
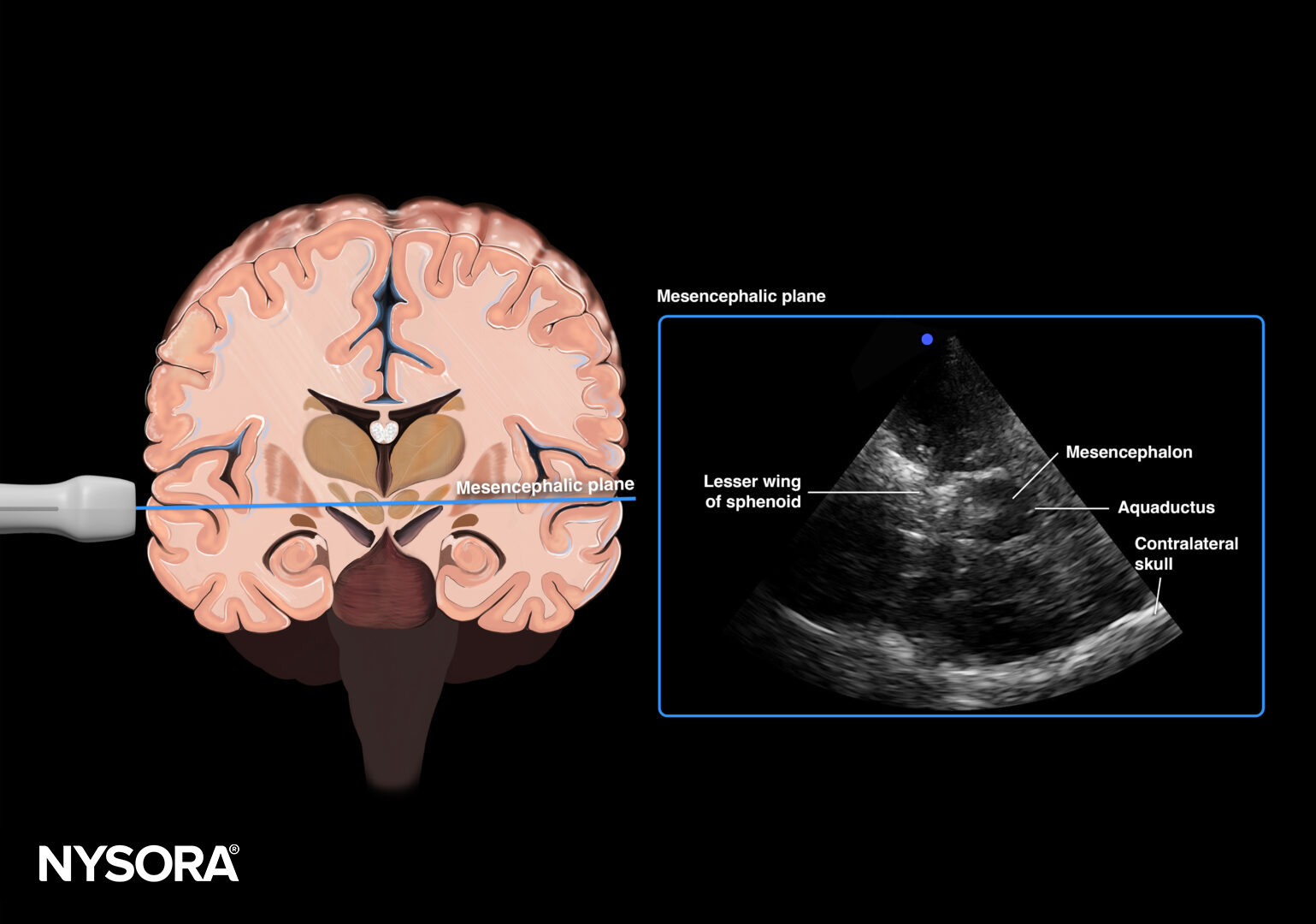
Mesencephalic plane.
