Indications
The BLUE (Bed Lung Ultrasound in Emergency) protocol can be used to troubleshoot the etiology of acute respiratory failure and differentiate between pneumothorax, pneumonia, pulmonary embolism, pulmonary edema, and COPD or asthma.
The BLUE protocol
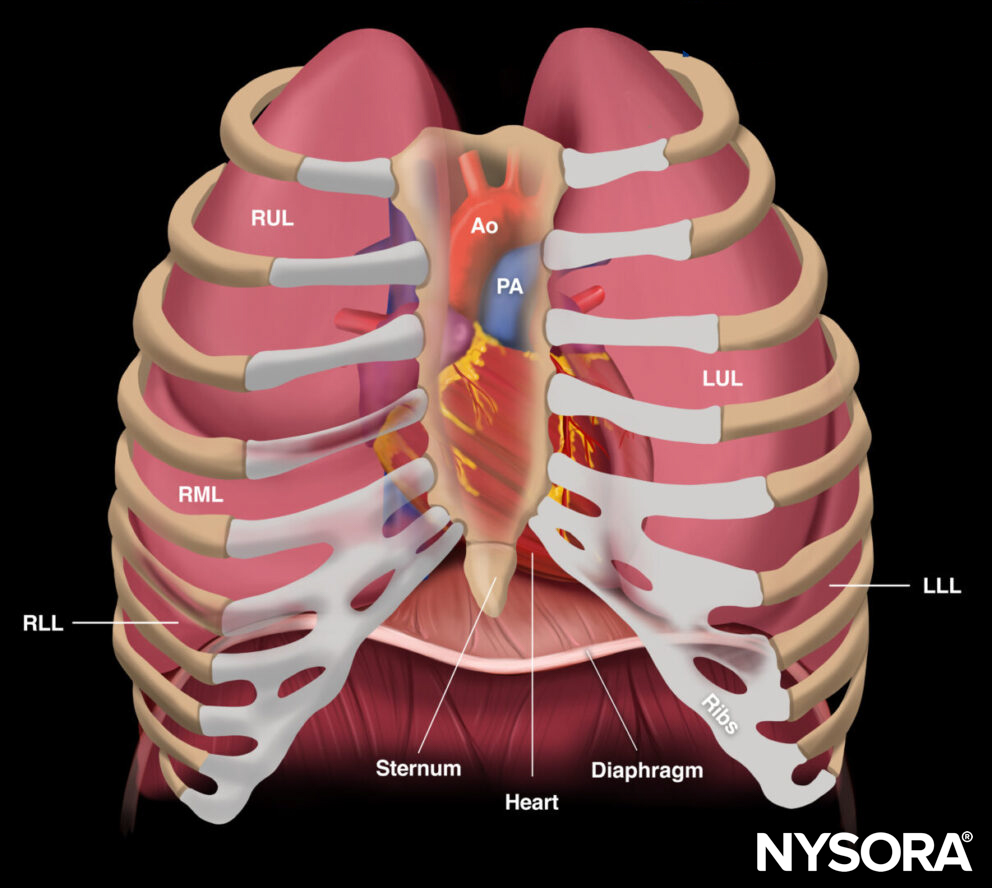
1. Scan the 2 BLUE points on the left and right thorax.
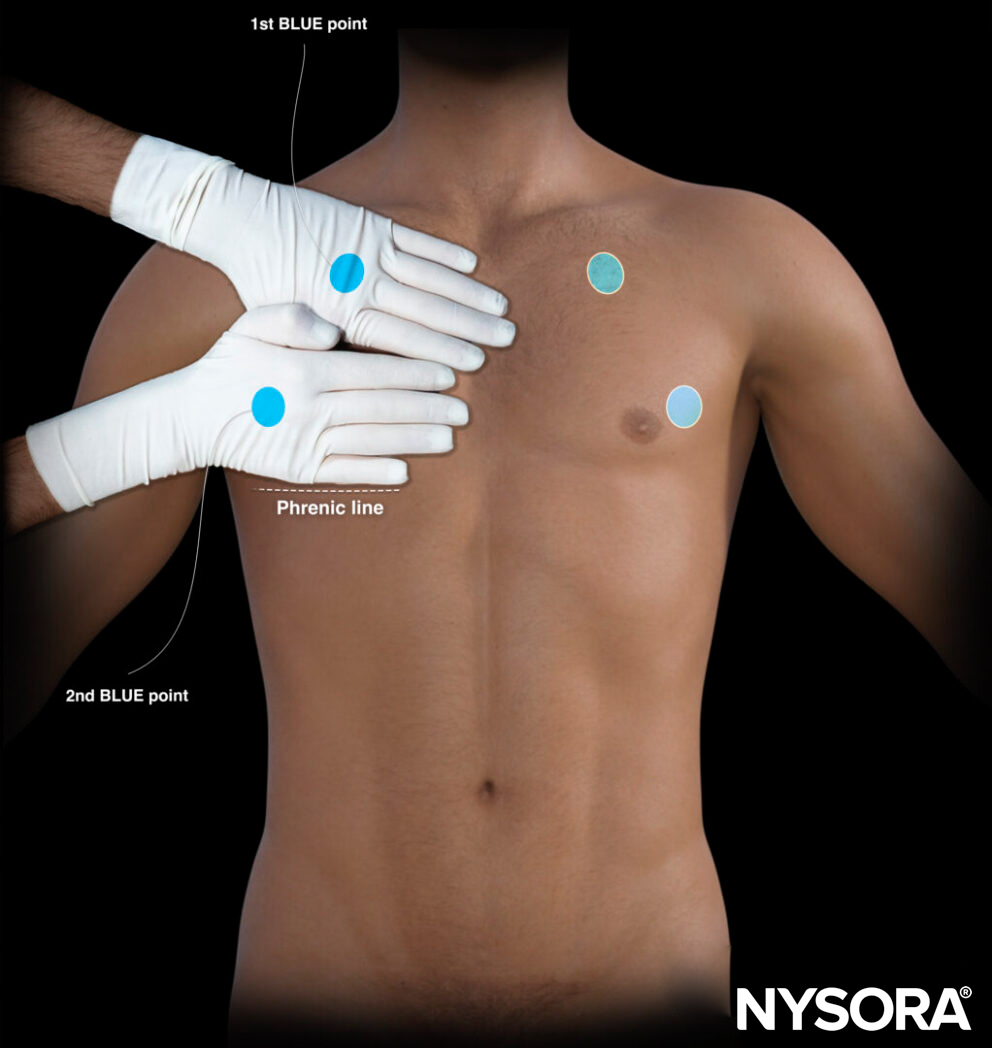
BLUE points on the left and right thorax.
