Learning objectives
- Indications for rigid bronchoscopy
- Advantages and disadvantages of rigid bronchoscopy
- Anesthesia management for rigid bronchoscopy
Definition and mechanism
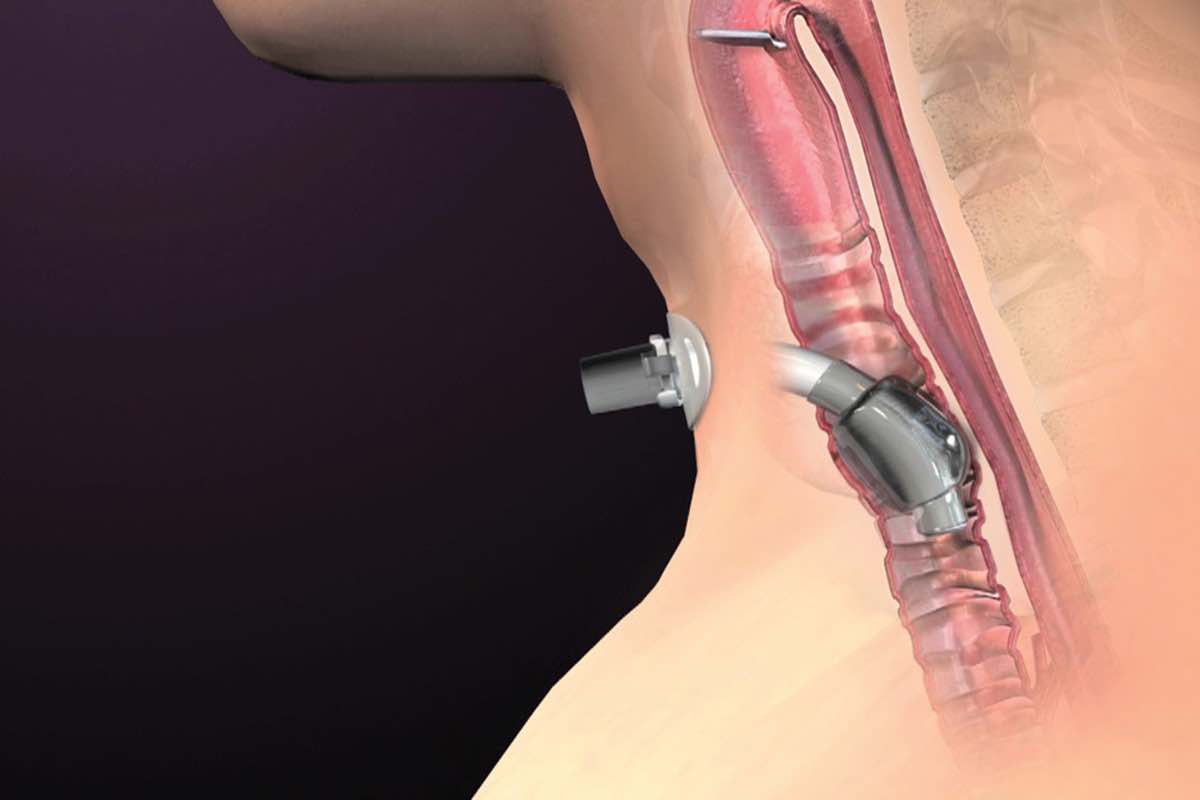
- To gain better access to the patient’s airway
- Allows insertion of instruments or airway devices
- Diagnosis of infections, cancers, inflammatory conditions, sarcoidosis, and lymphoma
- Treatment of airway obstruction, airway narrowing (stenosis), airway cancers, bleeding
- Removal of foreign or aspirated objects
- Considerations for surgical technique: stenting, laser, endobronchial electrosurgery, argon plasma coagulation, & balloon bronchoplasty
| Advantages | Disadvantages |
|---|---|
| Can be inserted past airway obstruction | Requires always general anesthesia |
| The airway is secure during the procedure | Oral and pharyngeal damage |
| Allows for: Larger biopsies Tamponade (stop) bleeding areas Removal of airway tumors and foreign objects Deploying airway devices (tracheobronchial stents) to keep collapsing airways open | Limited visualization |
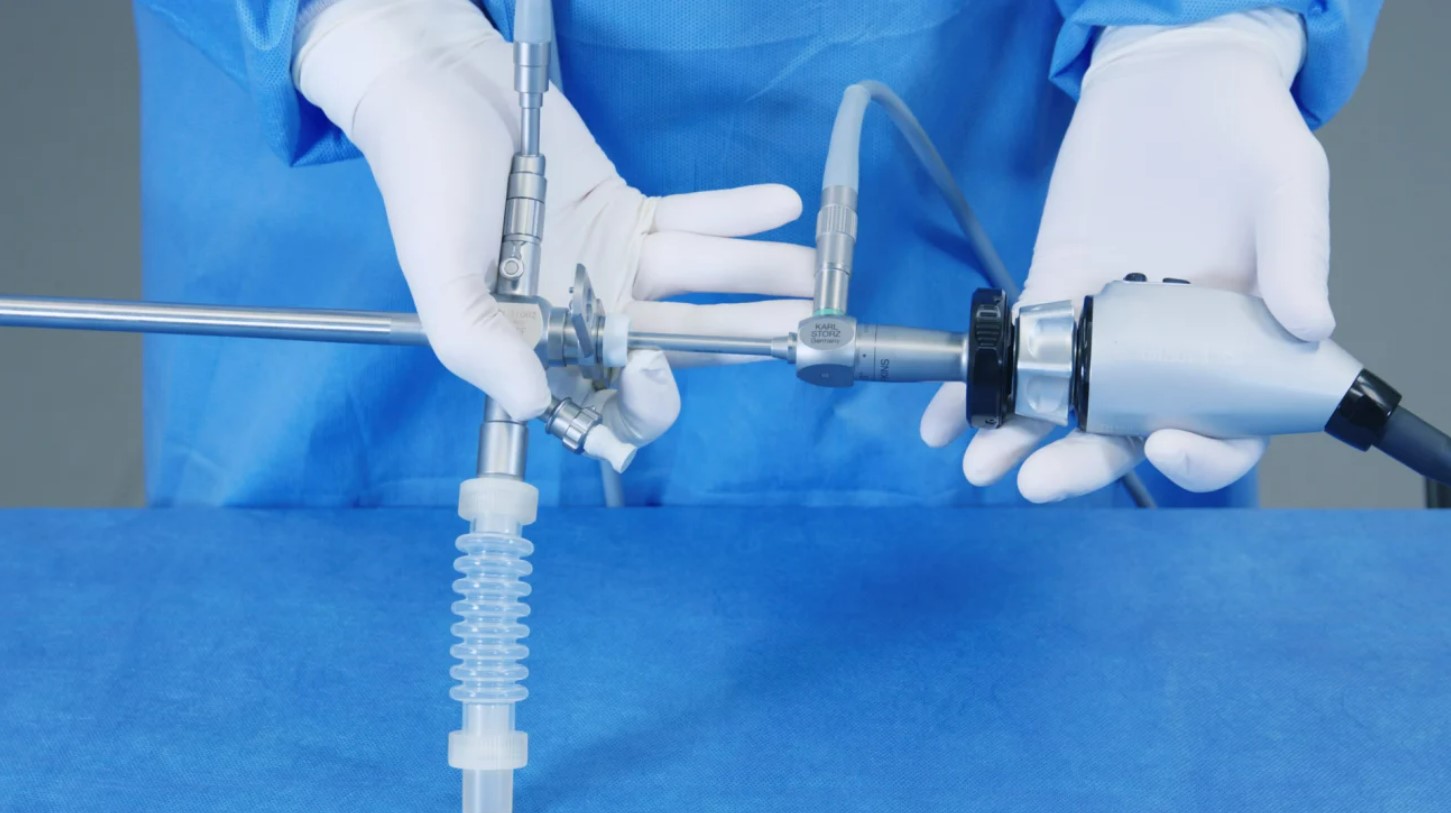
| Nonflexible metal rod |
Factors that complicate rigid bronchoscopy
