Indications
- Chest pain
- Dizziness
- Dyspnea or respiratory failure
- Hypotension
- Heart Murmurs
- Abnormal ECG
- Cardiac arrest
- Shock
- Volume status
Essential info
POCUS for cardiac ultrasound can be used in the acute setting to guide management, but does not equal a full diagnostic cardiac ultrasound. A POCUS examination is focused and goal-directed!
Functional anatomy
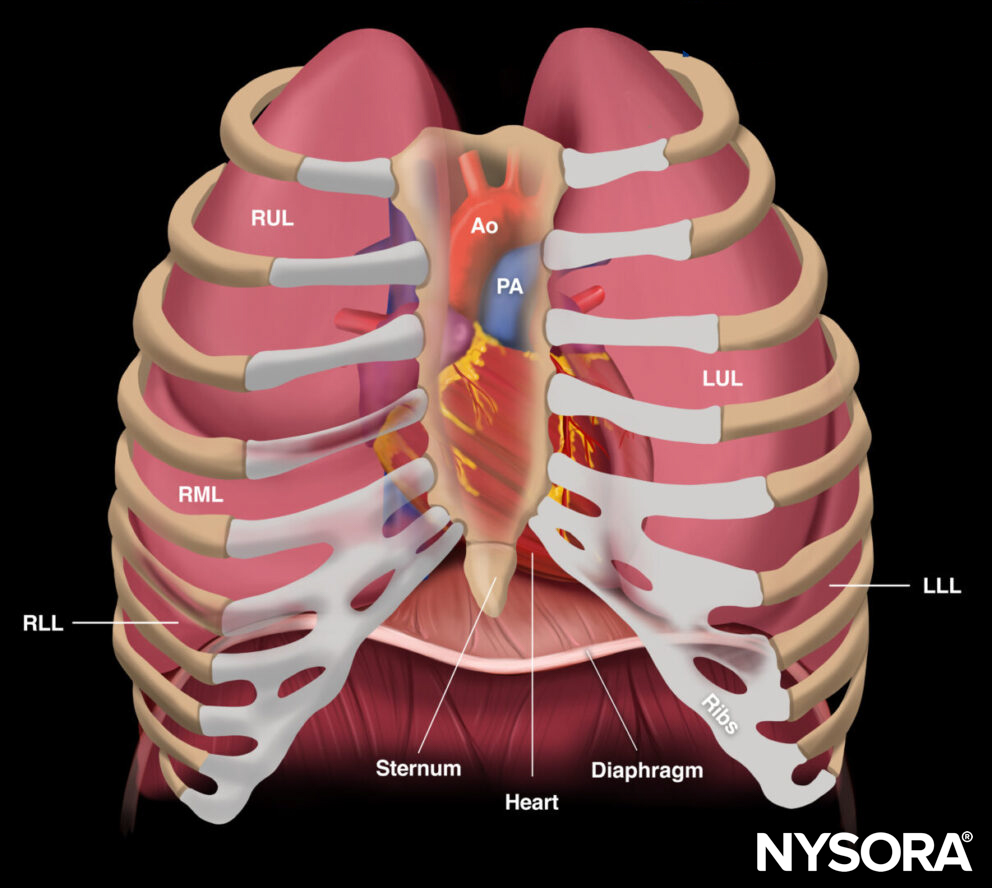
Anatomy of the thorax
The heart is located in the mediastinum between the lungs, in the center of the chest, and inside the rib cage. For that reason, cardiac ultrasound requires skills to work around the sternum and ribs to obtain adequate images through sonographic windows.

Relevant anatomy of the thorax with the different lung lobes (RUL, right upper lobe; RML, right middle lobe; RLL, right lower lobe; LUL, left upper lobe; LLL, left lower lobe), heart and large vessels (Ao, aorta; PA, pulmonary artery), diaphragm and bony structures (sternum and ribs).
Anatomy of the heart
The heart consists of four chambers (right atrium, right ventricle, left atrium, and left ventricle) and four valves (tricuspid valve, pulmonic valve, mitral valve, and aortic valve).
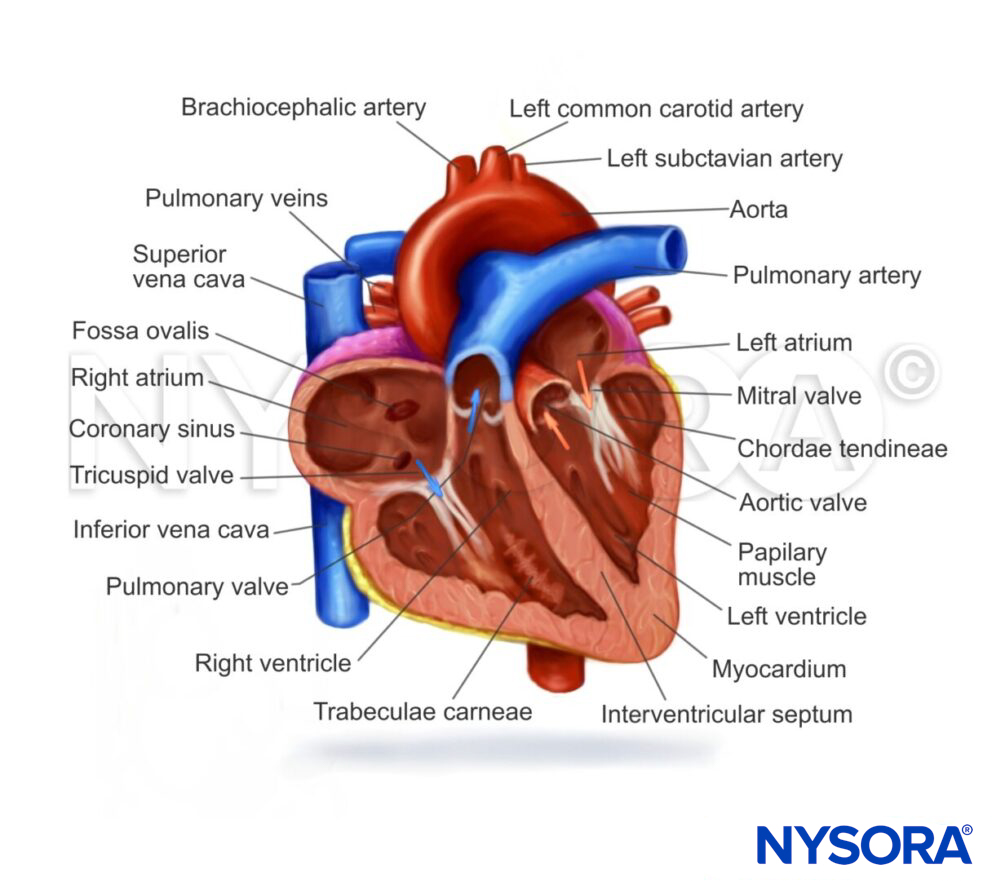
Functional anatomy of the heart and relevant structures. The blue arrows and vessels represent deoxygenated blood, while the red vessels and arrows represent blood rich in oxygen.
Ultrasound machine setup
- Transducer: Phased array transducer 1-5 MHz
- Ultrasound preset: Cardiac
- Orientation: Depends on the type of view and transducer position (cf. scanning)
- Depth: 15-20 cm
Tip
In the cardiac ultrasound preset, the screen index mark will be on the right side of the screen! In all other POCUS applications, the index mark will be on the left side of the screen.
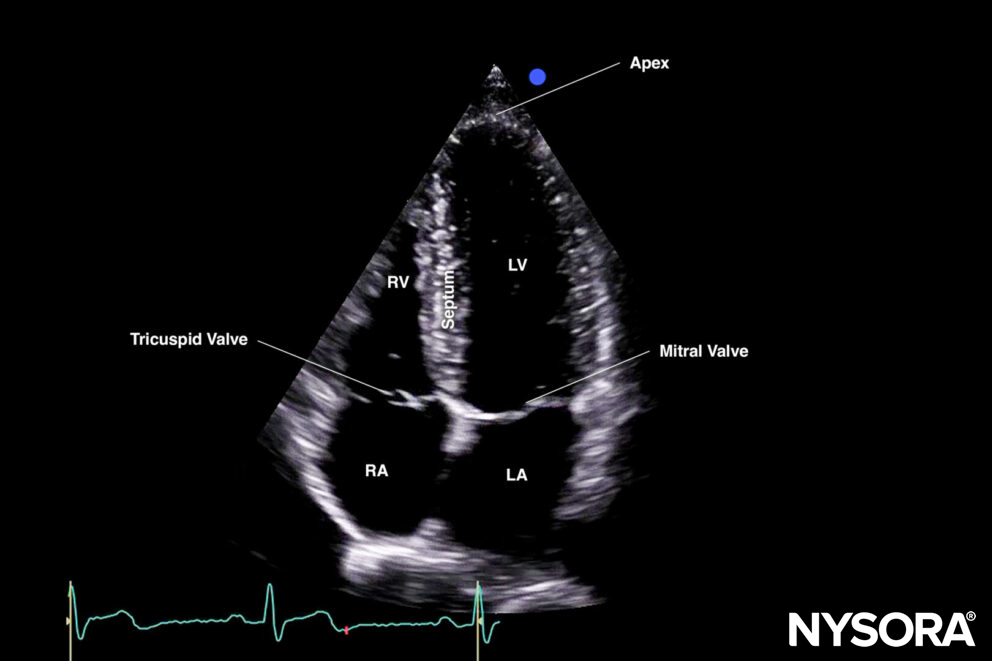
Illustration of the orientation marker on the right side of the screen when using cardiac settings. RV, right ventricle; LV, left ventricle; RA, right atrium; LA, left atrium.
Patient position
Left lateral decubitus provides better heart imaging by shifting the intrathoracic organs to the left side of the chest wall, bringing them closer to the ultrasound transducer.

The left lateral decubitus position is preferred for cardiac POCUS.
If left lateral decubitus is impossible, e.g., on critically ill or morbid patients, use the supine position and try to abduct the patient’s left arm.

Patients can also be scanned in the supine position if left lateral decubitus is not possible.
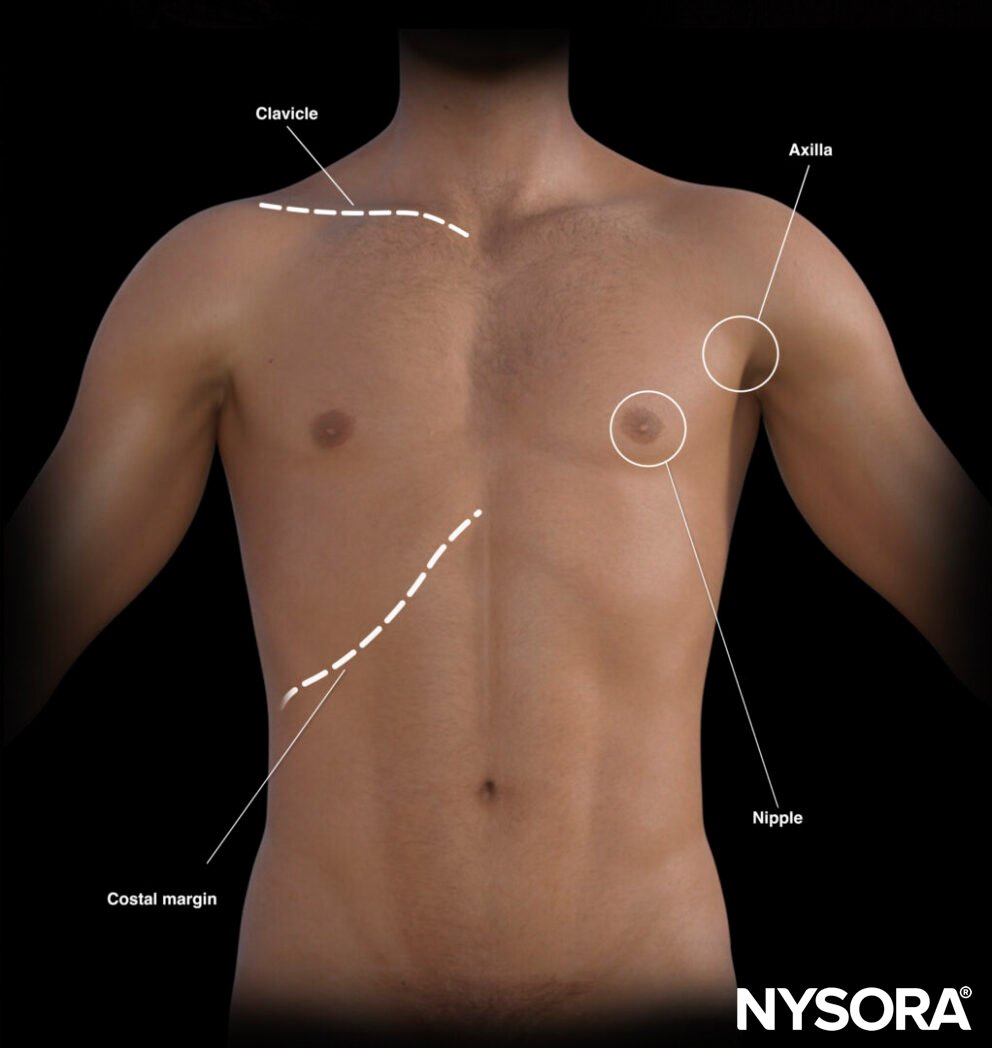
Landmarks
- Clavicles
- Sternum
- Nipple (male)/inframammary fold (female): 4th intercostal space
- Costal margin
The left lateral decubitus position is preferred for cardiac POCUS.