2. Evaluate the presence of lung sliding (the absence of lung sliding will be indicated with a prime mark or ‘).
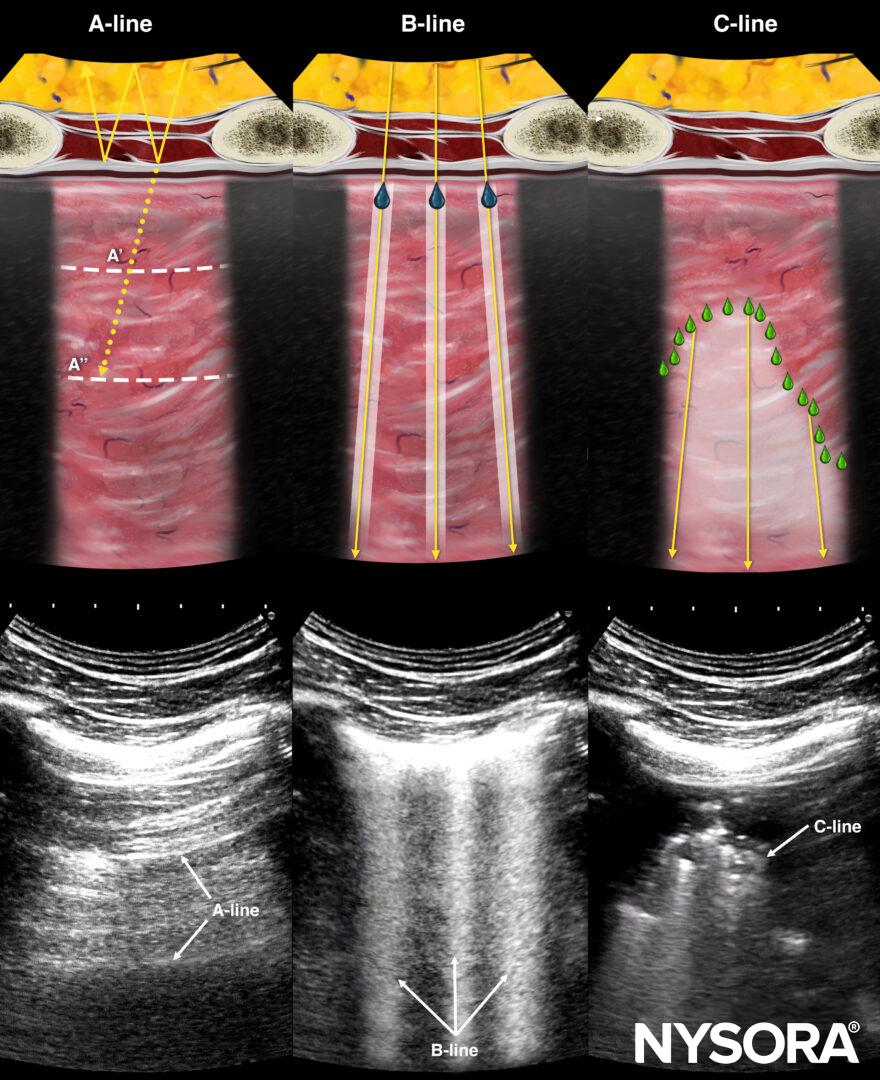
3. Check for lung artifacts (A-lines, B-lines, C-lines).
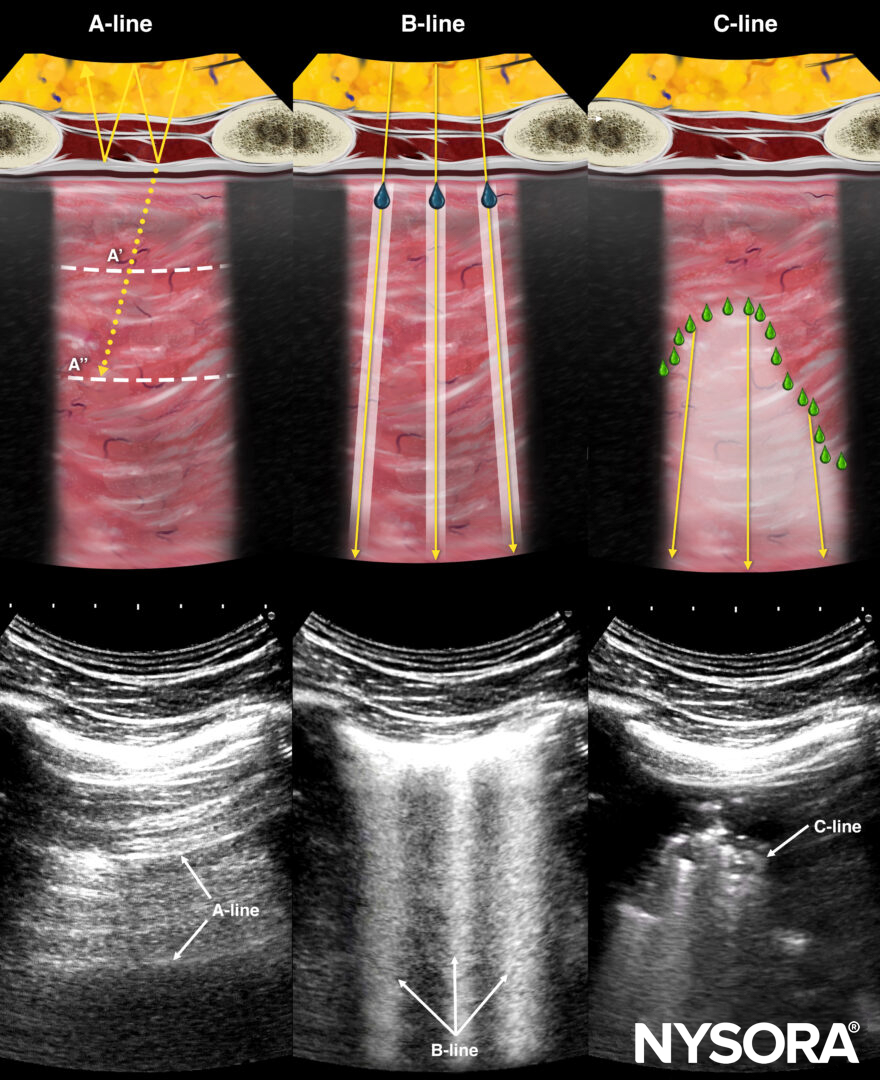
Relevant artifacts for the BLUE protocol.
4. Determine the profile based on the findings in all four BLUE points:
- A-profile: A-lines in all 4 BLUE points.
- B-profile: 3 or more B-lines in all 4 BLUE points.
- C-profile: A consolidation (C-line) is present in one of the BLUE points.
- A/B-profile: Various findings of A-lines and 3 or more B-lines in the four BLUE points.
5. An A-profile or A’-profile requires further scanning:
- In case of an A-profile, thrombosed veins need to be excluded using the DVT protocol.
