Risk factors and signs
Risk factors
- Recent (orthopedic) surgery
- Immobilization
- Cardiac illness
- Hypercoagulation disorders
- Smoking, obesity, use of anticonception, …
Signs
- Localized pain
- Asymmetric edema
- Colored skin
Tip
Patients with symptoms of DVT and pulmonary symptoms such as acute dyspnea or pain on chest pain require an immediate cardiac ultrasound to assess the right ventricle and exclude pulmonary emboli. This should be performed before the DVT assessment.
Functional anatomy
Zones of interest for DVT scan: Femoral and popliteal area
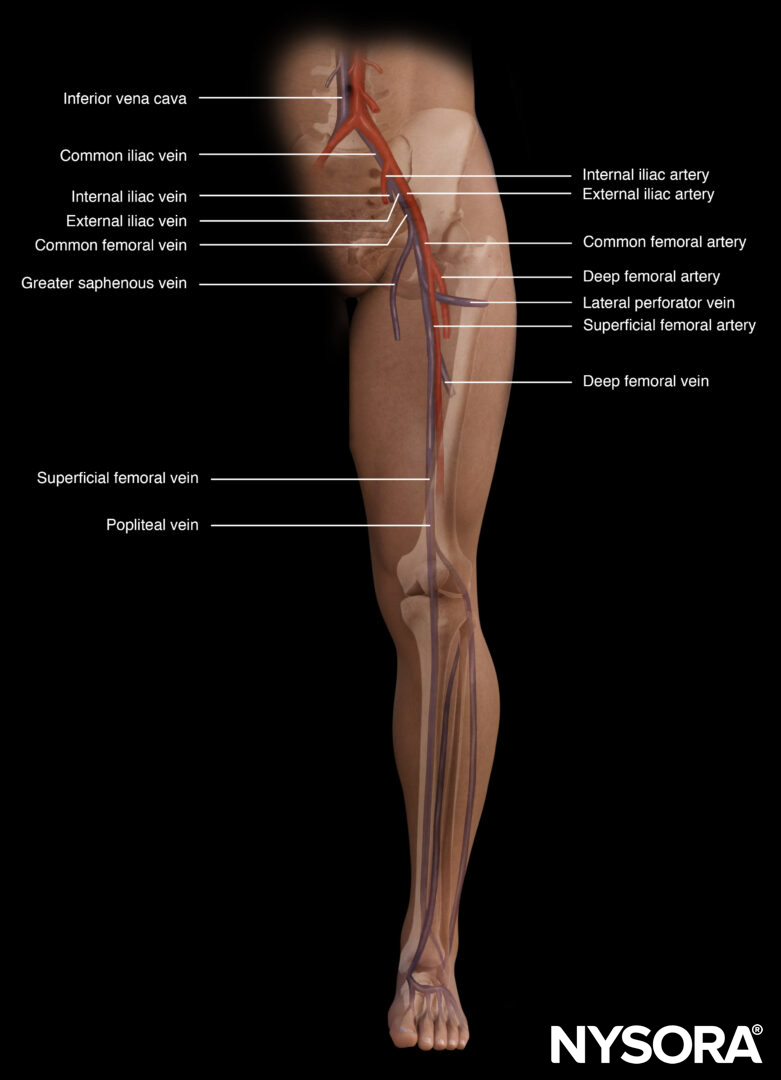
Important vascular structures of the lower extremity.
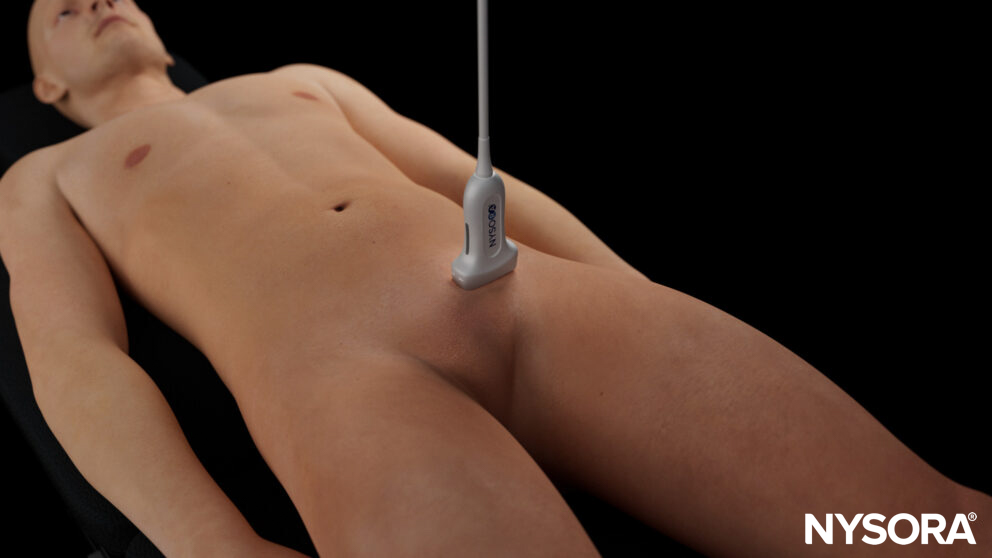
Patient position
Supine position with the leg in extension and exorotation.

Leg in flexion for the popliteal assessment.
![]()
Technique
- Start scanning at the level of the inguinal fold with a linear transducer.