Assessment
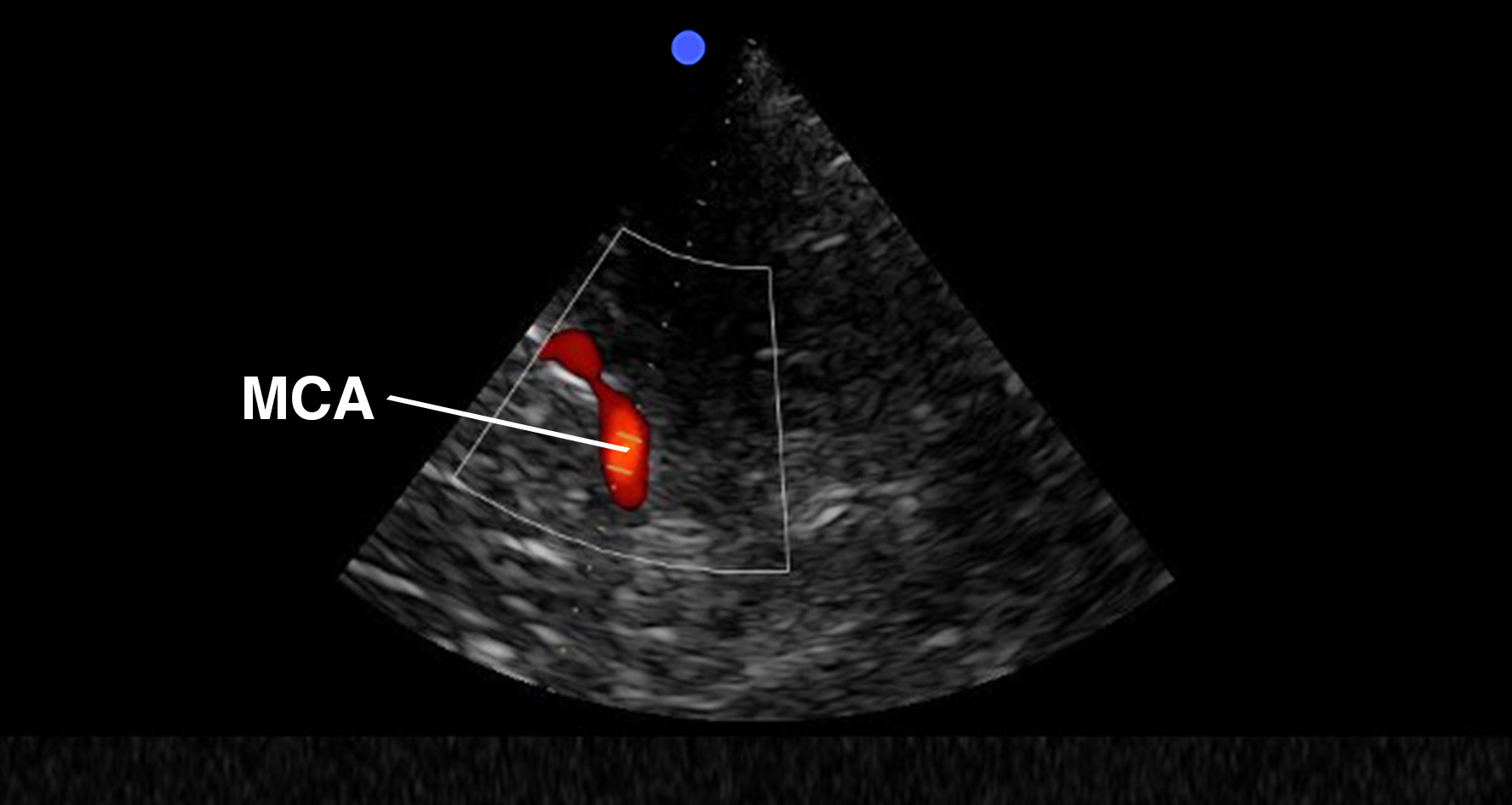
Use the mesencephalic plane and activate pulsed wave Doppler. Position the Doppler gate on the middle cerebral artery (MCA) and trace the flow velocities.
