Learning objectives
- Recognize Neuroleptic malignant syndrome (NMS)
- Management of NMS
Definition and mechanisms
- Neuroleptic malignant syndrome (NMS) is a rare, potentially fatal neurological condition caused by an adverse reaction to neuroleptic (haloperidol) or antipsychotic agents
- Caused by either treatment with dopamine receptor antagonists or by the withdrawal of dopamine receptor agonists
- This leads to an acute blockade of dopaminergic transmission in the:
- Nigrostriatum – which produces rigidity
- Hypothalamus – which produces hyperthermia
- Corticolimbic system – which produces an altered mental state
- Usually develops within the first 2 weeks of treatment with the agent but can occur at any time
- The mortality risk is 10%
- Clinical manifestations: remember the mnemonic FEVERS:
- Fever
- Encephalopathy
- Vital signs unstable
- Elevated labs
- Rigidity (vs myoclonus in serotonin syndrome)
- Sweating
Signs and symptoms
- Muscle cramps
- Tremors
- Fever
- Sweating
- Unstable blood pressure
- Stupor
- Muscular rigidity
- Autonomic dysfunction
- Confusion
- Agitation
- Delirium
- Tachycardia
Risk factors
- Dehydration
- Agitation
- Catatonia
- Typical neuroleptics: e.g. haloperidol, chlorpromazine
- Atypical neuroleptics: e.g. olanzapine, clozapine, risperidone
- Anti-dopaminergic antiemetics: e.g. droperidol
- Withdrawal of Dopaminergic Agents: levodopa, amantadine
Complications
| Respiratory | Secondary infection Aspiration pneumonia |
| Cardiovascular | Cardiac arrhythmias Pulmonary embolism |
| Musculoskeletal | Peripheral neuropathy Rhabdomyolysis → myoglobunuria |
Criteria for diagnosis
| Major criteria | Minor criteria |
|---|---|
| High fever Muscular rigidity Elevated serum creatine kinase | Tachycardia Raised blood pressure Tachypnea Altered consciousness level Sweating |
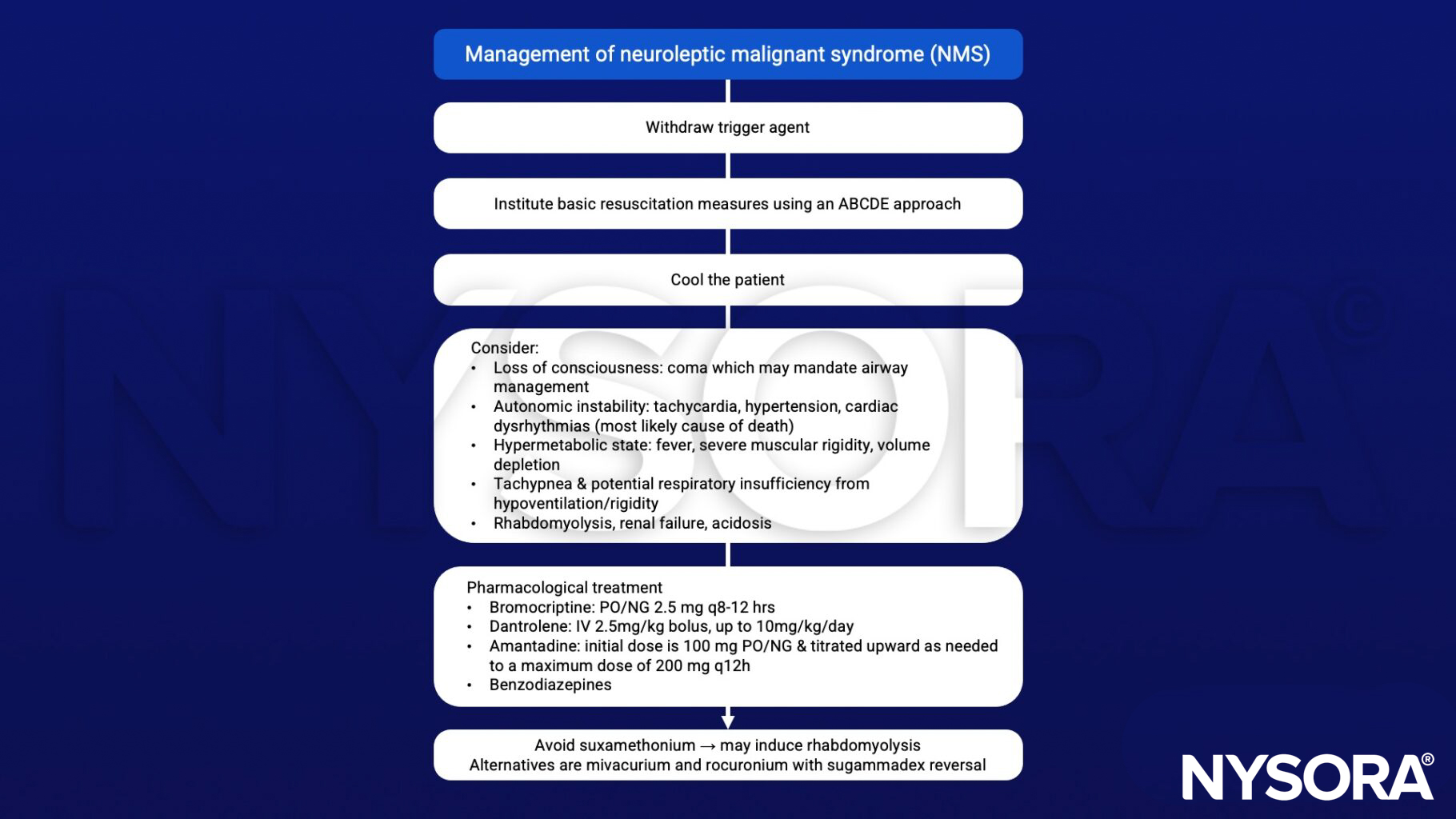
Management
Suggested reading
- Bartakke, A., Corredor, C., Van Rensburg, A., 2020. Serotonin syndrome in the perioperative period. BJA Education 20, 10–17.