Transducer position
A cardiac ultrasound is performed in three areas:
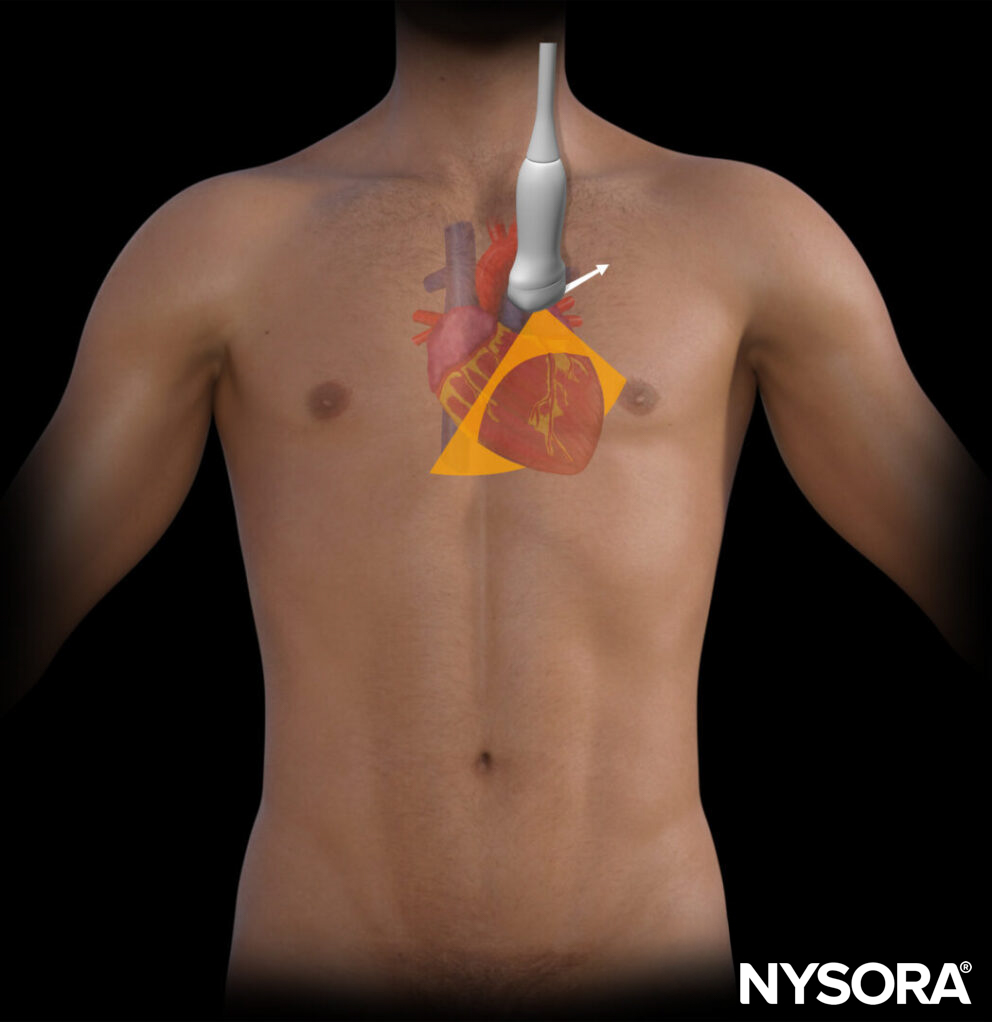
- Parasternal: 2nd to 4th rib intercostal space, left of the sternum.
- 2: Apical: 5th rib intercostal space, under left nipple, point of maximal impulse of the heart.
- 3: Subcostal: Overhand grip and transducer almost parallel with the skin.
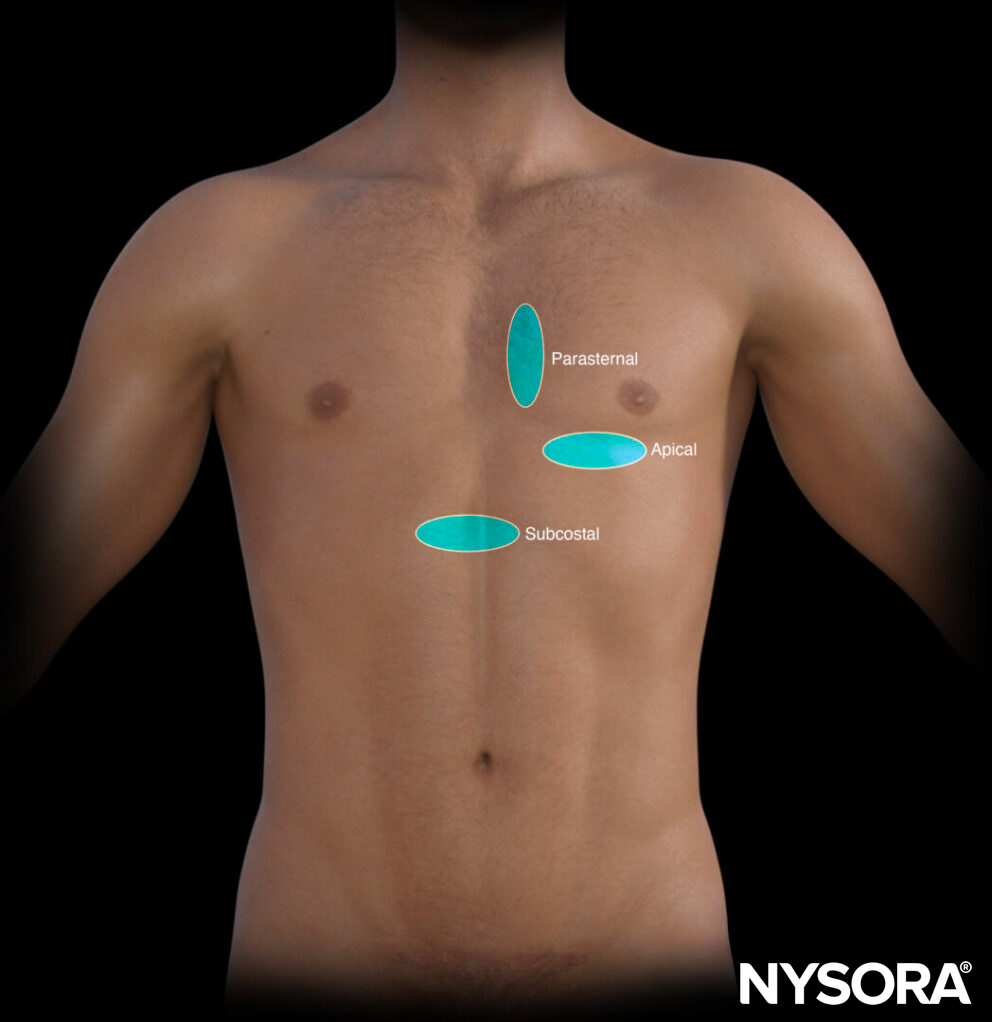
Different areas for transducer positioning in cardiac ultrasound: Parasternal, apical, and subcostal.
Scanning
Keep in mind that the heart has a diagonal/oblique axis. Each specific position (parasternal, apical, subcostal) and specific orientation images different structures of the heart by cutting the heart into one of the 3 planes:
- Long axis: Sagittal plane
- Short axis: Transverse plane
Four-chamber: Coronal plane
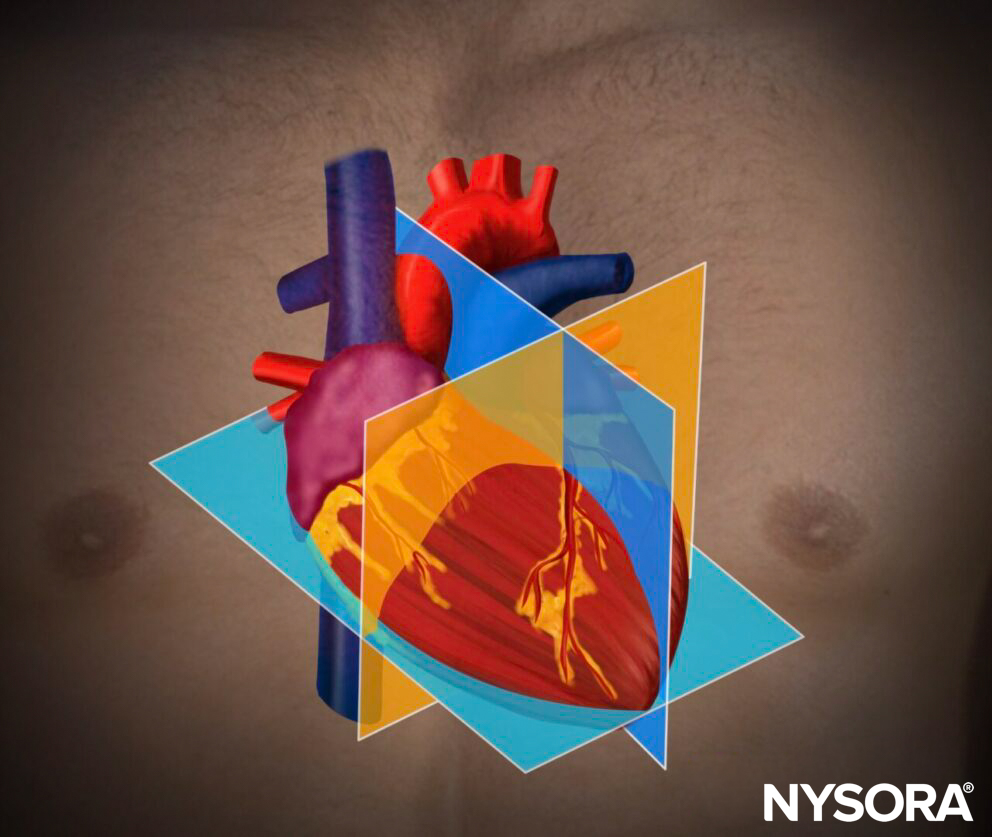
Traditional planes for cardiac ultrasound. The white dots represent the 3 transducer positions (parasternal, apical, and subcostal).
To obtain these planes with ultrasound, the index mark is oriented differently in each of the 3 positions. Each orientation at a specific position is designated by a standard nomenclature. For example, scanning in the parasternal position with a short-axis orientation is called ‘parasternal short axis view’.
Five essential cardiac ultrasound views: PLAX, parasternal long-axis view; PSAX, parasternal short-axis view; A4C, apical four-chamber view; S4C, subcostal four-chamber view; IVC, inferior vena cava view.
In total, scanning at these three positions with five different orientations will result in five essential cardiac ultrasound views:
- Parasternal long-axis view
- Parasternal short-axis view
- Apical four-chamber view
- Subcostal four-chamber view
- Inferior vena cava view
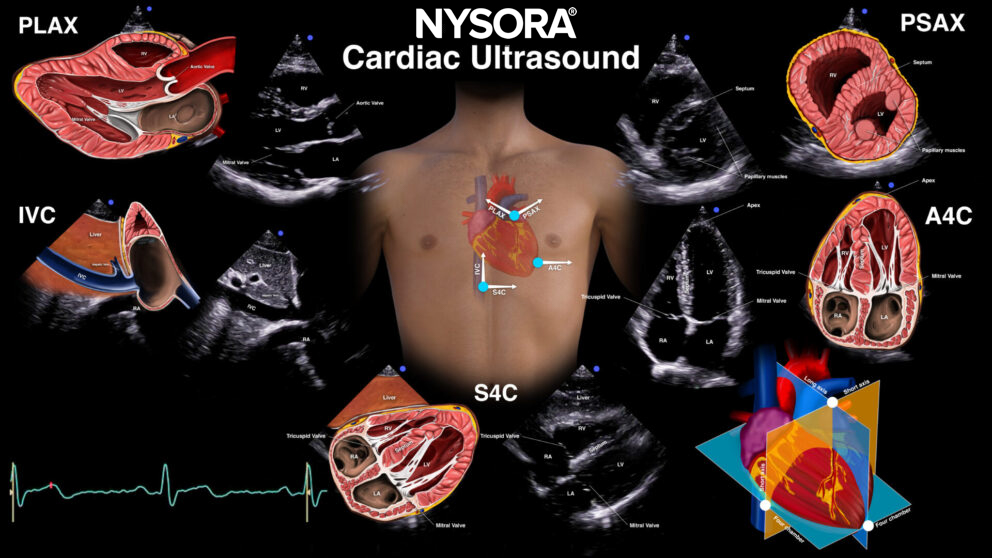
Different views according to the 3 transducer positions and 5 orientations for cardiac ultrasound. Parasternal long axis (PSAX), parasternal short axis (PSAX), apical 4-chamber (A4C), subcostal 4-chamber (S4C), inferior vena cava (IVC).
Tips
- Hold the transducer like a stencil and stabilize the hypothenar of your hand on the patient’s chest.
- For cardiac ultrasound, transducer movements are subtle but crucially important to obtain adequate views through the sonographic windows created by the sternum and the ribs:
- Sliding: Transducer alignments to find a window.
- Tilting: To the tilt transducer to planes perpendicular to the index mark.
- Rotation: Clockwise or counter-clockwise rotation.
- Rocking (heeling): Pivoting the transducer to planes parallel to the index mark.
Transducer maneuvers to optimize image quality.