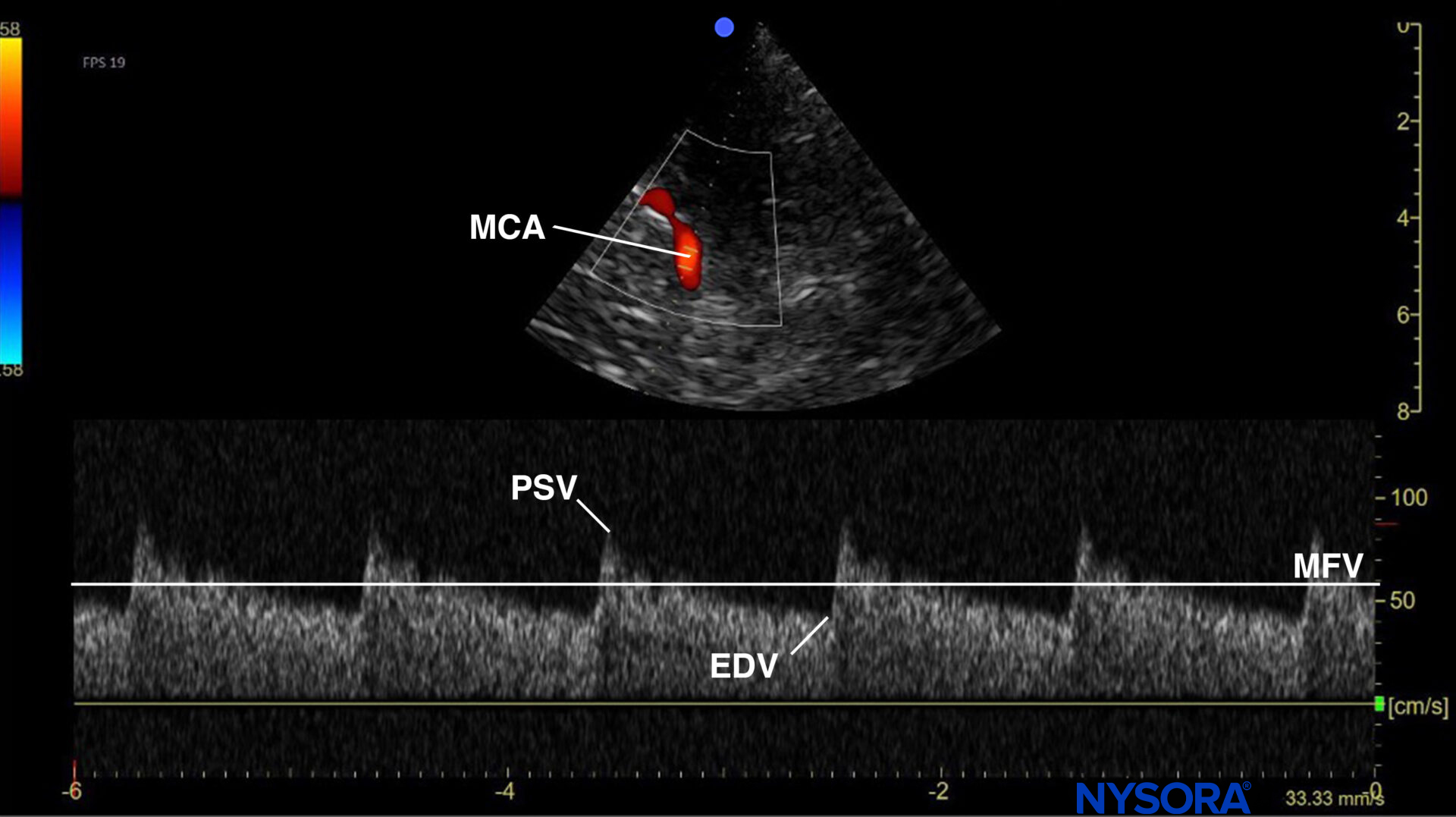
Mesencephalic plane pulsed wave Doppler with the Doppler gate on the middle cerebral artery (MCA). Evaluation of flow velocities in the MCA. PSV, peak systolic velocity; EDV, end-diastolic velocity; MFV, mean flow velocity.
Tip
When using pulsed wave Doppler, the flow toward the transducer is the flow above the baseline, while the flow away from the transducer is below.
Increased intracranial pressure (ICP) will affect cerebral blood vessel resistance and, consequently, cerebral blood flow velocities. Detection of a high resistance waveform or a high pulsatility index (PI) (= Gosling index) suggests a raised ICP. The pulsatility index equals the peak systolic velocity (PSV) minus the end diastolic velocity (EDV) divided by the mean flow velocity (MFV).
