Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About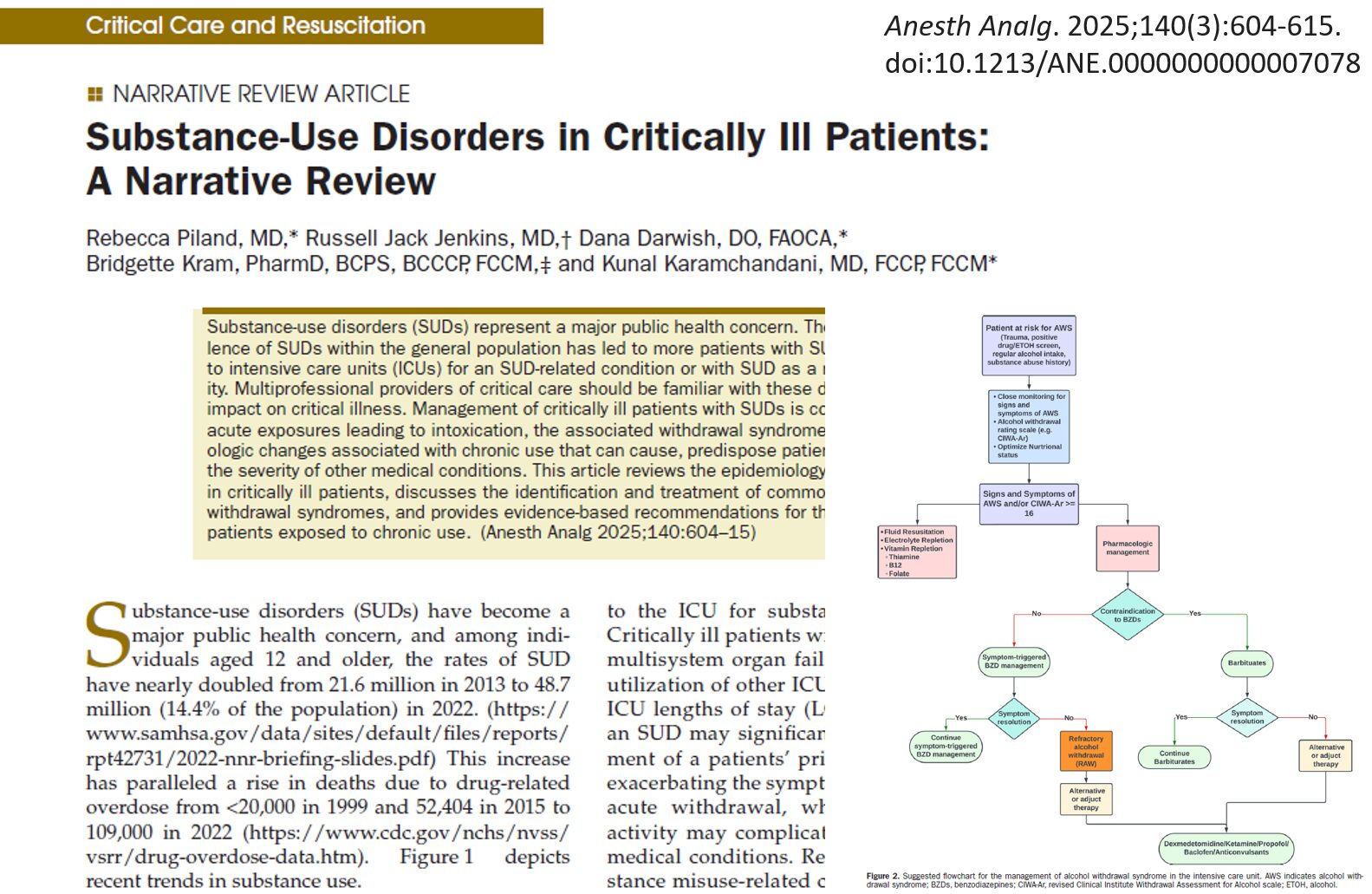





Substance use disorders (SUDs) are no longer just an emergency department issue—they’re a growing crisis in the ICU. Nearly 1 in 4 ICU admissions now involve SUD-related complications, leading to longer stays, worse outcomes, and higher resource use. A recent narrative review by Piland et al. (A&A, 2025) highlights the impact of SUDs on critically ill patients and provides essential management strategies.
