Learning objectives
- Definition, diagnosis, and management of hyperkalemia
Definition
- Hyperkalemia is an elevated level of potassium (K+) in the blood:
- Mild: a serum K+ 5.5 – 5.9 mmol/L
- Moderate: a serum K+6.0-6.4 mmol/L
- Severe: a serum K+ ≥ 6.5 mmol/L
Signs and symptoms
- Gastro-intestinal
- Nausea
- Vomiting
- Diarrhea
- Neuromuscular
- Paresthesias
- Muscle fasciculations
- Ascending paralysis of the extremities (quadriplegia)
- Cardiac
- Dyspnea
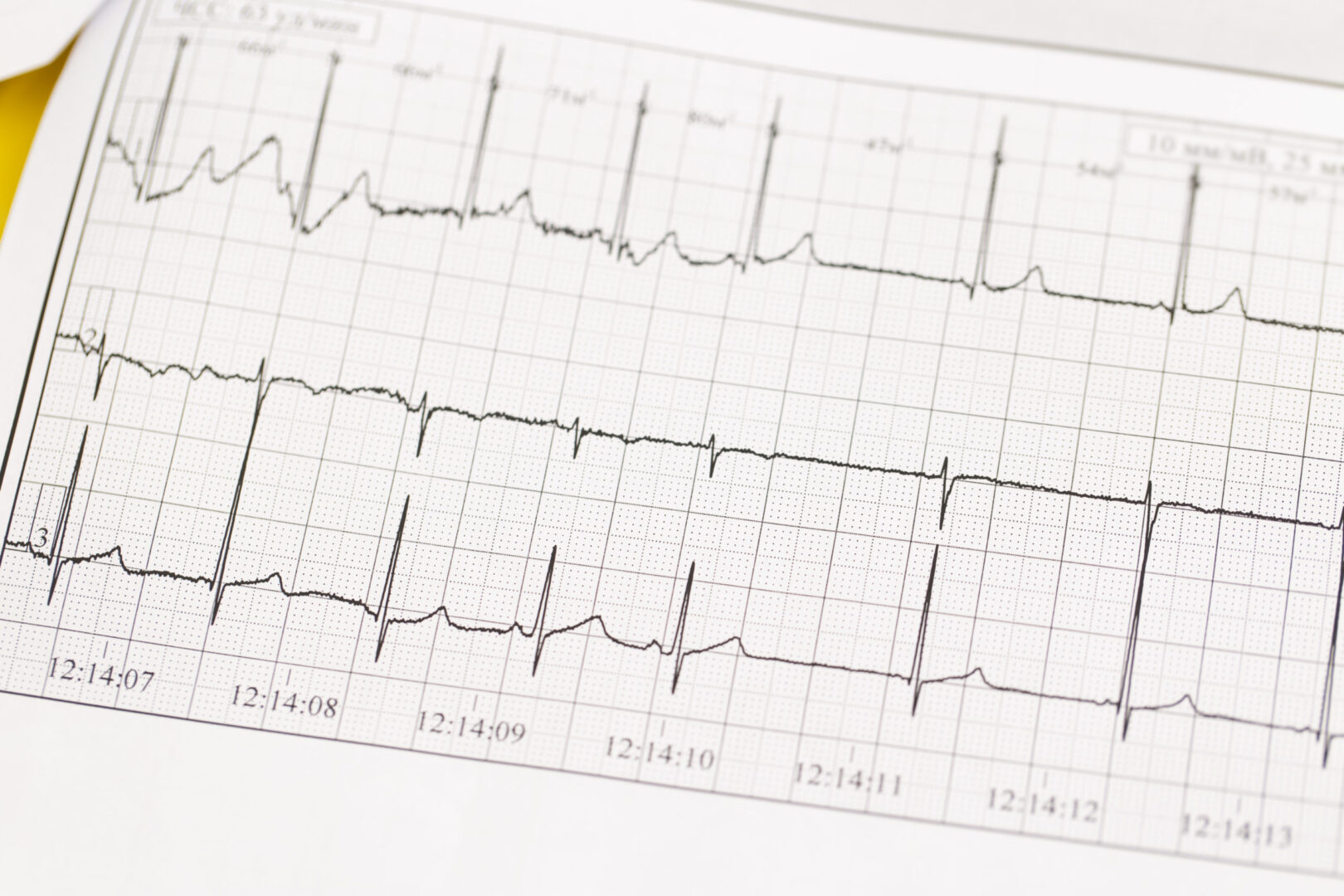
- Progressive ECG changes with increasing severity of hyperkalemia
- Peaked T wave
- Wide PR interval
- Wide QRS duration
- Loss of P wave
- Sinusoidal wave
Causes
| Renal failure | |
| Medications | Angiotensin-converting enzyme inhibitors (ACE-i) Angiotensin II receptor blockers (ARB) Potassium-sparing diuretics Non-steroidal anti-inflammatory drugs (NSAIDs) Beta-blockers Trimethoprim (antibiotic) |
| Tissue breakdown | Rhabdomyolysis Trauma |
| Endocrine disorders | Diabetes mellitus type 2 Adrenocortical insufficiency |
Management
- First, ensure that the lab result is correct and rule out pseudohyperkalemia
- Typical examples:
- Poor storage of blood specimens
- Long transport time from blood draw of the sample to processing in the lab

Suggested reading
- Lott C, Truhlář A, Alfonzo A, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances [published correction appears in Resuscitation. 2021 Oct;167:91-92]. Resuscitation. 2021;161:152-219.
- Palmer BF, Carrero JJ, Clegg DJ, et al. Clinical Management of Hyperkalemia. Mayo Clin Proc. 2021;96(3):744-762.
- Palmer BF, Clegg DJ. Diagnosis and treatment of hyperkalemia. Cleve Clin J Med. 2017;84(12):934-942. doi:10.3949/ccjm.84a.17056
Clinical updates
Jessen et al. (Resuscitation, 2025) conducted a systematic review and meta-analysis showing that insulin with glucose lowers serum potassium by about 0.7 mmol/L within 60 minutes, while inhaled or IV beta₂-agonists (e.g., salbutamol) reduce potassium by 0.9–1.0 mmol/L, with combination therapy achieving up to a 1.2 mmol/L reduction. In contrast, bicarbonate showed no meaningful potassium-lowering effect, and there is no high-quality evidence that calcium improves outcomes beyond membrane stabilization. These findings support insulin–glucose and beta₂-agonists as first-line therapies for acute hyperkalemia and call for re-evaluation of routine bicarbonate and calcium use.
Glahn et al. (British Journal of Anaesthesia, 2025) highlight in the updated 2024 EMHG guidelines that severe hyperkalemia is a key life-threatening feature of malignant hyperthermia (MH) and requires immediate treatment alongside dantrolene. Recommended management includes IV insulin with dextrose, IV calcium chloride or gluconate for membrane stabilization, beta₂-agonists, and dialysis in refractory cases, with close potassium and ECG monitoring. The guideline reinforces structured, protocol-driven hyperkalemia treatment as a core component of MH crisis management to prevent arrhythmias and cardiac arrest.
- Read more about this study HERE.