For the popliteal position, the leg is flexed to allow scanning of the popliteal fossa.

- Slowly scan distally and assess compressibility every 1-2 cm.
- Pay special attention to the 5 visualization key points since these are more likely to visualize clots.
-
- Common femoral vein
- Bifurcation of the common femoral vein and the saphenous vein
- Bifurcation of the common femoral vein and the lateral perforator vein
- Bifurcation of the superficial femoral vein and the deep femoral vein
- Popliteal vein
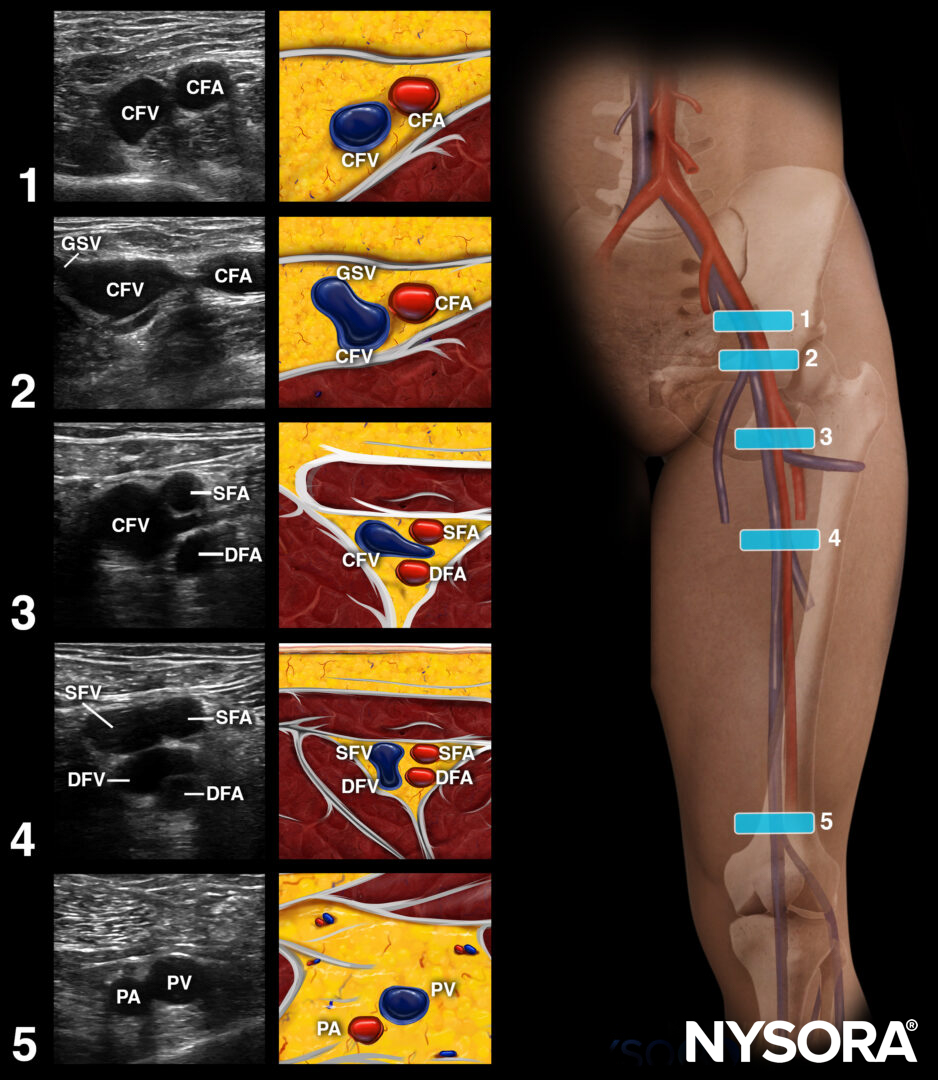
CFV, common femoral vein; CFA, common femoral artery; GSV, great saphenous vein; SFA, superficial femoral artery; DFA, deep femoral artery; SFV, superficial femoral vein; DFV, deep femoral vein; PA, popliteal artery; PV, popliteal vein.
- A non-compressible vein is pathognomonic for DVT.
Tips
- Ultrasound has a high level of accuracy in detecting DVT.
- The thrombus does not need to obstruct the lumen of the vein completely; it can also be partially obstructed.
Clinical updates
Zaki et al. (The Ultrasound Journal, 2024) conducted a systematic review and meta-analysis of 26 ED-based studies (n≈3350) and found that emergency physician–performed POCUS has high diagnostic accuracy for DVT: pooled sensitivity/specificity were 92.3%/96.9% for 2-point compression and 89.2%/92.7% for 3-point compression, while complete and whole-leg protocols achieved ~100% sensitivity and 97% specificity. Meta-regression showed heterogeneity related to reference standard and operator factors, but diagnostic performance remained high even with limited training, particularly when supervised by attending physicians. Importantly, POCUS significantly reduced time from triage to diagnosis compared with radiology-performed studies, supporting its use as a first-line ED imaging strategy for suspected DVT.
- Zaki HA, Albaroudi B, Shaban EE, et al. Deep venous thrombosis (DVT) diagnostics: gleaning insights from point-of-care ultrasound (PoCUS) techniques in emergencies: a systematic review and meta-analysis. Ultrasound J. 2024;16(1):37.