Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About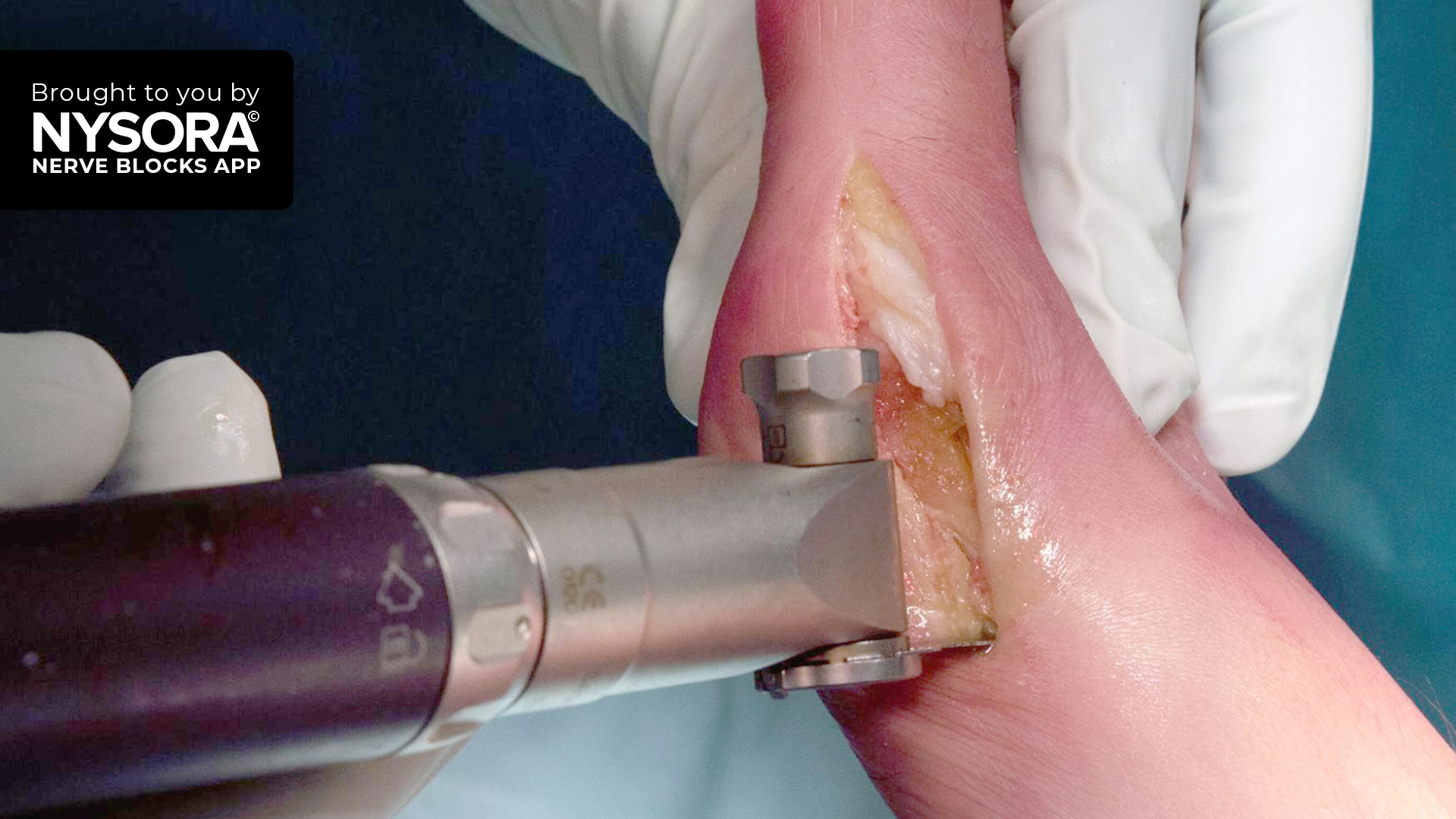



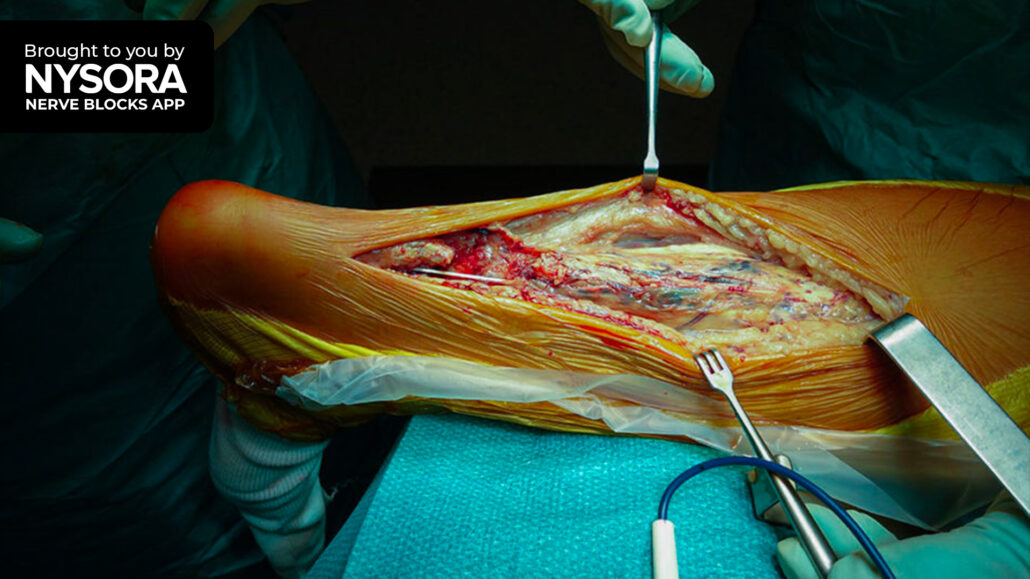
Case presentation
A 50-year-old female patient, with no significant medical history, was scheduled for an elective surgical procedure to correct a bunion on her right foot. This hallux valgus (i.e., bunion)—a deformity of the joint connecting the big toe to the foot—had been causing her increasing pain and discomfort, negatively impacting her daily activities and limiting her choice of footwear. When conservative measures proved inadequate for symptomatic relief, surgery was recommended.

Nerve block techniques
An ultrasound-guided ankle block was planned to provide effective regional anesthesia for foot surgery, allowing direct visualization of the nerves and adjacent structures to improve block efficacy and safety.
A comprehensive ankle block, targeting all five nerves, is not mandatory. It is sufficient to anesthetize only the tibial, deep peroneal, and superficial peroneal nerves. Priority should be given to blocking the tibial nerve first due to its size and critical role in achieving anesthesia, alongside its relatively longer onset time.
- Patient position: The patient was positioned supine with the leg slightly elevated to facilitate scanning around the ankle.
- Ultrasound scanning: Utilizing a high-frequency linear transducer, positioned transversely over the ankle, the specific nerves intended for the block were located.
- Needle insertion: A 25-gauge needle was inserted in-plane to inject the local anesthetic in the fascial plane enveloping the nerve.
Local anesthetic choice and volume: The local anesthetic administration involved injecting 5 mL of 0.5% bupivacaine around the tibial nerve and 3 mL of the same concentration at both the superficial and deep peroneal nerves.