Tip
Off-axis scanning frequently occurs in cardiac ultrasound and can lead to misinterpretations of diameter and size.
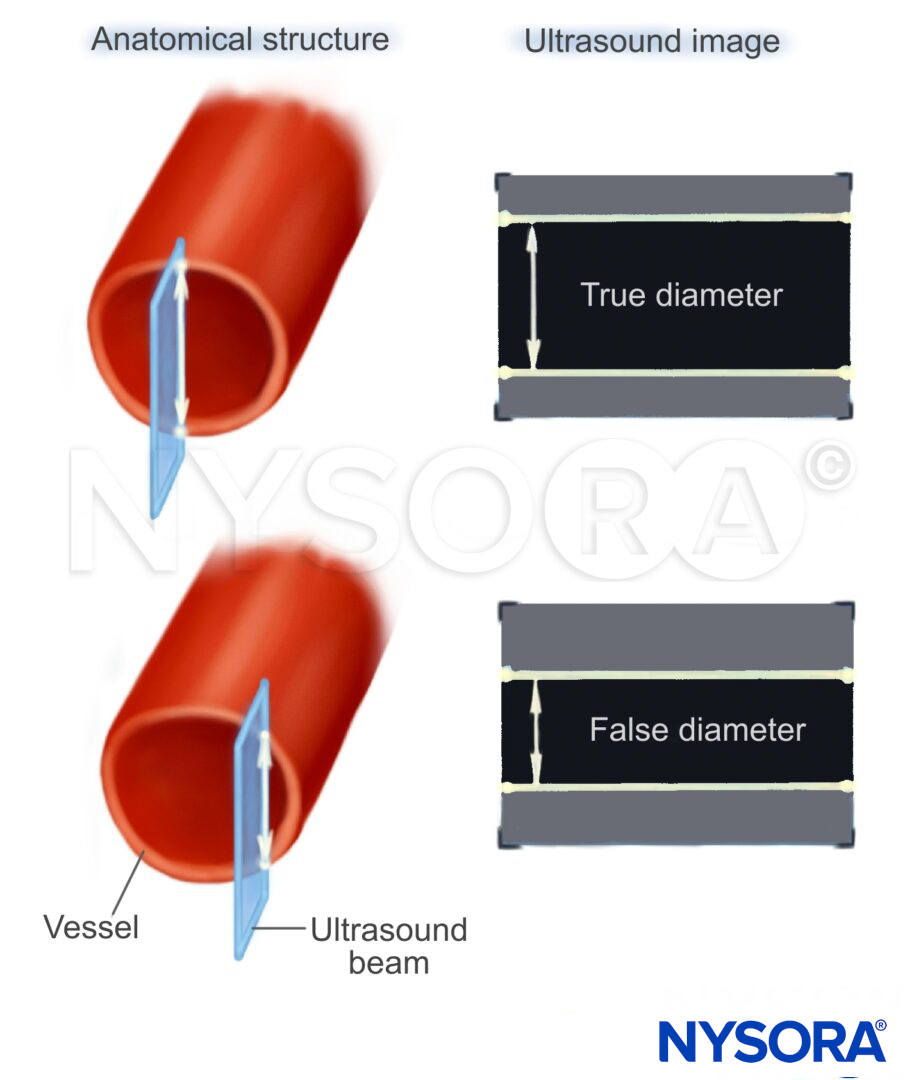
Illustration of how off-axis scanning can lead to false interpretations.
Tips
- Cardiac ultrasound assessment requires a systematic approach in all positions and orientations.
- Always optimize the depth settings to see all structures.
- When a good acoustic window is obtained, try to maximize the information, as other acoustic sono windows may not be favorable.
- If it is difficult to obtain an image, change the body position if possible.
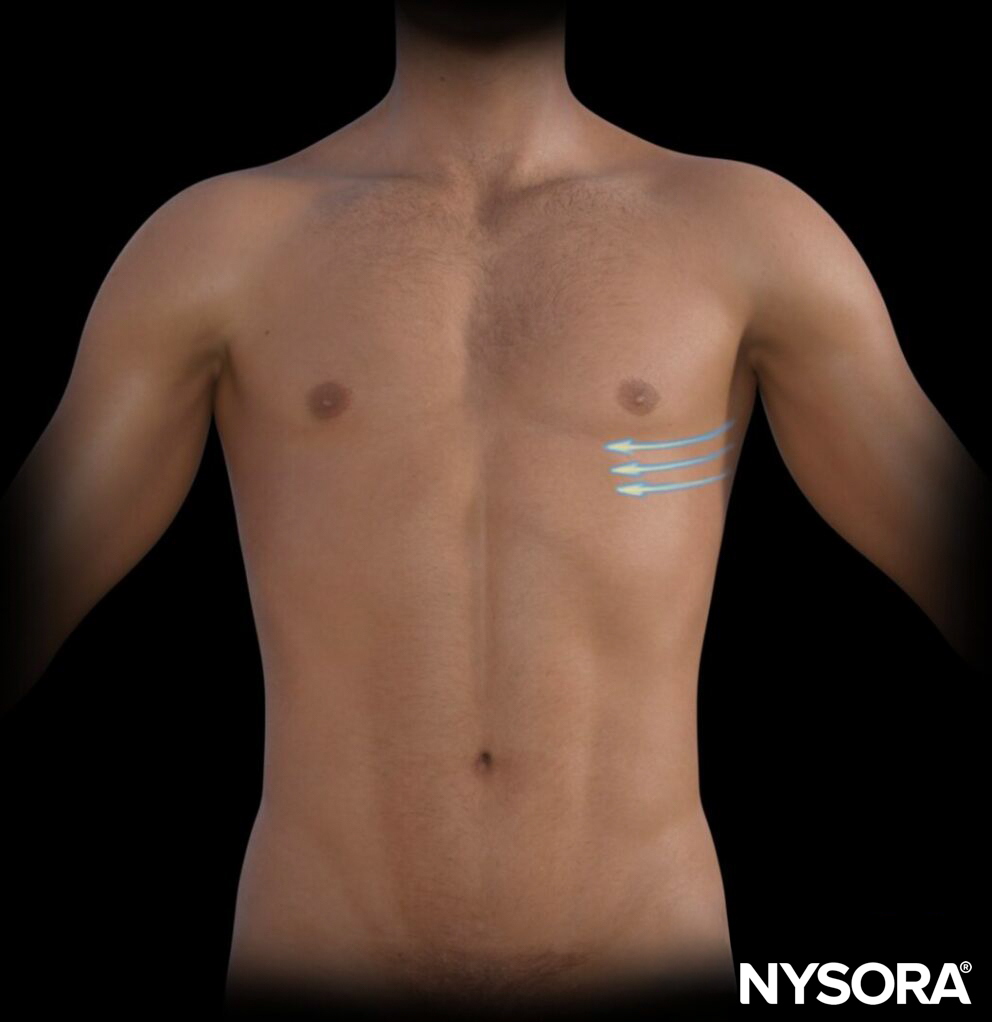
- Movements to find acoustic windows:
- Parasternal: Snail shell movement around the starting point.

Snail shell movements to find acoustic windows in the parasternal views.
- Apical 4-chamber: Between rib spaces moving from midaxillary to midclavicular in C-shapes.
C-chape movements between rib spaces, moving from midaxillary to midclavicular in the apical 4-chamber view.
- Subcostal: All structures are located close to each other and deeper, so small movements are required.
Parasternal long-axis view (PLAX)
Positioning
Place the transducer at the parasternal position (2nd-4th ribs) and orient the index mark toward the right shoulder.
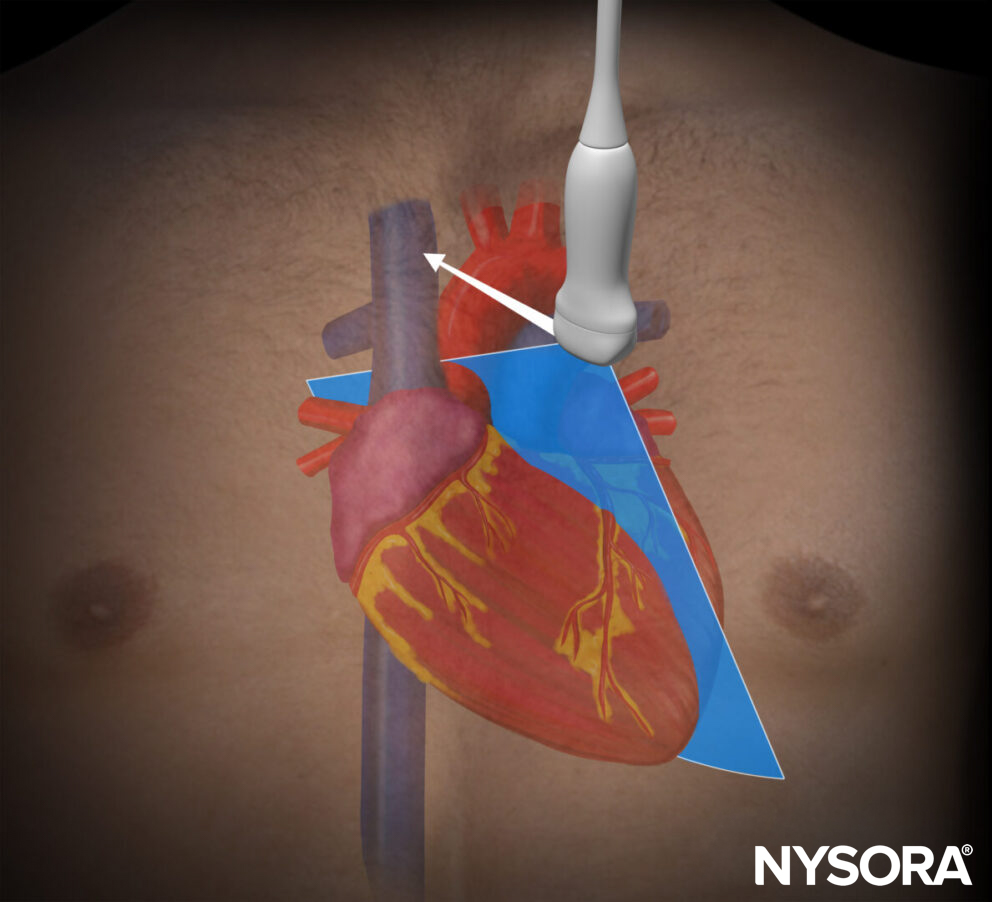
Transducer position for the parasternal long-axis view.
Sonoanatomy
The standard parasternal long-axis view cuts the heart through the sagittal plane.
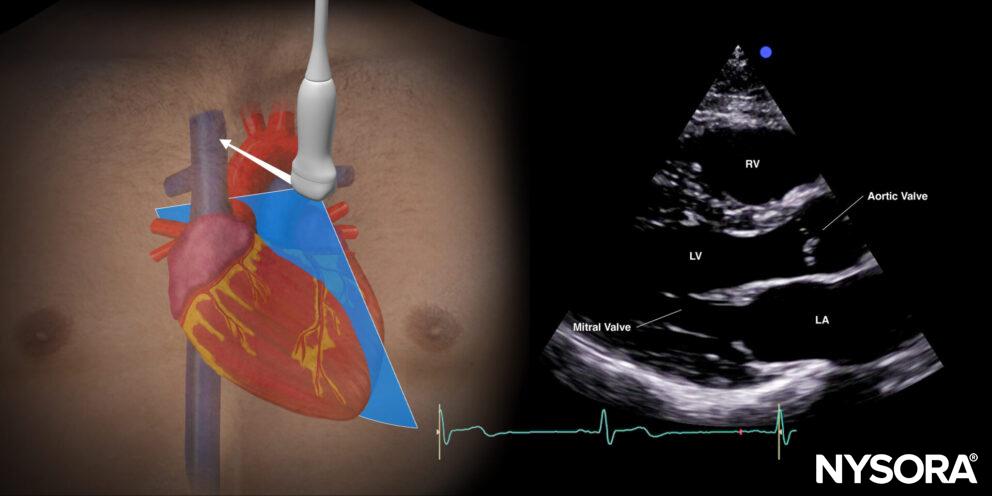
Sonoanatomy of the heart in the parasternal long-axis view. Left ventricle (LV), left atrium (LA), mitral valve, aortic valve, right ventricle (RV).
Reverse ultrasound anatomy
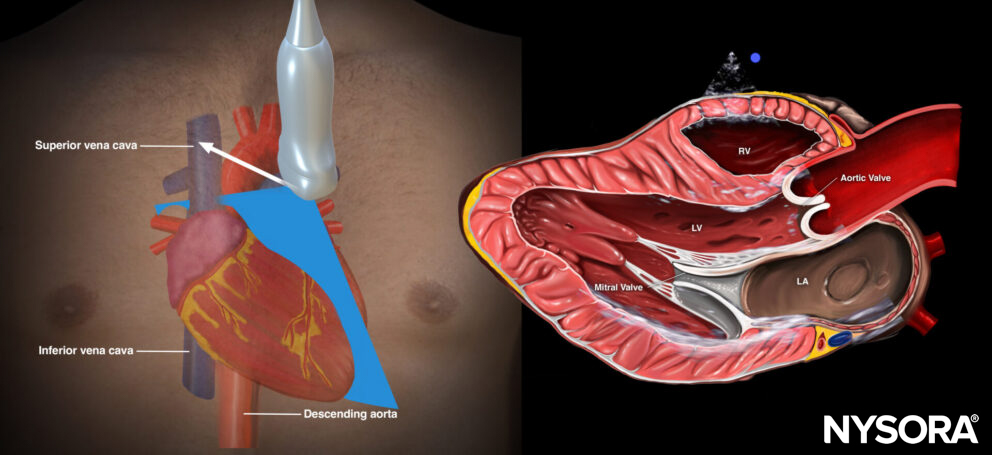
Reverse Ultrasound Anatomy of the heart in the parasternal short-axis view. Left ventricle (LV), left atrium (LA), mitral valve, aortic valve, right ventricle (RV).
