Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About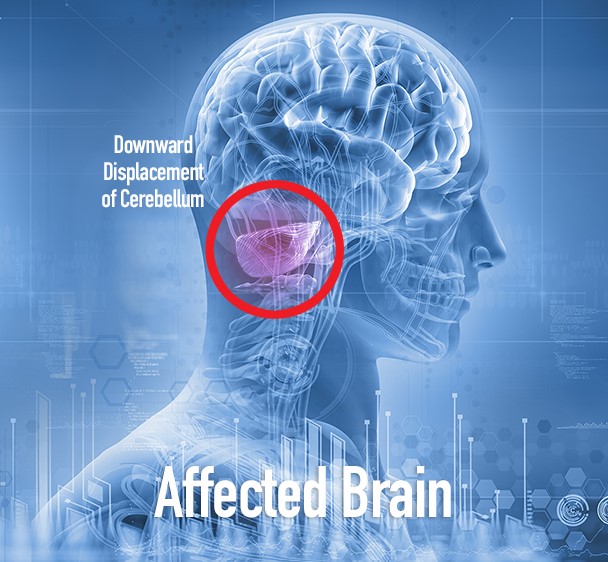
Learning objectives
- Types of a Chiari malformation
- Management of a Chiari malformation
Definition and mechanisms
- Chiari malformation is a structural defect in the cerebellum, characterized by a downward displacement of one or both cerebellar tonsils through the foramen magnum
- Occurs when part of the skull is misshapen or smaller than typical, pressing on the brain and forcing the brain downward
- Congenital causes include hydrocephalus, craniosynostosis, hyperostosis, X-linked vitamin D-resistant rickets, and neurofibromatosis type I
- Acquired disorders include space-occupying lesions due to brain tumors or hematomas and traumatic brain injury
- Most patients have no signs or symptoms and do not require treatment
- Other conditions associated with Chiari malformation include:
- Hydrocephalus
- Syringomyelia
- Spina bifida
- Spinal curvature
- Tethered spinal cord syndrome
- Ehlers-Danlos syndrome
- Marfan syndrome
Types of Chiari malformation
- The type depends on the anatomy of the brain tissue that is displaced and whether developmental problems are present:
| Type 1 | Type 2 | Type 3 | Type IV |
|---|---|---|---|
| Occurs when the lower part of the cerebellum pushes into the foramen magnum Signs or symptoms may not occur until late childhood or adulthood and is often first noticed by accident during an examination for another condition Most common type and is not considered life-threatening | Congenital pediatric forms A greater amount of cerebellum and brain stem tissue extends into the spinal compared with that in Chiari malformation type 1 The nerve tissue connecting both halves of the cerebellum may be missing or only partially formed Nearly always accompanied by myelomeningocele, a form of spina bifida that occurs when the spinal canal and backbone do not close before birth Often seen on ultrasound during pregnancy Symptoms of Type II usually appear during childhood and are generally more severe than in Type 1 The term Arnold-Chiari malformation is specific to Type II malformations | Most serious form A portion of the lower back part of the cerebellum or the brainstem extends through an abnormal opening in the back of the skull, even possibly the membranes surrounding the brain or spinal cord Diagnosed with ultrasound during pregnancy or at birth Can cause debilitating and life-threatening complications Associated with severe neurological defects | An incomplete or underdeveloped cerebellum (cerebellar hypoplasia) The cerebellum is in its normal position but parts are missing and portions of the skull and spinal cord may be visible |
Signs and symptoms
- Neurogenic dysphagia
- Cyanosis
- Weak crying
- Facial weakness
- Aspiration
- Headaches
- Tinnitus
- Lhermitte’s sign
- Vertigo (dizziness)
- Nausea
- Schmahmann syndrome
- Nystagmus
- Facial pain
- Muscle weakness
- Impaired gag reflex
- Restless leg syndrome
- Sleep apnea
- Sleep disorders
- Impaired coordination
- Severe cases may develop all the symptoms and signs of a bulbar palsy
- Paralysis
- Papilledema on the fundoscopic exam due to increased intracranial pressure
- Pupillary dilation
- Dysautonomia:
- Tachycardia
- Syncope
- Polydipsia
- Chronic fatigue
- Opisthotonos
- Stridor
Diagnosis
- Patient history
- Neurological examination
- MRI/CT
- Ultrasound for Chiari II malformation
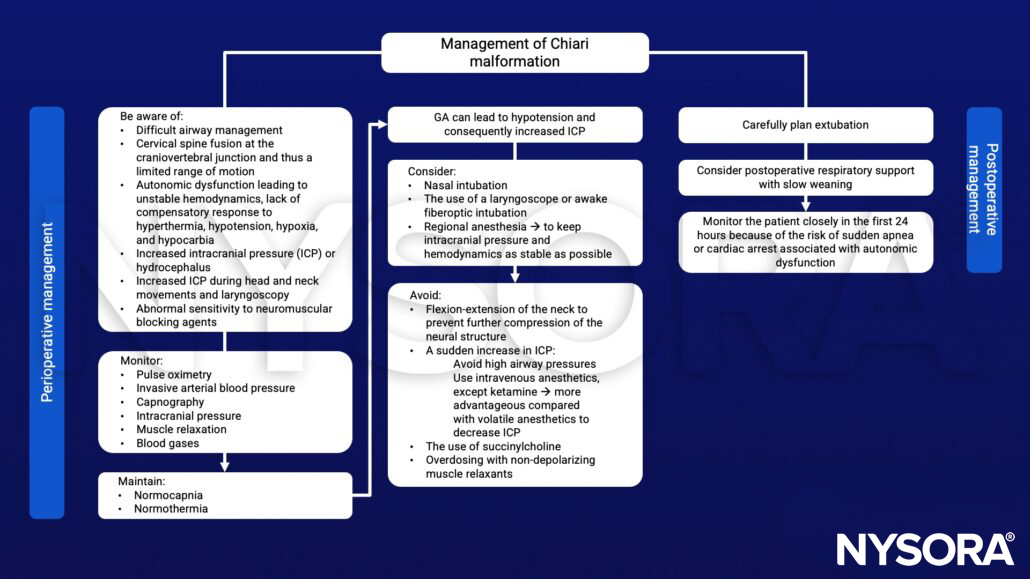
Management
Suggested reading
- Coviello A, Golino L, Posillipo C, Marra A, Tognù A, Servillo G. Anesthetic management in a patient with Arnold-Chiari malformation type 1,5: A case report. Clin Case Rep. 2022;10(2):e05194.
- Anesthetic management of a patient with Arnold-Chiari malformation type I with associated syringomyelia: A case report Anesth Pain Med. 2012;7(2):166-169.