- Patients requiring high levels of supplemental O2
- Patients with baseline hypercarbia and hemodynamic instability
- Unstable cervical spine or diminished range of motion of the cervical spine caused by spondylosis
- Maxillofacial trauma or oral disease preventing opening of the jaw (stenosis, obstructing neoplasms)
- Procedure-specific complications: hemorrhage, airway trauma, perforation, fire, systemic gas embolism, & dissemination of post-obstructive pneumonia
Management
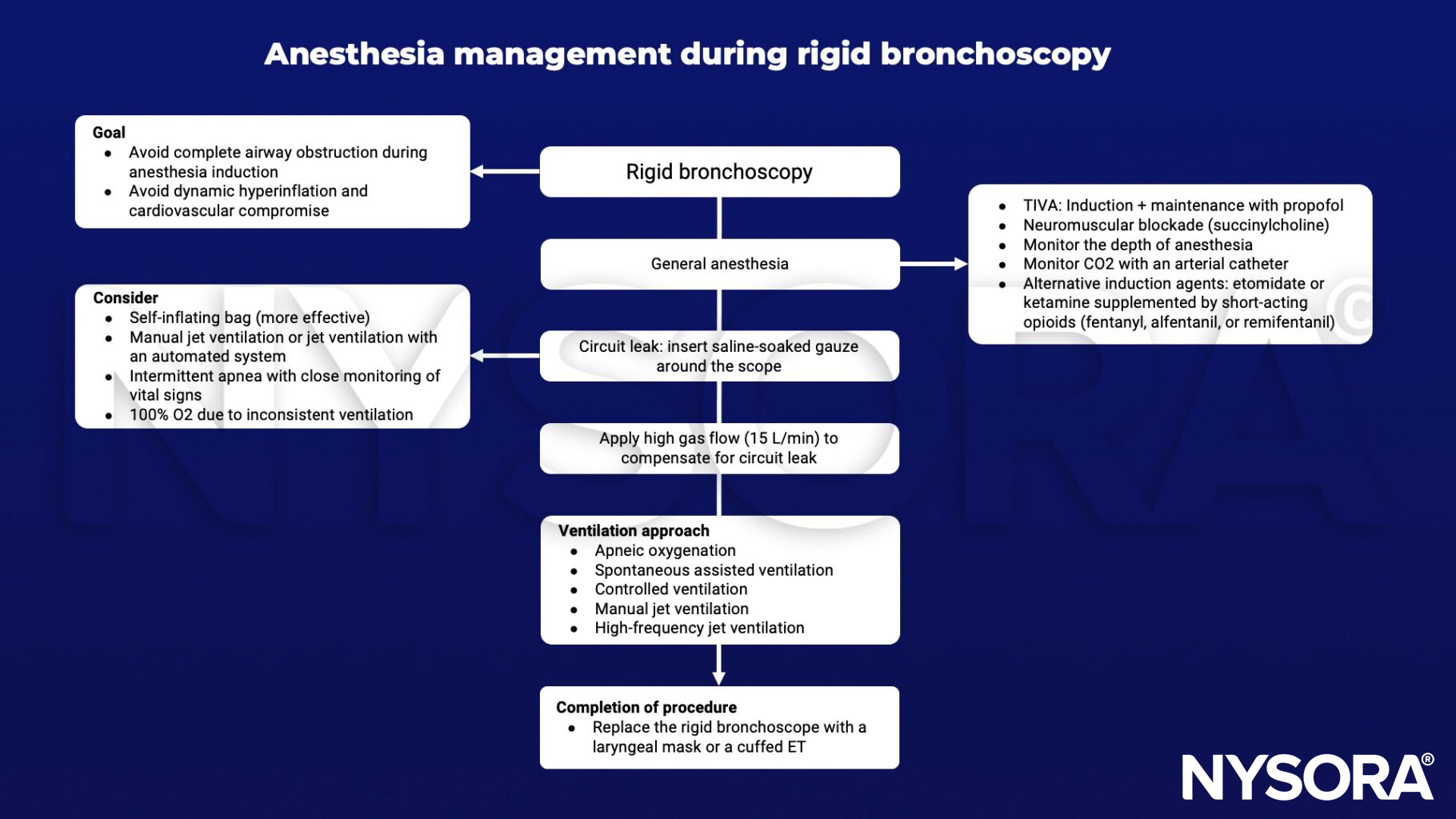
Keep in mind
- Full stomach vs. unsecured airway
- High oxygen requirements with risk of fire ignition
- Jet ventilation through obstructing stenoses with risk of air trapping & barotrauma
Suggested reading
- Galway U, Zura A, Khanna S, Wang M, Turan A, Ruetzler K. Anesthetic considerations for bronchoscopic procedures: a narrative review based on the Cleveland Clinic experience. J Thorac Dis. 2019;11(7):3156-3170.
- Kabadayi, Selin & Bellamy, Mark. (2016). Bronchoscopy in critical care. BJA Education. 17. mkw040. 10.1093/bjaed/mkw040.
- Pathak V, Welsby I, Mahmood K, Wahidi M, MacIntyre N, Shofer S. Ventilation and anesthetic approaches for rigid bronchoscopy. Ann Am Thorac Soc. 2014;11(4):628-634.