Practical use:
- Left ventricle size and function
- Pericardial effusion
- Valve function: mitral valve prolapse, mitral valve regurgitation, aortic stenosis
Tips
- The parasternal long-axis view does not fully visualize the right ventricle, but mainly the right ventricular outflow tract
- This view does not include the apex of the left ventricle.
- Mnemonic that helps with the orientation of the ultrasound image: ‘3 L’s’: Long axis, Left ventricle on the Left side.
Parasternal short-axis view (PSAX)
Positioning
Place the transducer at the parasternal position (2nd-4th ribs) and orient the index mark toward the left shoulder (90 degrees clockwise from parasternal long axis view).
Transducer position for the parasternal short-axis view.
Sonoanatomy
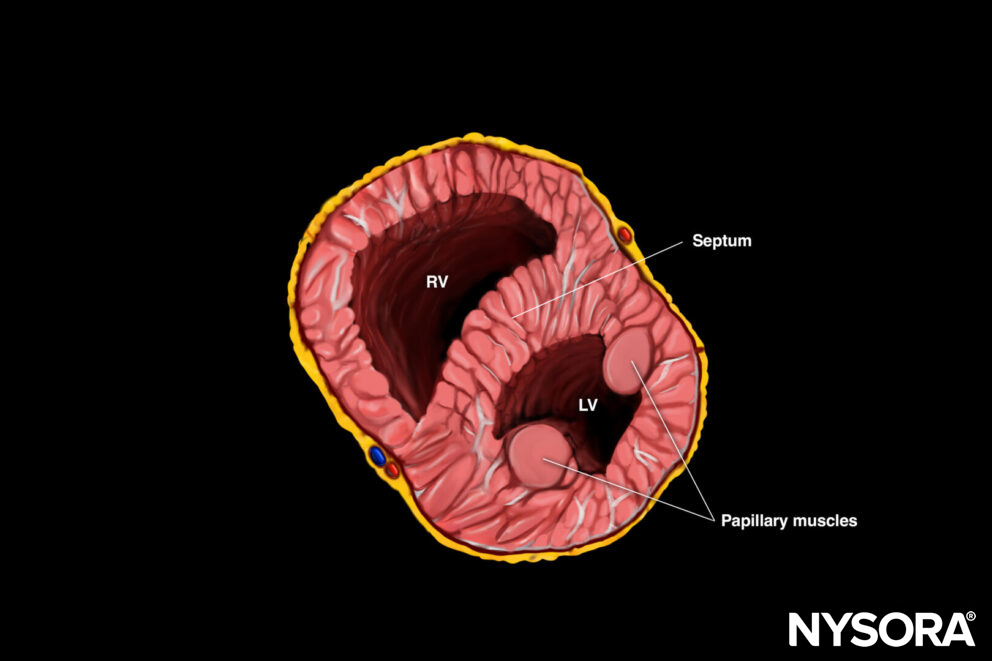
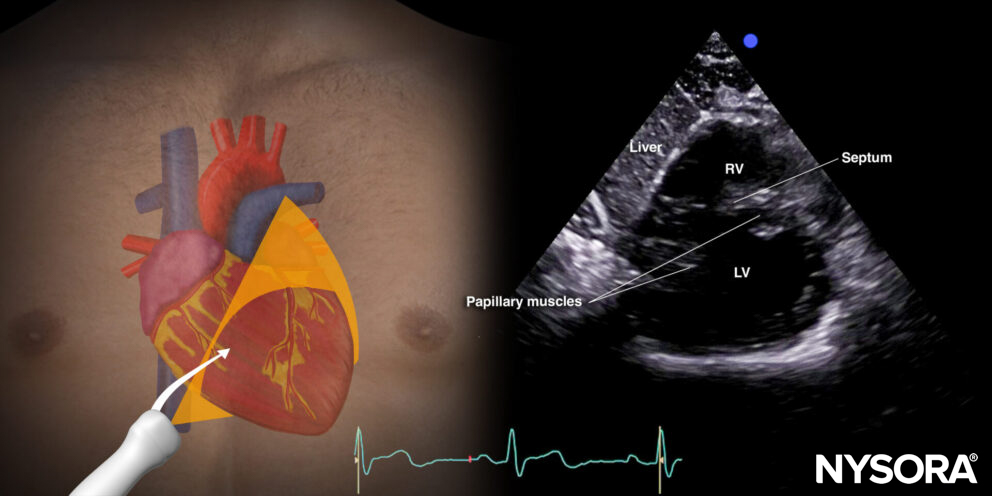
The standard parasternal short-axis view cuts the heart through the transverse plane.
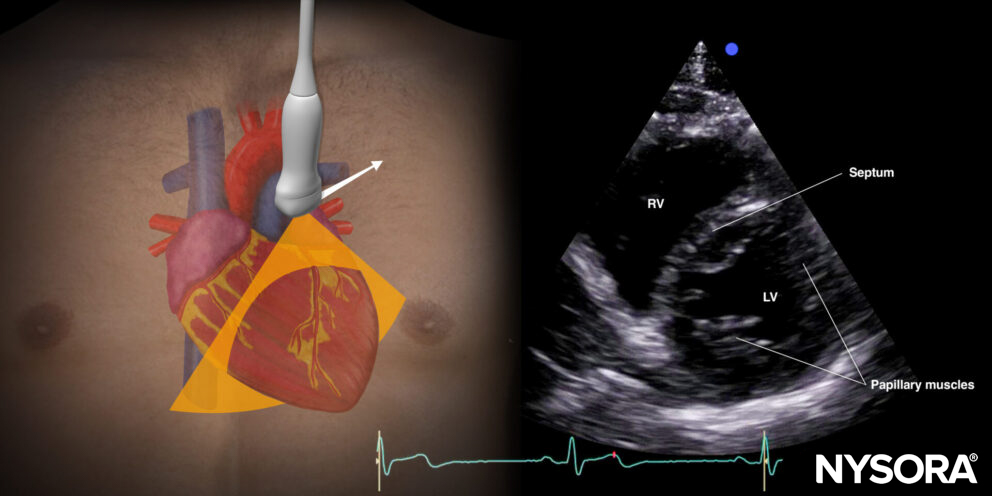
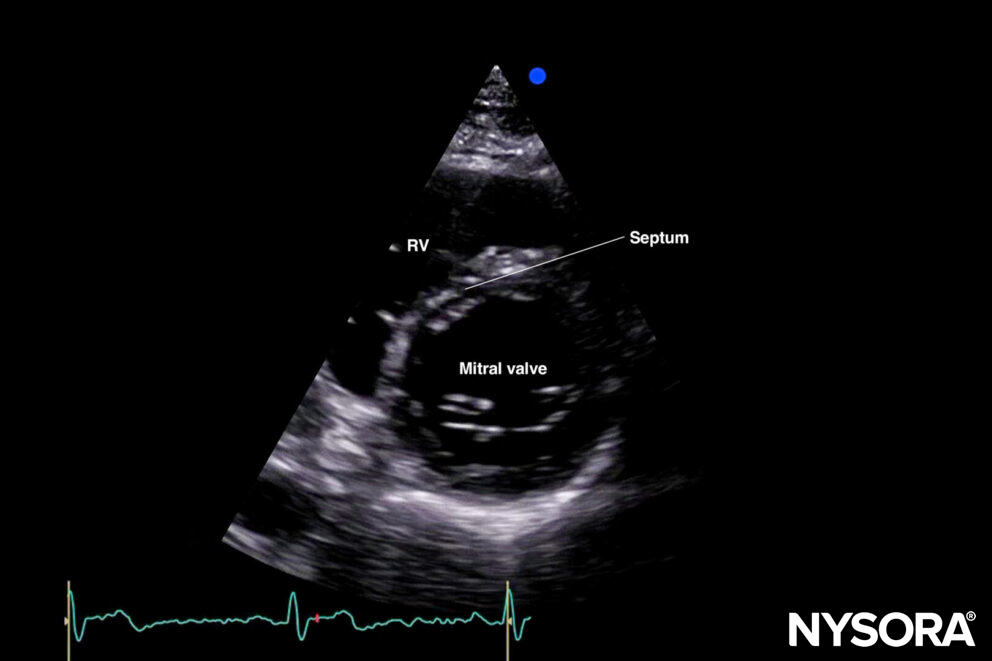
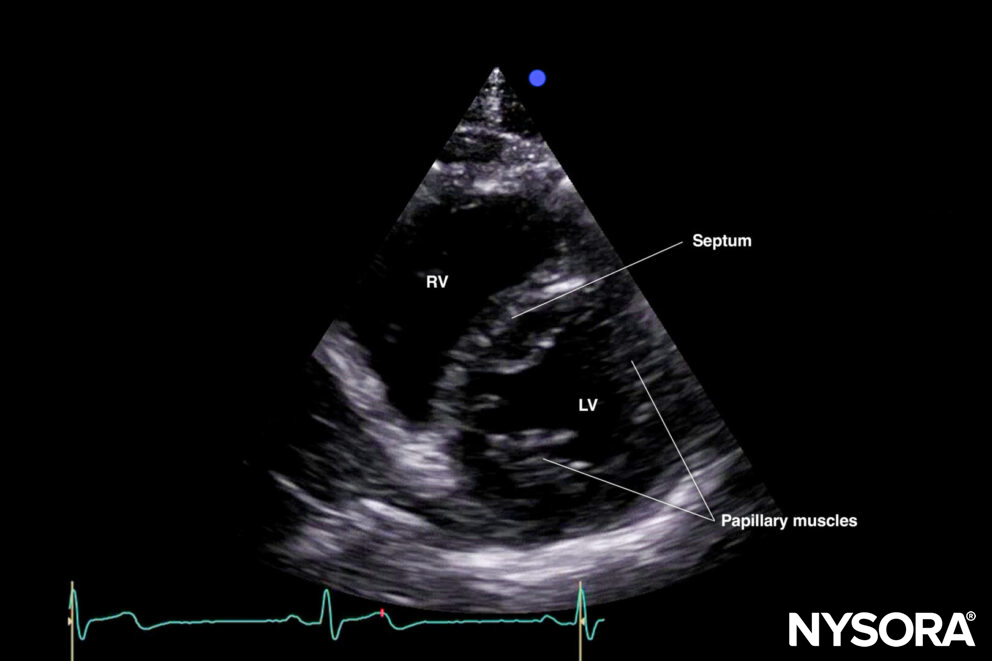
Sonoanatomy of the heart in the parasternal short-axis view. Right ventricle (RV), septum, left ventricle (LV), and papillary muscles.