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Adnet, P., Lestavel, P., Krivosic-Horber, R., 2000. Neuroleptic malignant syndrome. British Journal of Anaesthesia 85, 129–135.
Clinical updates
Wijdickset al. (New England Journal of Medicine, 2024) provide an updated critical care–focused review of neuroleptic malignant syndrome (NMS), emphasizing that although incidence remains low (0.02–3%), mortality has declined to 4.7% at 30 days but can reach 15% at 1 year due to late complications such as aspiration pneumonia and renal failure. They detail contemporary ICU management, including early airway protection, aggressive fluid resuscitation targeting urine output of 200–300 mL/hr for rhabdomyolysis, surface cooling plus acetaminophen for hyperthermia, and escalation to dantrolene, bromocriptine, amantadine, or electroconvulsive therapy in severe cases with core temperatures ≥38–40°C and marked rigidity. The review also highlights emerging insights into differential diagnosis (notably distinguishing NMS from serotonin syndrome and malignant hyperthermia), limited evidence for genetic susceptibility, and a relatively low but persistent recurrence risk (5 of 119 rechallenged patients in one nationwide study), supporting cautious reintroduction of low-potency agents when necessary.
Funcis et al. (European Journal of Neurology, 2024) reported that among 5,108 patients treated with dopamine receptor–blocking agents and/or tetrabenazine, only one case of neuroleptic malignant syndrome (NMS) was recorded, suggesting either extreme rarity or significant underrecognition. Through a case report and literature review (11 total cases), they identified advanced disease stage, rigid, akinetic/Westphal phenotype, dehydration, polytherapy, and abrupt medication changes as key risk factors, and emphasized that atypical NMS (e.g., hyperthermia without rigidity) may be overlooked in HD due to hypothalamic degeneration and masking by baseline motor symptoms.