Clinical updates
Tsan et al. (A&A Practice, 2025) describe successful awake rigid bronchoscopy in a 70-year-old woman with near-total tracheal obstruction (0.4 cm lumen) from anaplastic thyroid cancer, using ultrasound-guided bilateral superior laryngeal nerve blocks combined with glossopharyngeal topicalization and minimal sedation (dexmedetomidine and remifentanil) to maintain spontaneous ventilation. Mechanical coring via the rigid bronchoscope restored airway patency and enabled a bronchoscopy-guided awake tracheostomy without hypoxemia or hemodynamic instability, supporting awake rigid bronchoscopy with targeted airway anesthesia as a viable option in impending “cannot intubate, cannot ventilate” scenarios.
Aravena and Mehta (Current Opinion in Pulmonary Medicine, 2025) review contemporary evidence comparing rigid (RB) and flexible bronchoscopy (FB), highlighting that advanced guided and robotic bronchoscopy now achieve diagnostic yields up to 80–90% for peripheral pulmonary nodules, though meta-analyses suggest overall yields have plateaued and remain below CT-guided biopsy with substantially lower pneumothorax rates. For central airway obstruction, large registry data (EpiGETIF) demonstrate ≥96% technical success with therapeutic rigid bronchoscopy and significant dyspnea reduction, while newer flexible modalities (CO₂ laser, microwave ablation, metallic stents) show high procedural success (≈89%) with low complication rates, supporting a complementary RB–FB strategy tailored to airway control needs, bleeding risk, and stent selection.
Chavoshi et al. (Anesthesia and Pain Medicine, 2024) conducted a randomized trial of 60 children undergoing rigid bronchoscopy for foreign body removal, comparing spontaneous ventilation (sevoflurane + propofol) with controlled ventilation using atracurium or rocuronium, finding significantly higher rates of bucking, laryngospasm, and lower minimum oxygen saturation in the spontaneous ventilation group. Controlled-ventilation groups required fewer propofol boluses, had higher pulmonologist satisfaction scores, and experienced fewer intraoperative airway complications without prolonging anesthesia or bronchoscopy duration, supporting low-dose non-depolarizing muscle relaxants, particularly rocuronium, as a safer strategy in pediatric rigid bronchoscopy.