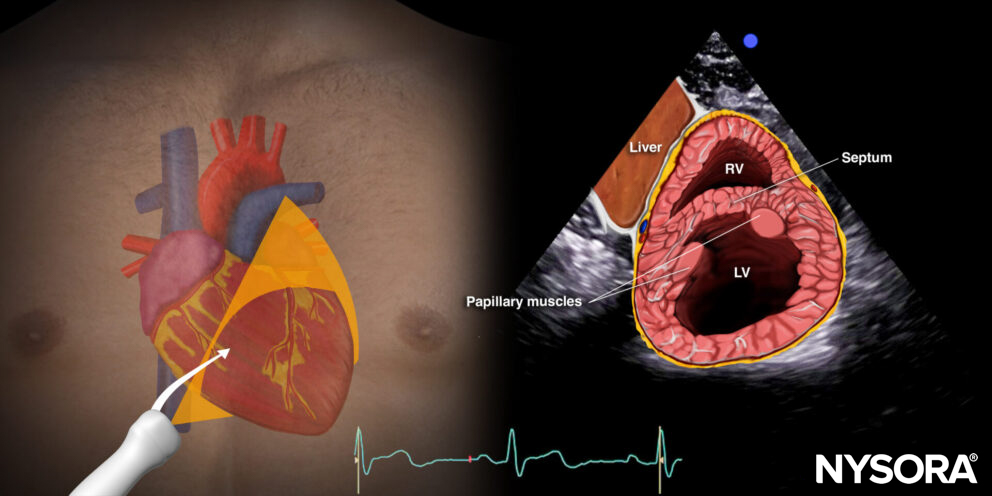
Reverse ultrasound anatomy:
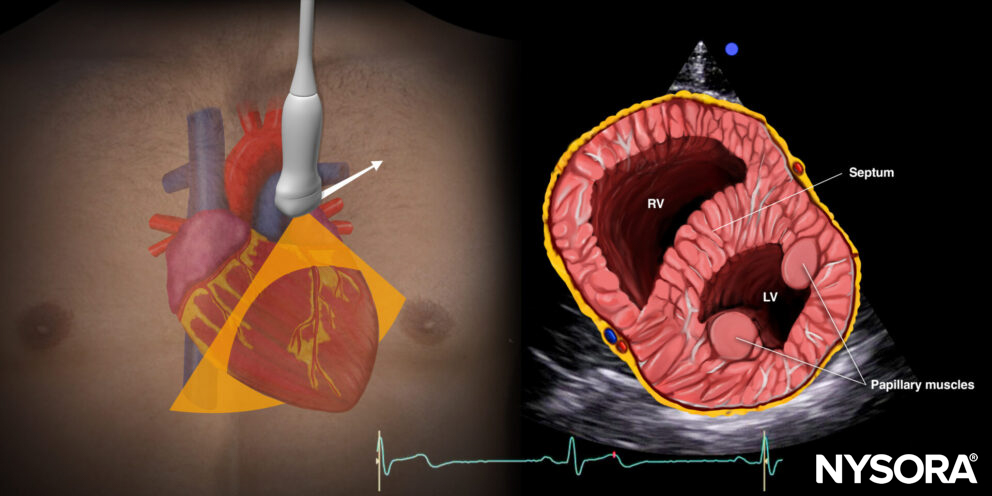
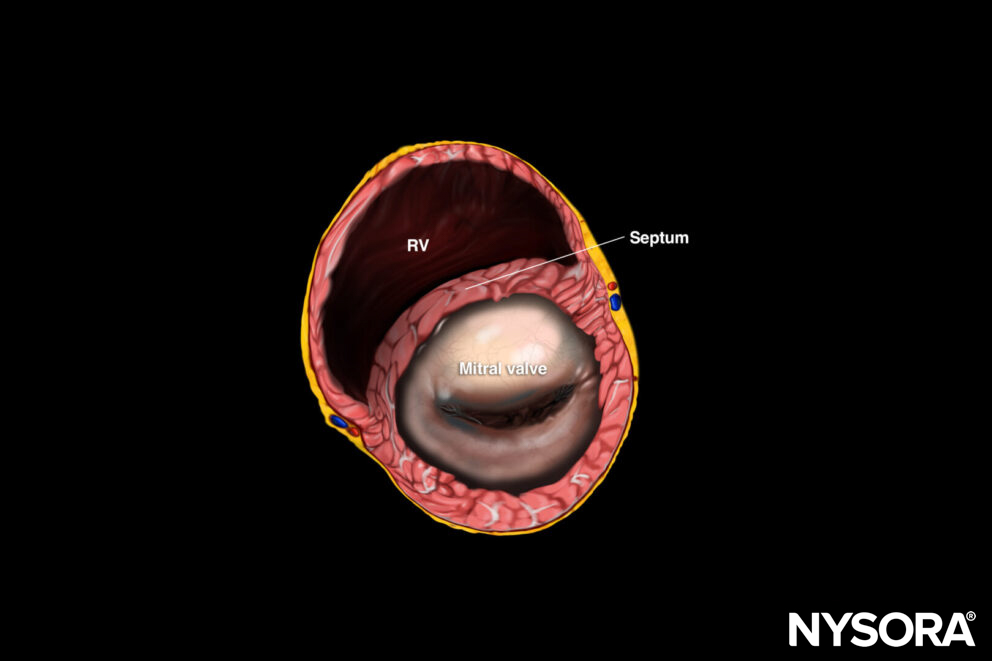
Reverse Ultrasound Anatomy of the heart in the parasternal short-axis view. Right ventricle (RV), septum, left ventricle (LV), and papillary muscles.
By tilting or sliding the transducer along the axis of the heart, other structures can be visualized next to the standard parasternal short-axis view. So in total, four levels of scanning can be obtained by tilting or sliding the transducer:
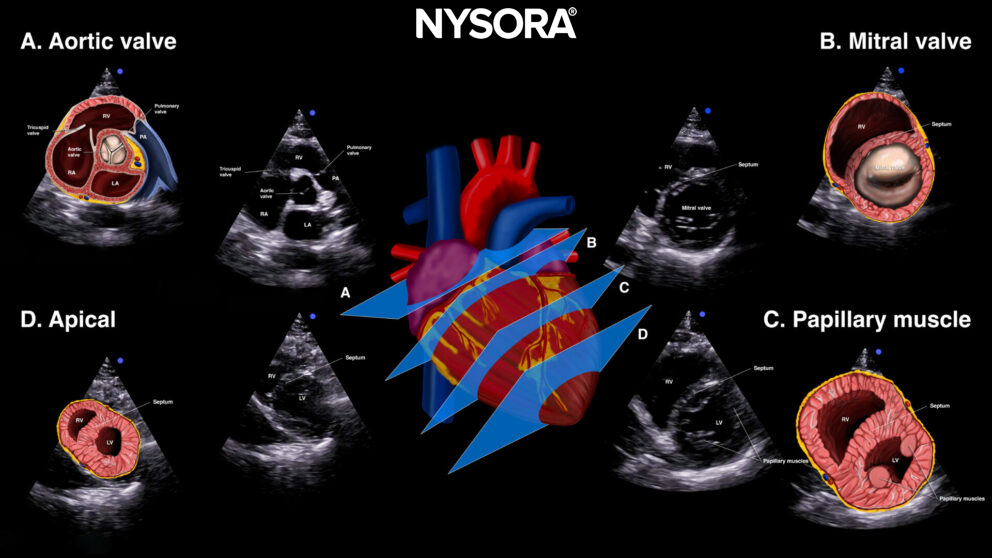
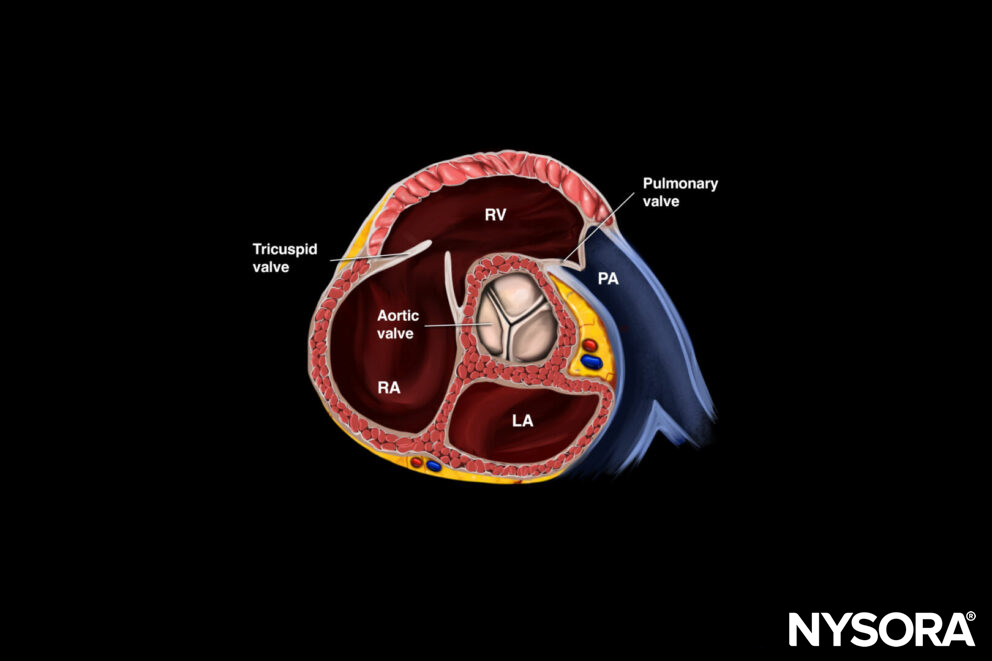
Tilting or sliding in the parasternal short-axis position provides 4 images: A. Aortic valve level (Mercedes-Benz view), B. Mitral valve level (fish mouth view), C. Papillary muscle level, D. Apical level.
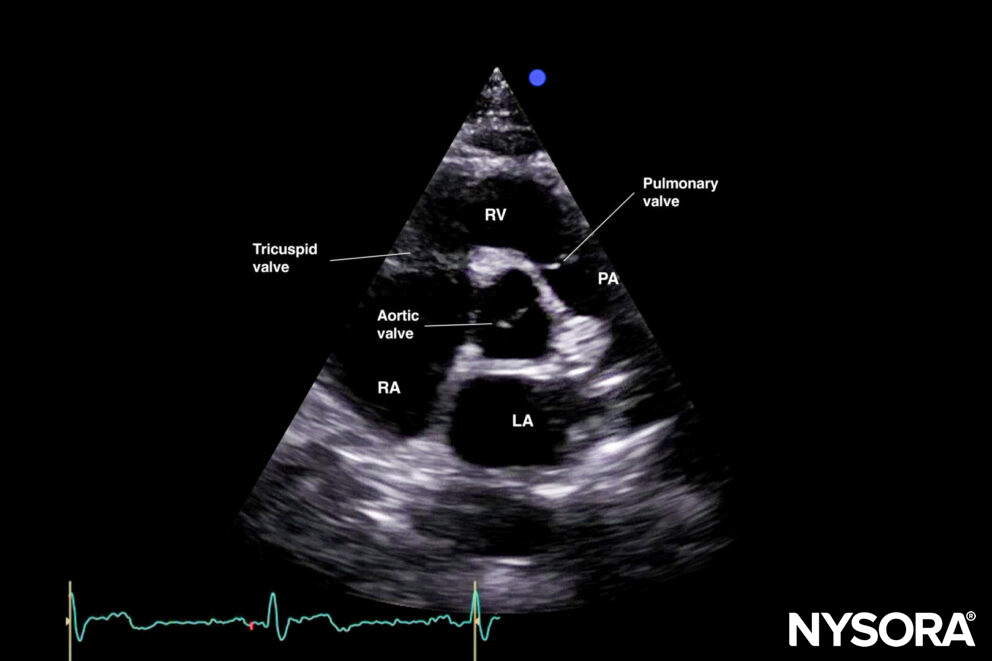
A. Aortic valve level: ‘Mercedes Benz’ view: This is a good view to assess the aortic valve, the right ventricle, the tricuspid valve, and the pulmonary valve.
Tilting or sliding in the parasternal short-axis position provides 4 images: A. Aortic valve level (Mercedes-Benz view), B. Mitral valve level (fish mouth view), C. Papillary muscle level, D. Apical level.
B. Mitral valve level: ‘Fish mouth’ view: Right ventricle and mitral valve.
C. Papillary muscle level or standard parasternal short-axis view: Right ventricle, left ventricle, papillary muscles (posteromedial and anterolateral papillary muscle).
D. Apical level: Here, the papillary muscles are gon,e and it is possible to assess the apex.
Practical use:
- Left ventricular function
- Right ventricle dilatation: a D-shaped right ventricle represents pressure and volume overload (See “Clinical applications)
- Pericardial effusion
- Valve function:
- Aortic valve: ‘Mercedes Benz’ view
- Mitral valve: ‘Fish mouth’ view: anterior and posterior leaflet
- Volume status: kissing left ventricle papillary muscles at the end of the systole indicate hypovolemia
Tips
- The papillary muscles are a landmark for dividing the left ventricle in half.
- A good parasternal long-axis view guarantees a good parasternal short-axis view.
- The left ventricle should be circular (off-axis views will result in an elliptical shape)
ALTERNATIVE VIEW FOR THE PSAX:
Subcostal short-axis view (SSAX)
Positioning:
Place the transducer with an overhand grip at the subcostal position and the index marker toward the patient’s left shoulder.
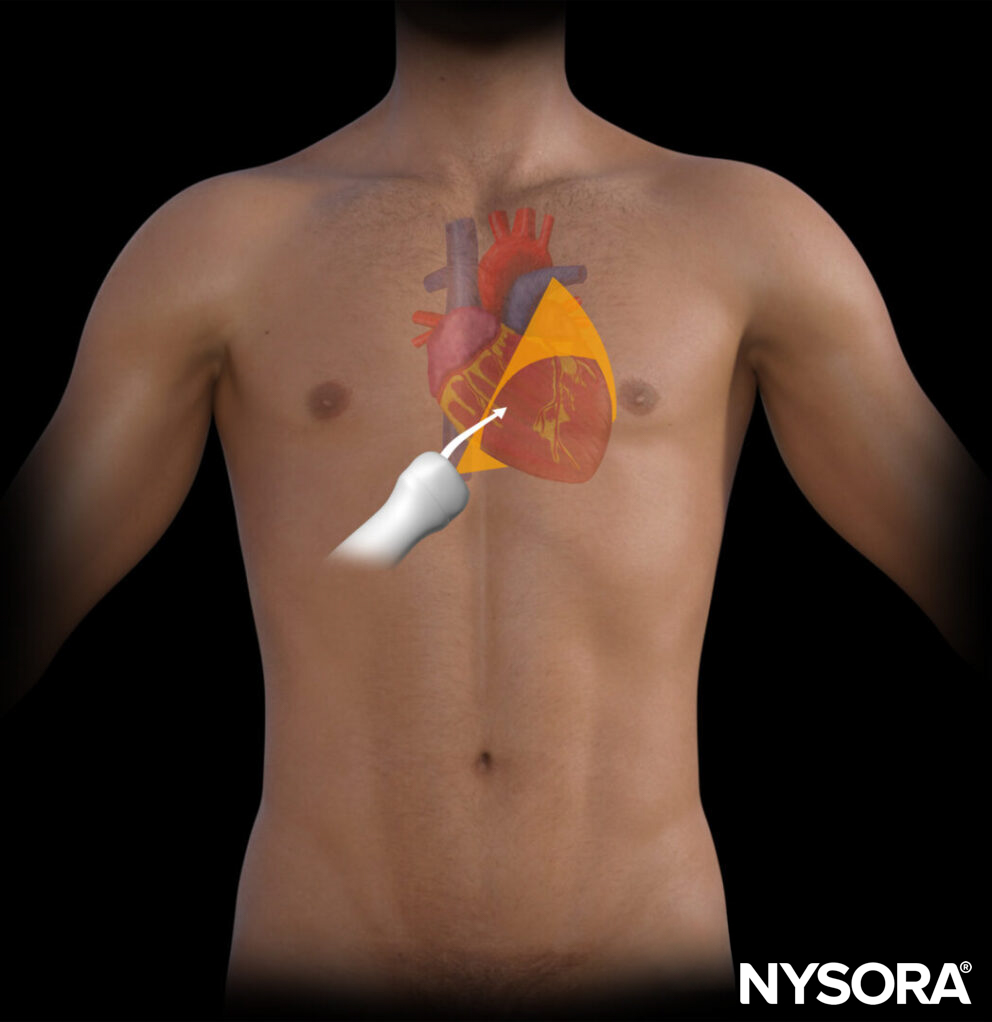
Transducer position for the subcostal short-axis view.