Why This Topic Is Important
SUD prevalence has doubled in the past decade, affecting 48+ million Americans. These patients often require intensive interventions such as mechanical ventilation, high-dose sedation, and prolonged ICU stays. Without proper management, withdrawal syndromes, pain control challenges, and medication interactions can worsen outcomes.
How the Authors Did the Study
This narrative review compiles data from multiple studies on the prevalence, management strategies, and outcomes of patients with SUDs admitted to the ICU. The review categorizes key substances—including alcohol, opioids, cannabis, nicotine, and stimulants—and outlines evidence-based treatment approaches.
What the Authors Found
1. Alcohol Use Disorder (AUD)
- 8.6% of men and 1.7% of women globally suffer from AUD.
- AUD contributes to 10-20% of ICU admissions and leads to longer ICU stays.
- Alcohol withdrawal syndrome (AWS) is a major concern, with severe cases requiring intensive monitoring and treatment.
2. Opioid Use Disorder (OUD)
- 6.7 to 7.6 million U.S. adults are currently affected.
- ICU challenges include managing acute opioid overdose, pain control, and withdrawal.
- Opioid-induced hyperalgesia and post-ICU opioid dependence are major concerns.
3. Cannabis and the ICU
- Cannabis use has nearly doubled in the past 20 years.
- Chronic cannabis users may require higher doses of sedation and have increased risks of pulmonary complications.
4. Nicotine withdrawal in the ICU
- 25-47% of ICU patients are active smokers.
- Smoking increases risks of ARDS, postoperative complications, and ICU delirium.
- Nicotine withdrawal symptoms can worsen ICU agitation and require careful management.
5. Stimulant use and critical illness
- Cocaine and methamphetamine use increase the risk of myocardial infarction, stroke, and ICU admissions.
- Patients may present with acute agitation, hallucinations, and cardiovascular instability.
Breaking It Down: The Bigger Picture
- Patients with SUDs require more ICU resources, including sedation, mechanical ventilation, and hemodynamic support.
- Untreated withdrawal can lead to worse outcomes and prolonged ICU stays.
- Multimodal pain management strategies are critical in opioid-tolerant patients to prevent over-sedation and opioid-induced hyperalgesia.
- Early involvement of addiction specialists can improve long-term outcomes.
Key Clinical Practice Recommendations
- Screen for SUDs early in ICU admissions—many patients may not disclose their history.
- Manage alcohol withdrawal aggressively with symptom-based treatment (CIWA-Ar scale) and consider dexmedetomidine or ketamine in patients resistant to benzodiazepines.
- Use multimodal pain management (regional anesthesia, NSAIDs, acetaminophen) to reduce opioid use and monitor mechanically ventilated patients for opioid withdrawal, particularly if they’ve been on long-term infusions.
- Be aware of cannabis-related effects, such as increased sedation requirements and pulmonary complications, and avoid abrupt discontinuation of opioid agonist therapies (buprenorphine, methadone) in patients with OUD.
- Address nicotine withdrawal proactively to reduce ICU agitation, improve ventilator synchronization, and ensure proper follow-up with addiction services upon discharge to reduce hospital readmissions.
For more information on managing SUDs, check out Anesthesia Updates on the NYSORA Anesthesia Assistant App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.
Reference: Piland R, Jenkins RJ, Darwish D, Kram B, Karamchandani K. Substance-Use Disorders in Critically Ill Patients: A Narrative Review. Anesth Analg. 2025;140(3):604-615.