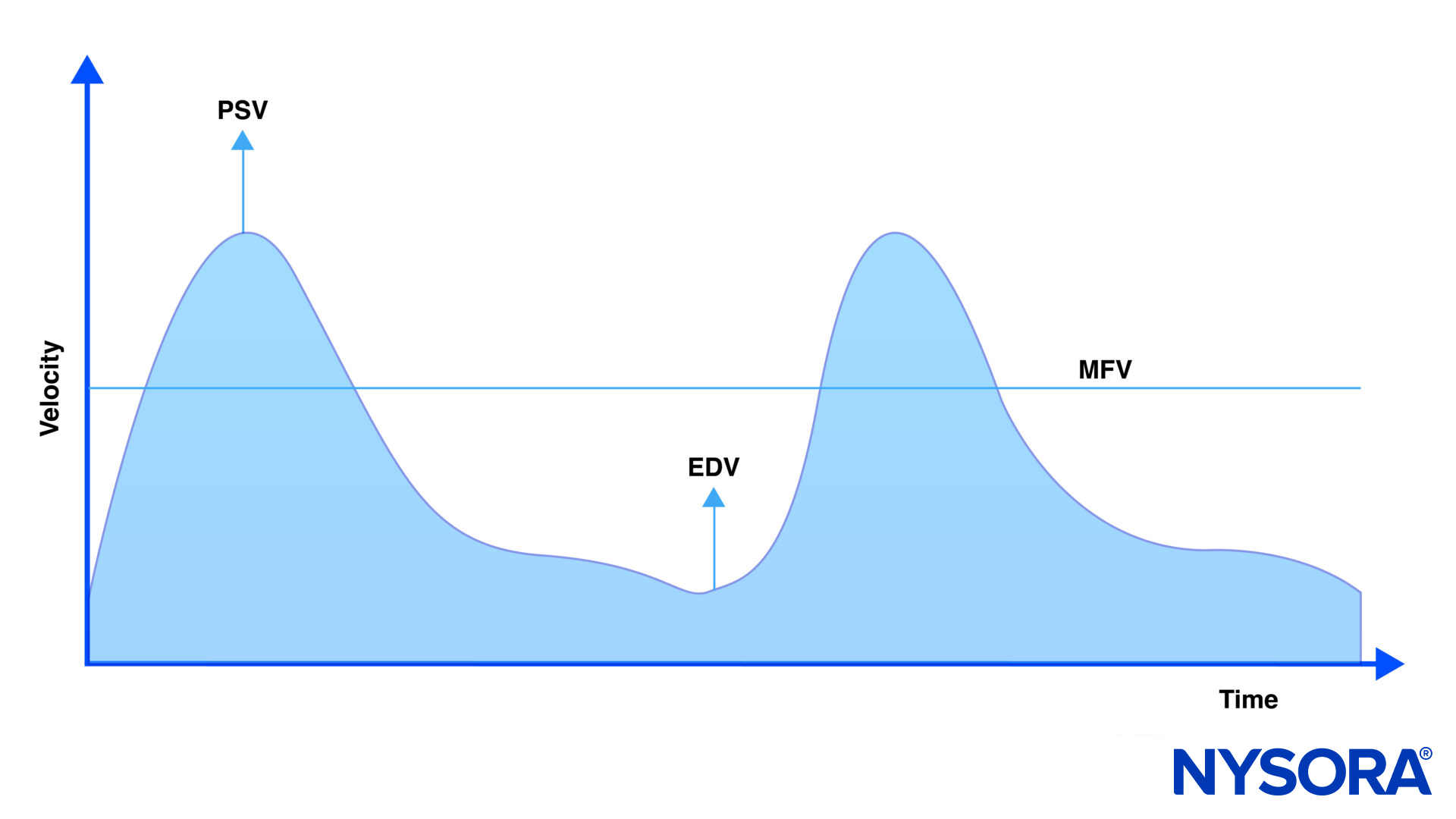
Middle cerebral artery flow velocity over time. PSV, peak systolic velocity; EDV, end-diastolic velocity; MFV, mean flow velocity.
PI = (PSV – EDV)/ MFV
- A normal PI usually ranges between 0.5 and 1.
- A PI > 1.2 should raise suspicion of increased intracranial pressure.
Note
Changes in PI are not dependent solely on changes in ICP, but also on cerebral perfusion pressure (CPP), arterial blood pressure and its pulsatility, hematocrit, and variations in partial pressure of CO2.
Tips
- Estimated ICP approximates the PI x 10 (more exact formula: ICP = 10.93 x PI – 1.28)
- The pulsatility index is a better indicator for cerebral perfusion than the resistance index (RI) (=Pourcelot index) since it uses the mean flow velocity and not the systolic flow velocity.
- RI = (PSV + EDV)/ PSV
- Many ultrasound machines will automatically calculate the PI if a TCD mode is used.
Clinical updates
- Rasulo et al. (Critical Care, 2022) conducted the prospective multicenter IMPRESSIT-2 study (262 patients; 687 paired measurements) comparing TCD-derived ICP (ICPtcd) with invasive ICP monitoring and found that ICPtcd has a high negative predictive value for excluding intracranial hypertension: NPV 91.3% at >20 mmHg, 95.6% at >22 mmHg, and 98.6% at >25 mmHg. The optimal ICPtcd threshold to rule out intracranial hypertension was 20.5 mmHg (AUC 0.76), with moderate sensitivity (70%) and specificity (72%), and a mean bias of −3.3 mmHg versus invasive ICP, supporting TCD as a screening tool to exclude, though not confirm, intracranial hypertension when invasive monitoring is unavailable.
-
- Rasulo FA, Calza S, Robba C, et al. Transcranial Doppler as a screening test to exclude intracranial hypertension in brain-injured patients: the IMPRESSIT-2 prospective multicenter international study. Crit Care. 2022;26(1):110.