Sonoanatomy:
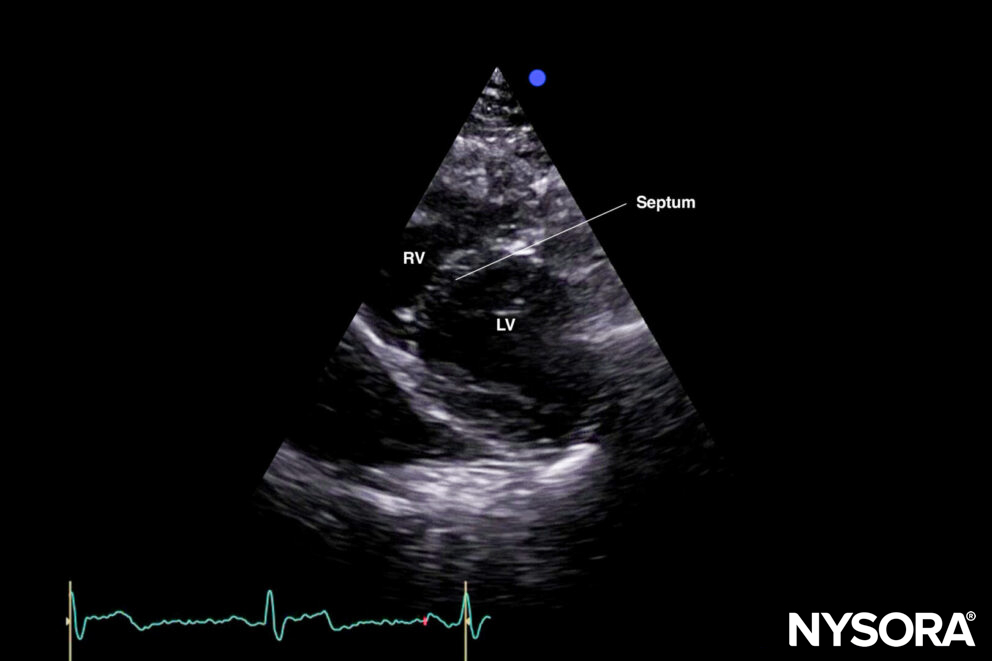
The subcostal short-axis view cuts the heart through the same transverse plane, but at a lower angle.
Sonoanatomy of the heart in the subcostal short-axis view. Right ventricle (RV), left ventricle (LV), septum, and papillary muscles.
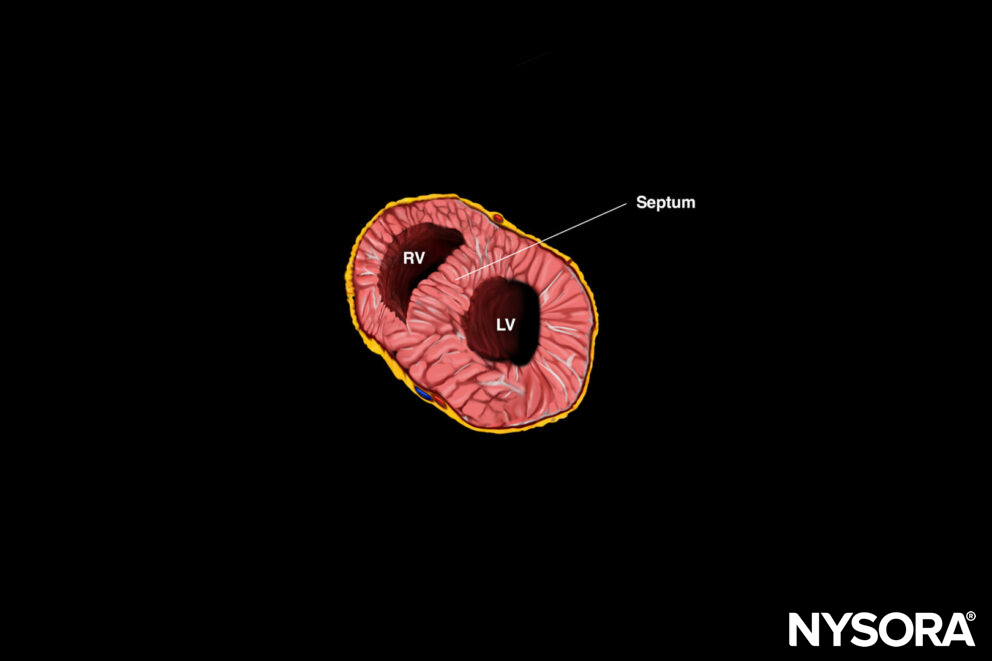
Reverse ultrasound anatomy:
Reverse Ultrasound Anatomy of the heart in the subcostal short-axis view. Right ventricle (RV), left ventricle (LV), septum, and papillary muscles.
Practical use:
The information that can be obtained with the SSAX view is the same as for the PSAX:
- Left ventricular function
- Right ventricle dilatation: a D-shaped right ventricle represents pressure and volume overload
- Pericardial effusion
- Valve function:
- Aortic valve: ‘Mercedes Benz’ view
- Mitral valve: ‘Fish mouth’ view: anterior and posterior leaflet
- Volume status: kissing left ventricle papillary muscles at the end of the systole indicate hypovolemia
Tips
- Tilting or sliding the transducer along the axis of the heart will provide the same views as the PSAX (aortic valve, mitral valve, papillary muscle, and apical view)
- Specific populations, such as ventilated patients with high PEEP or COPD patients, can have a hard parasternal short-axis view due to hyperinflation of the lungs. The subcostal short-axis view is a good alternative here since the heart usually shifts caudally due to high intrathoracic pressures.
- The subcostal view may be challenging in obese or muscular patients due to the abdominal mass.
Apical four-chamber view (A4C)
Positioning:
Place the transducer at the apical position (5th-6th ribs) and with the index marker toward the left side of the patient.
Tip
The apical position is usually at the point where the pulse of the heart can be felt the best (point of maximal impulse).
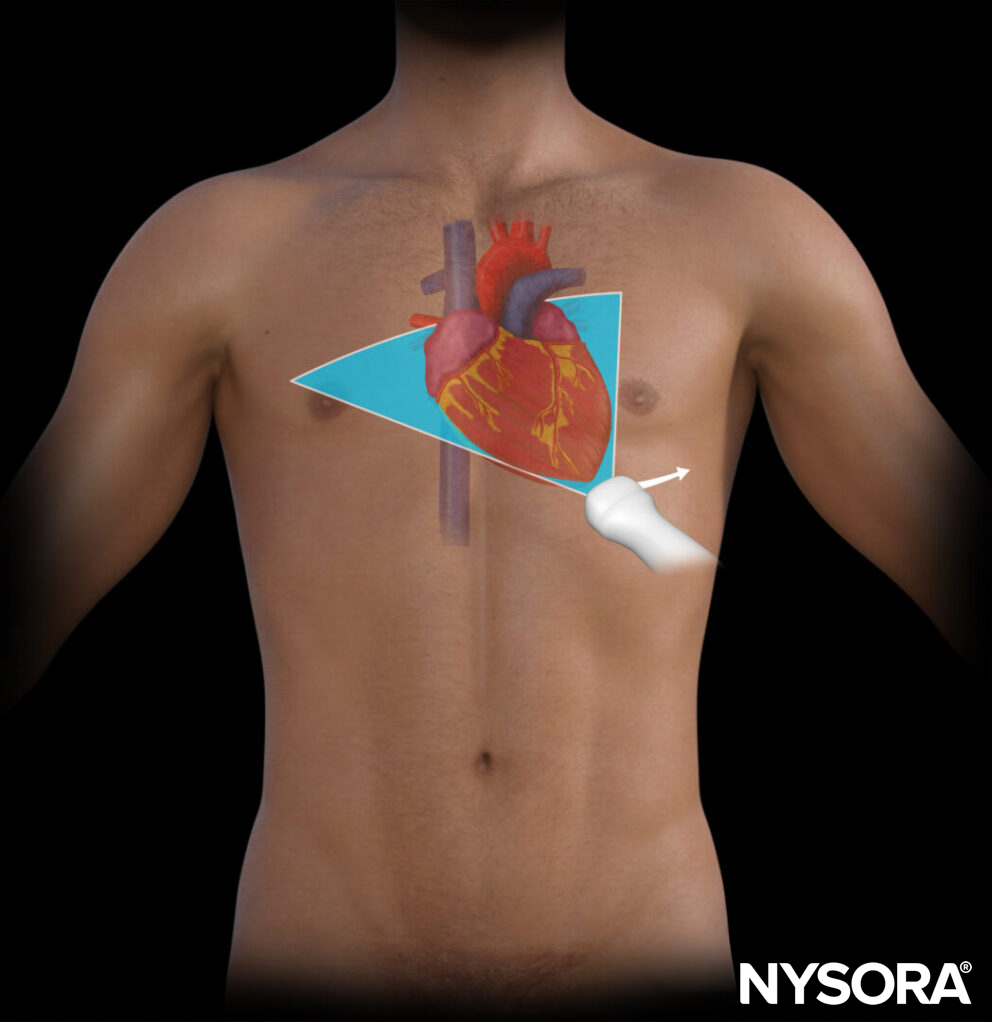
Transducer position for the apical four-chamber view.
Sonoanatomy
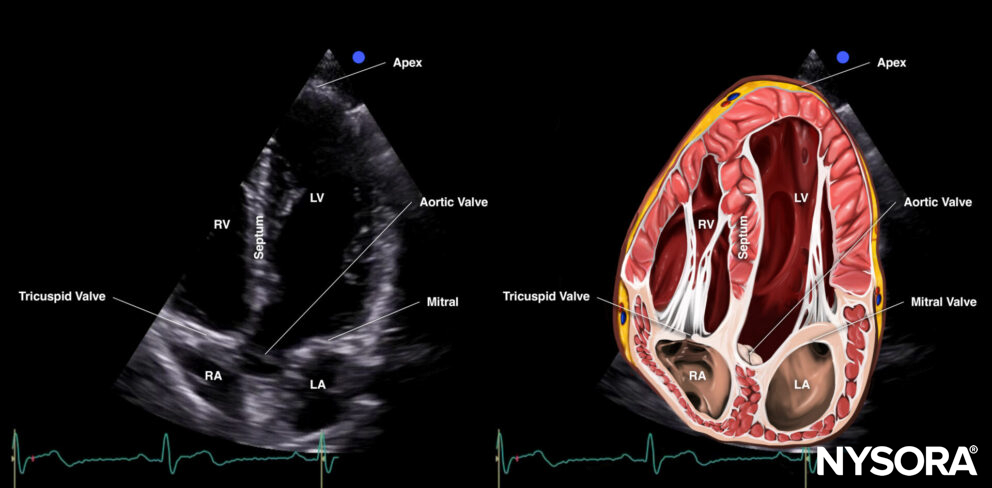
The apical four-chamber view cuts the heart through the coronal plane.
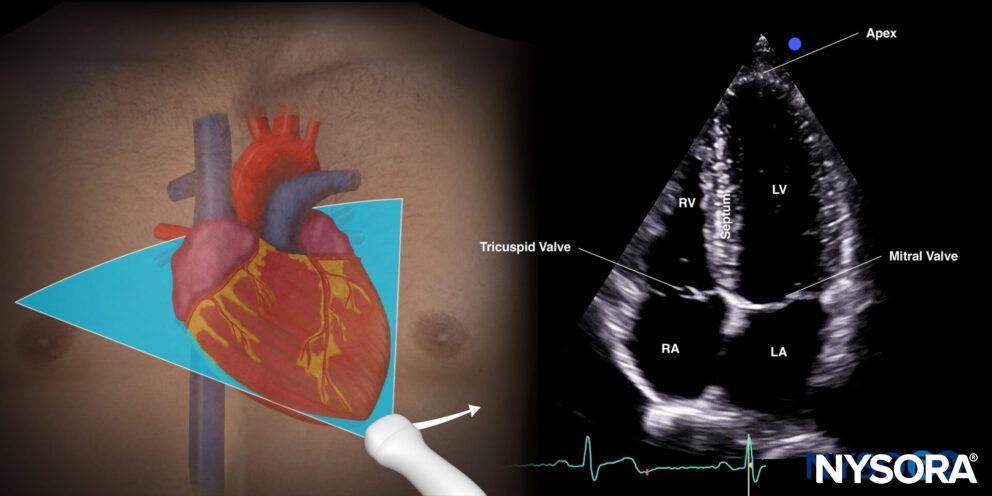
Sonoanatomy of the heart in the apical four-chamber view. Left atrium (LA), left ventricle (LV), right atrium (RA), right ventricle (RV), septum, tricuspid valve, mitral valve, apex.