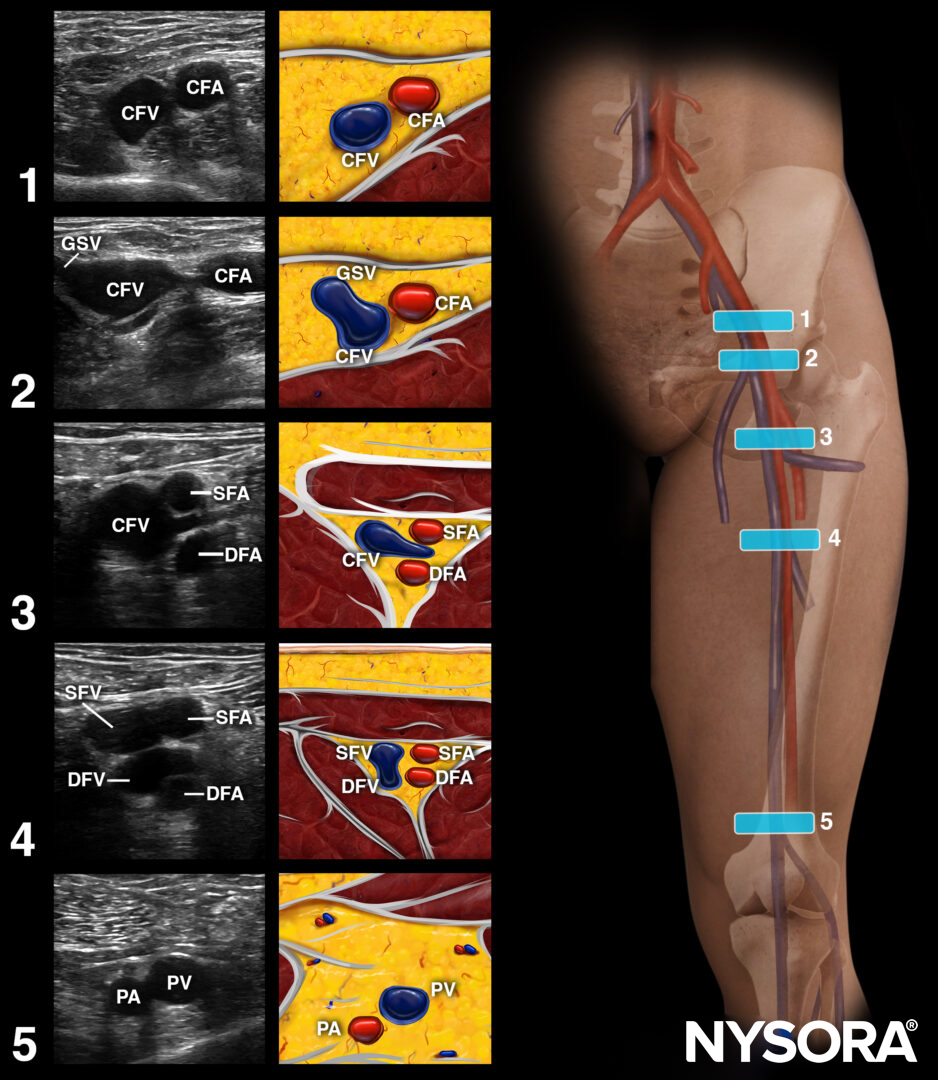
Approach for DVT scanning: Apply pressure at the following 5 points to compress the veins.
- When negative, the PLAPS point should be assessed to rule out consolidation.
PLAPS point.

Shred sign or C-line.
- In case of an A’-profile, the chest wall should be scanned to rule in a lung point.
Lung point.
Summary
The BLUE protocol. Adapted from D. Lichtenstein.
Note
The BLUE protocol has an accuracy of more than 90% for prompting diagnosis in the setting of acute respiratory failure.
Clinical updates
O’Brien et al. (International Journal of Emergency Medicine, 2025) conducted a prospective study of 250 ED patients with dyspnea and found that a fourth-year medical student performing a modified BLUE protocol POCUS achieved 84% overall diagnostic accuracy (κ=0.84), with high sensitivity/specificity for asthma/COPD (88%/96%), acute heart failure (81%/99%), pneumonia (80%/97%), and pneumothorax (100%/99%) . Mean POCUS exam time was 10.4 minutes versus 102.1 minutes to obtain CXR (p<0.0001), suggesting novice-performed POCUS can provide rapid, reliable risk stratification for common dyspnea etiologies in the ED.
- O’Brien J, Caja KR, Tabbut MP, Schrock JW. Novice point-of-care ultrasound for the assessment of acute dyspnea in the emergency department. Int J Emerg Med. 2025;18(1):204.