Reverse ultrasound anatomy:
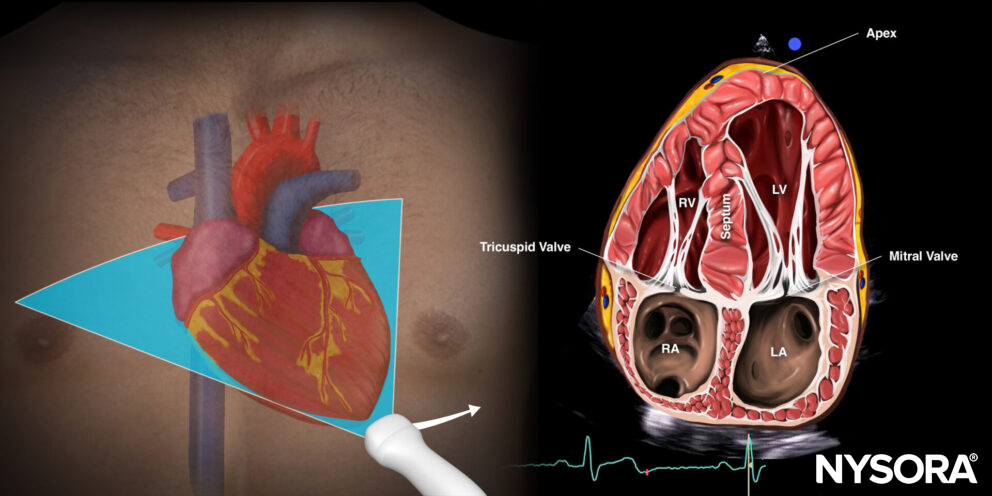
Reverse Ultrasound Anatomy of the heart in the apical four-chamber view. Left atrium (LA), left ventricle (LV), right atrium (RA), right ventricle (RV), septum, tricuspid valve, mitral valve, apex.
Practical use:
- Left ventricle size and function
- Right ventricle size and function
- Septal kinetics
- Valve function: Doppler
Tips
- The apical 4-chamber view can be challenging to obtain. Repositioning the patient into left lateral decubitus brings the heart closer to the chest wall, potentially improving imaging by reducing lung artifacts.
- Adjust the depth to visualize all 4 chambers.
- Off-axis scanning is very common and is also called foreshortening. This will result in inaccurate measurements. If the ventricles look rounded and shorter instead of bullet-shaped, the cursor should be moved more apically and more laterally. To prevent foreshortening, the septum should always point toward the top of the screen, and the left ventricle needs to be assessed in its longest axis.
- The apical 4-chamber views can be modified to image other structures of interest:
- Apical 5-chamber view: Tilting transducer 5-10 degrees caudally to the apical 4-chamber view. This will result in the visualization of the so-called 5th chamber, or the left ventricle outflow tract.
Apical 5-chamber view (left) and Reverse Ultrasound Anatomy (right).
-
- Coronary sinus view: Tilting the transducer 5-10 degrees cranially to the apical 4-chamber view. The coronary sinus will appear as an atrial septal defect between the right and left atrium.
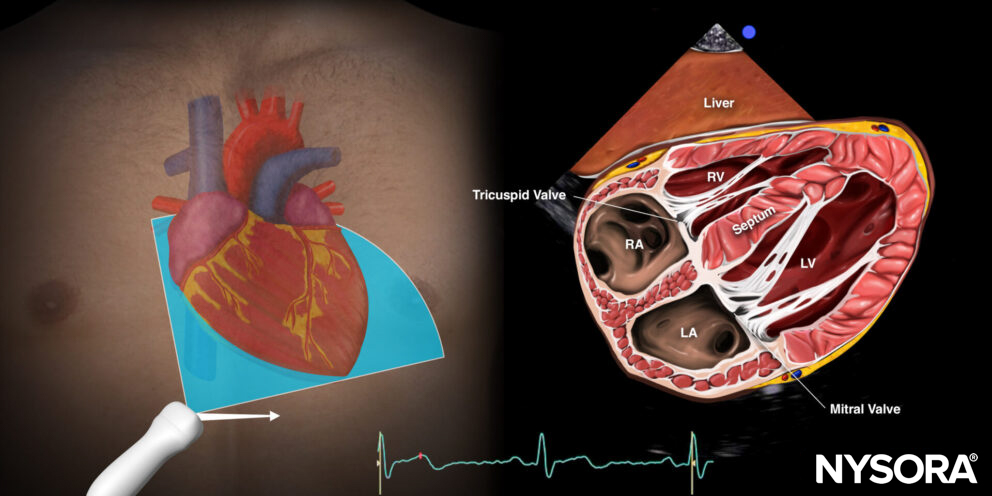
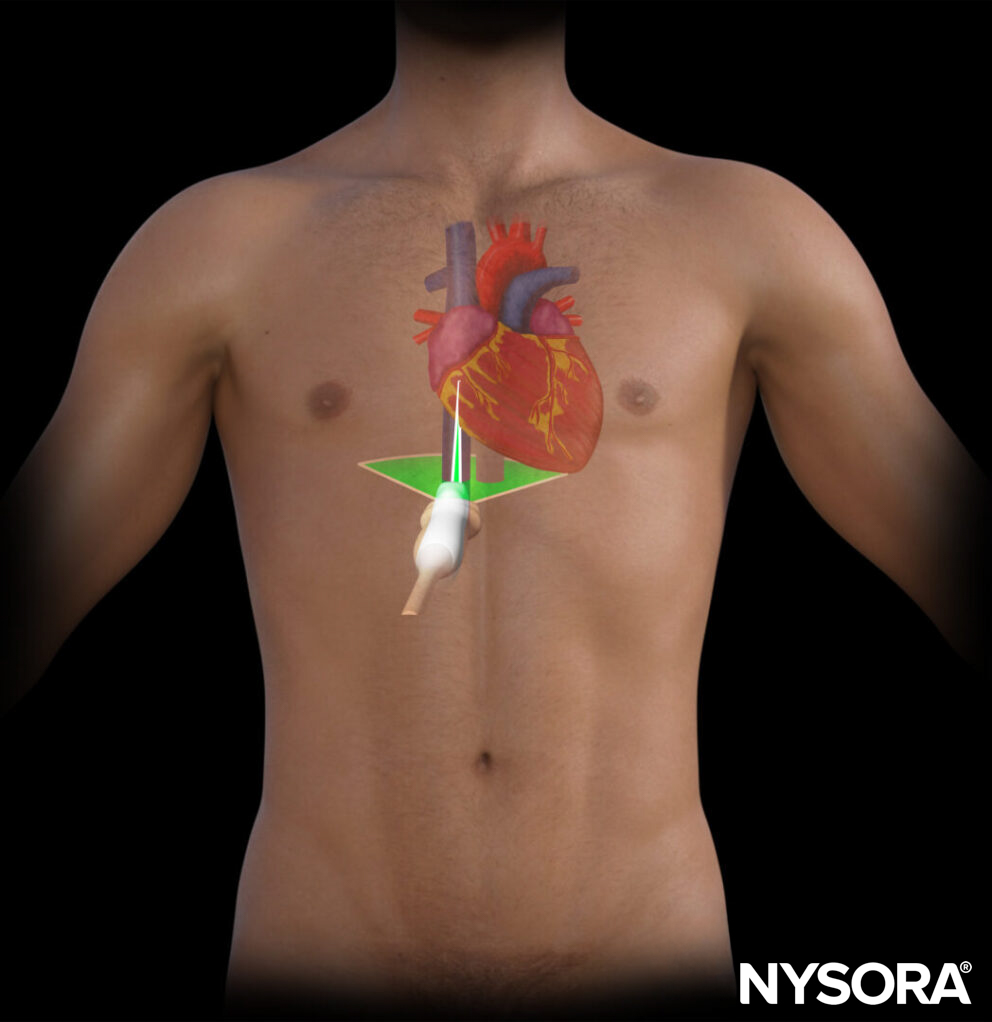
Subcostal (subxiphoid) four-chamber view (S4C)
Positioning:
Place the transducer with an overhand grip at the subcostal position with the transducer almost parallel to the skin and the index marker toward the patient’s left.
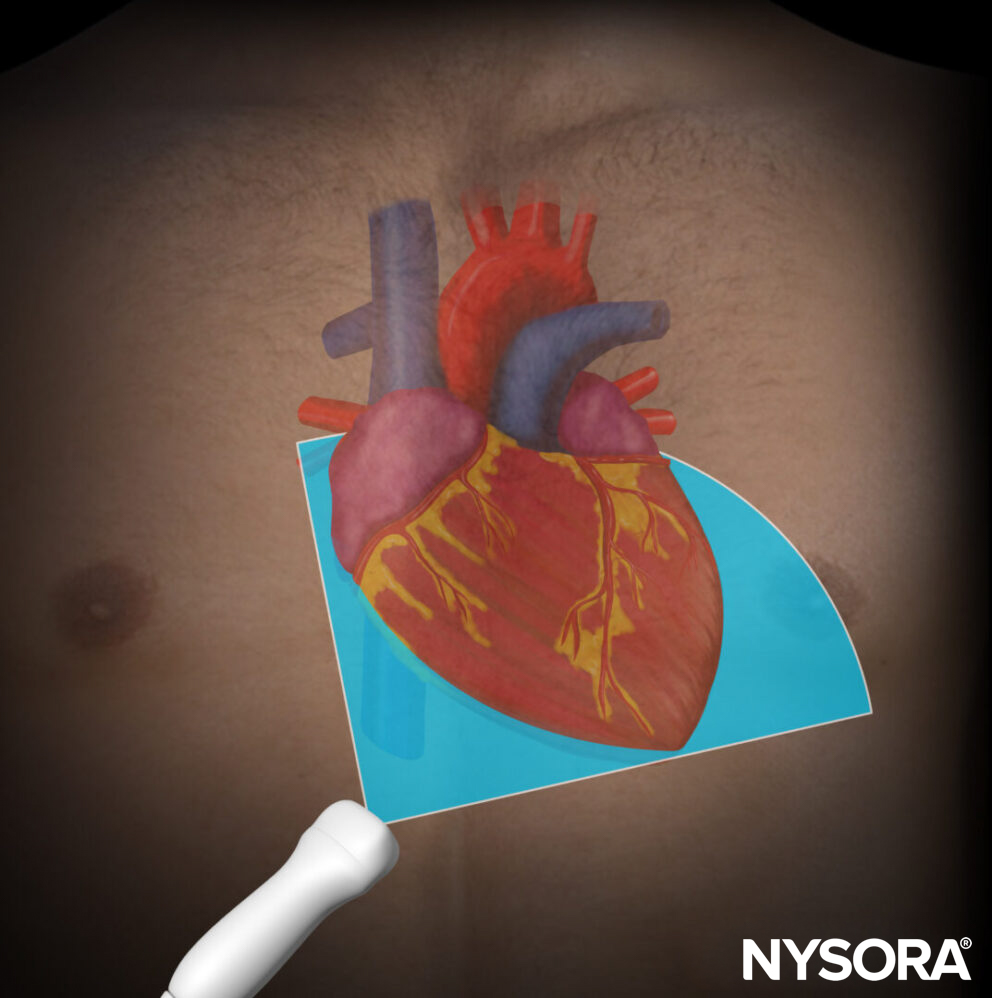
Transducer position for the subcostal four-chamber view.
Sonoanatomy:
The subcostal four-chamber view cuts the heart through the coronal plane.
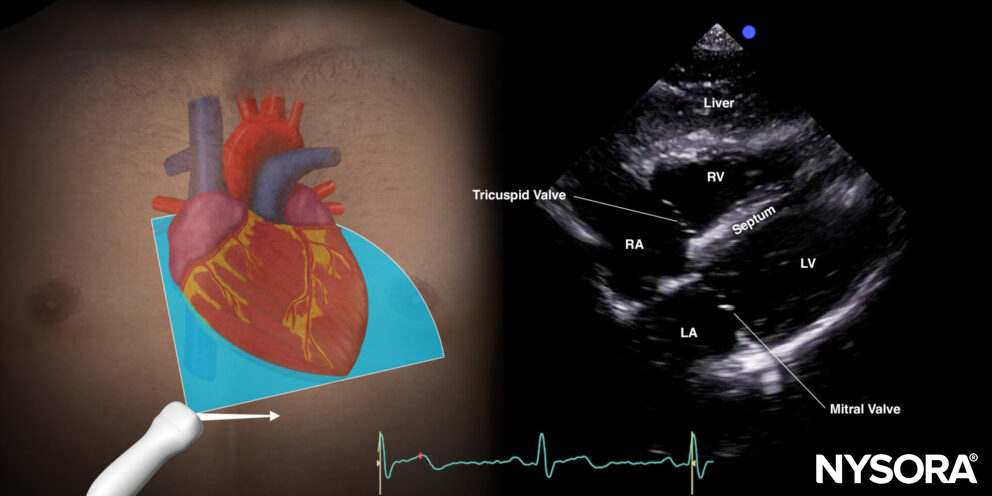
Sonoanatomy of the heart in the subcostal four-chamber view. Left atrium (LA), left ventricle (LV), right atrium (RA), right ventricle (RV), septum, tricuspid valve, mitral valve.
Reverse Utrasound Anatomy
Reverse Ultrasound Anatomy of the heart in the subcostal four-chamber view. Left atrium (LA), left ventricle (LV), right atrium (RA), right ventricle (RV), septum, tricuspid valve, and mitral valve.
Practical use:
- Right ventricle/left ventricle size
- Right ventricle/left ventricle function
- Pericardial effusion
- Cardiac arrest: Accessible/reliable window!
Tips
- It is important to understand that the liver serves as an acoustic window to visualize the heart.
- Asking the patient to hold their breath on inhalation or to bend their knees relaxes the abdominal muscles and can improve imaging.
- The subcostal 4-chamber view is an alternative view for when the apical 4-chamber view is difficult to obtain. The ventricle volume size, however, may be underestimated by the subcostal 4-chamber view.
- Try to image the left ventricle in its longest axis.
- The subcostal 4-chamber view may be challenging in obese or muscular patients.
In mechanically ventilated or COPD patients, hyperinflation can push the heart toward the abdomen, making it easier to obtain ultrasound images of the heart. - In case of cardiac arrest, a curved transducer can be used in the subxiphoid position.
Inferior vena cava view (IVC)
Positioning:
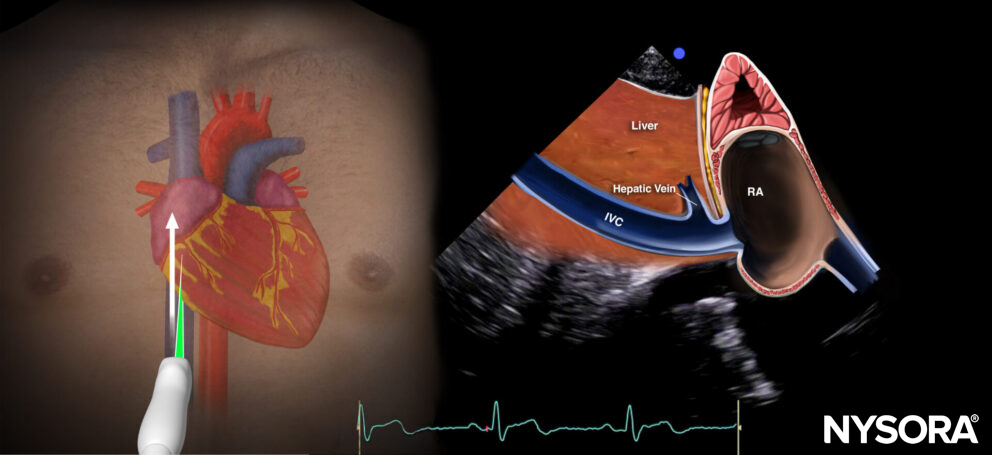
Place the transducer perpendicular to the skin in the subcostal position, with the index marker toward the patient’s left. After visualizing the inferior vena cava and the aorta, focus the ultrasound beam on the inferior vena cava and rotate the index marker 90 degrees counterclockwise (toward the head). Try to visualize its junction with the right atrium by rocking the transducer.
Rotational movement:
Initial transducer position and rotational movement to obtain the inferior vena cava view.
Final position:
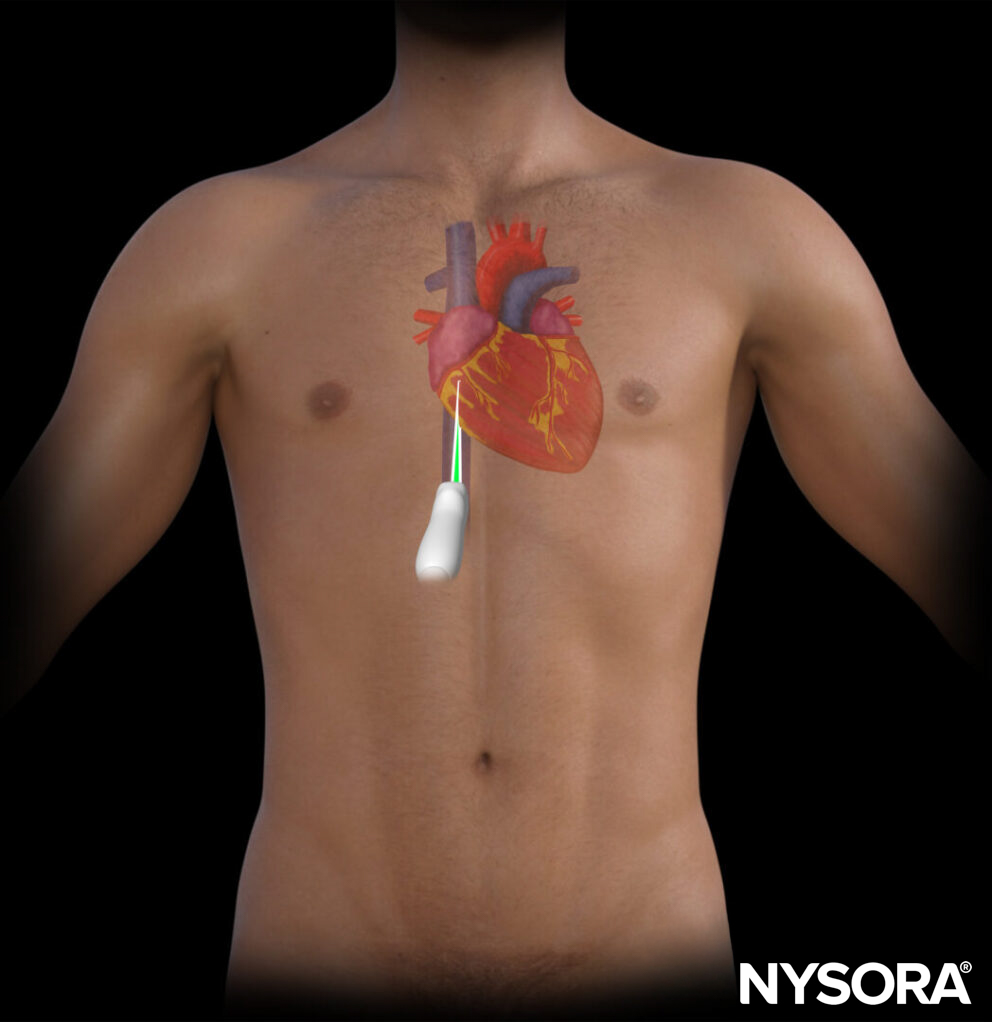
Final transducer position for the inferior vena cava view.
Sonoanatomy:
The inferior vena cava view cuts through the inferior vena cava and the right atrium.
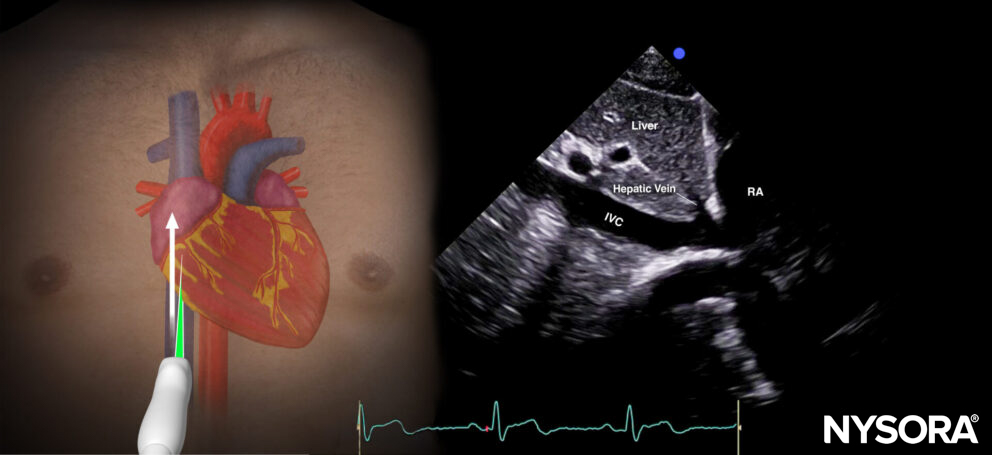
Sonoanatomy of the inferior vena cava view. Inferior vena cava (IVC), right atrium (RA), hepatic vein(sometimes), liver.
Reverse ultrasound anatomy:
Reverse Ultrasound Anatomy of the inferior vena cava view. Inferior vena cava (IVC), right atrium (RA), hepatic vein(sometimes), liver
Practical use:
- Volume status (inferior vena cava size variation)
- Compression of the right atrium in case of tamponade
Tips
- Volume status assessment by inferior vena cava size variation is not reliable in cases of increased right ventricular pressure or volume overload, since this will also lead to a dilated inferior vena cava.
- The aorta runs parallel to the inferior vena cava. Distinguish the inferior vena cava from the aorta! The aorta is surrounded by white, fatty tissue, has an angle toward the patient’s dorsum, and is pulsatile.
- The inferior vena cava runs intrahepatically and has a hepatic vein branch. In case of a dilated inferior vena cava, the aspect of the inferior vena cava and the hepatic vein is sometimes compared to a ‘Moose head’ or a ‘Playboy bunny’.
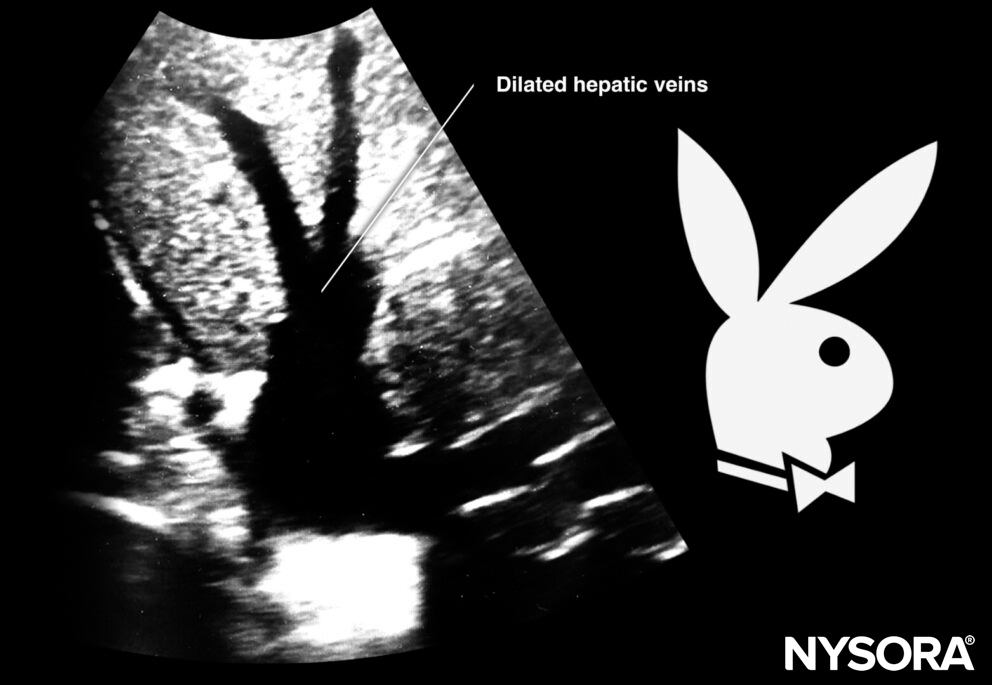
Sonoanatomy of dilated hepatic veins.
Overview
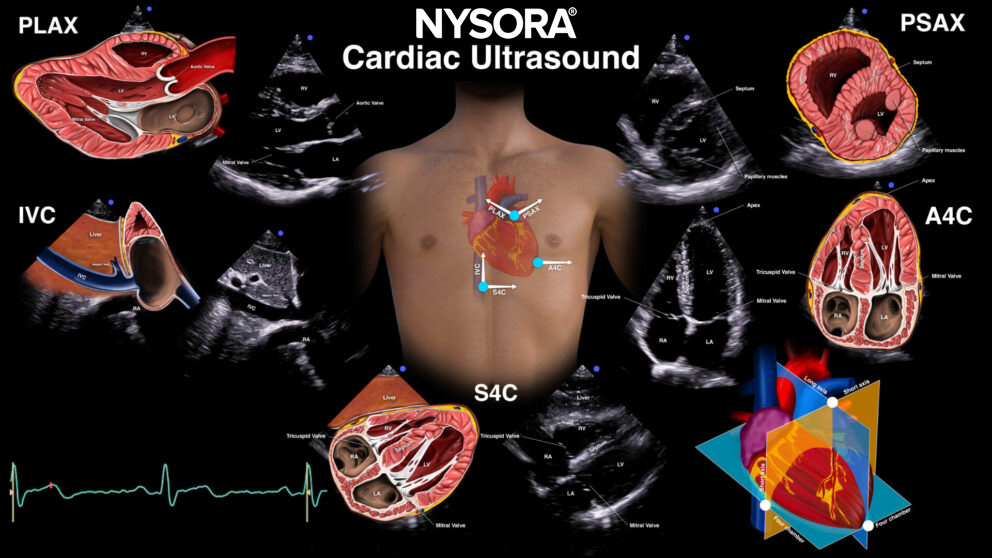
Different views according to the 3 transducer positions and 5 orientations for cardiac ultrasound. Parasternal long-axis (PLAX), parasternal short-axis (PSAX), apical four-chamber (A4C), Subcostal four-chamber (S4c), inferior vena cava (IVC).