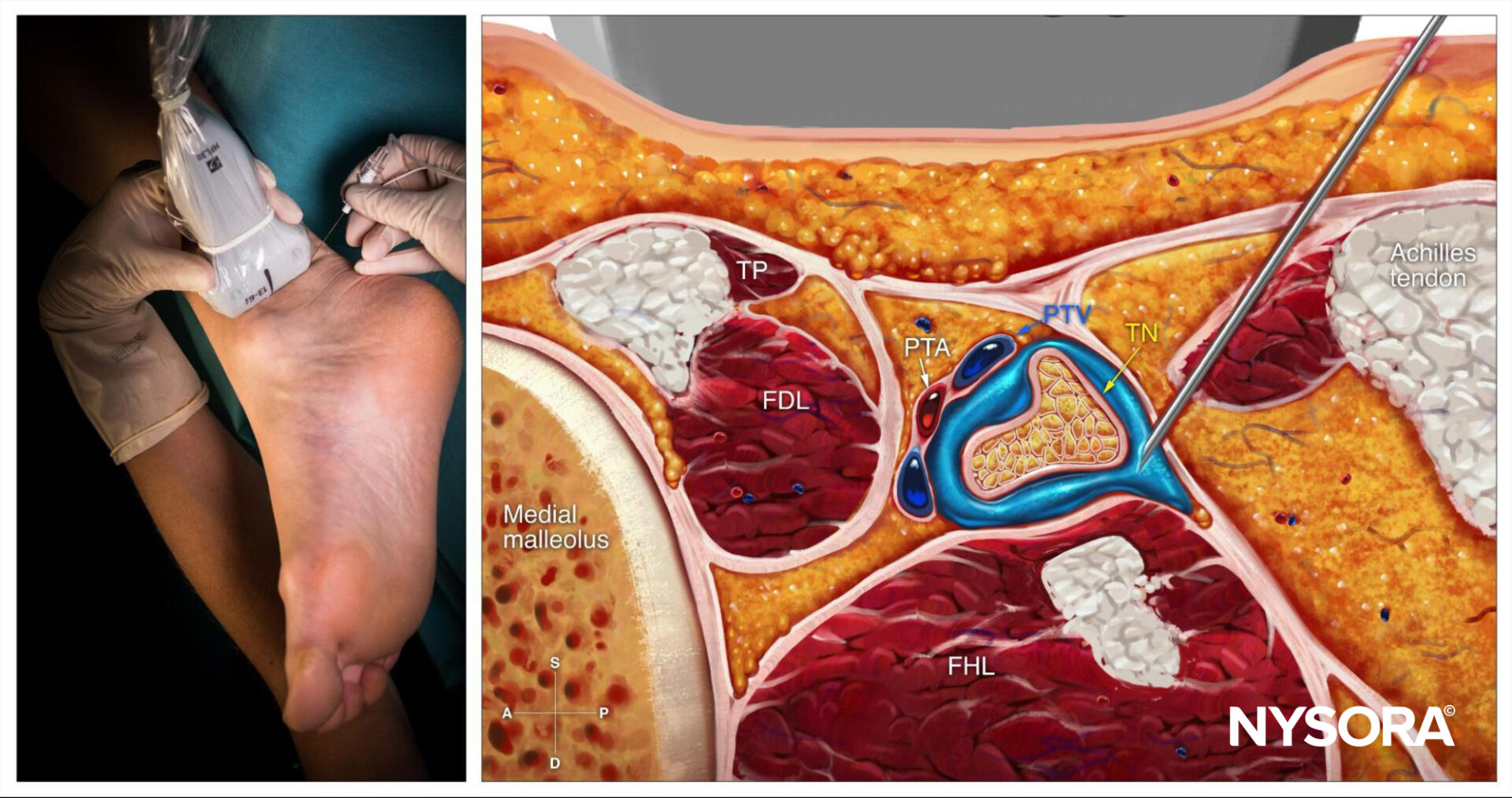
Reverse Ultrasound Anatomy for a tibial nerve block at the ankle level with needle insertion in-plane and local anesthetic spread. TP, tibialis posterior muscle; FDL, flexor digitorum longus; PTA, posterior tibial artery; PTV, posterior tibial vein; TN, tibial nerve; FHL, flexor hallucis longus.
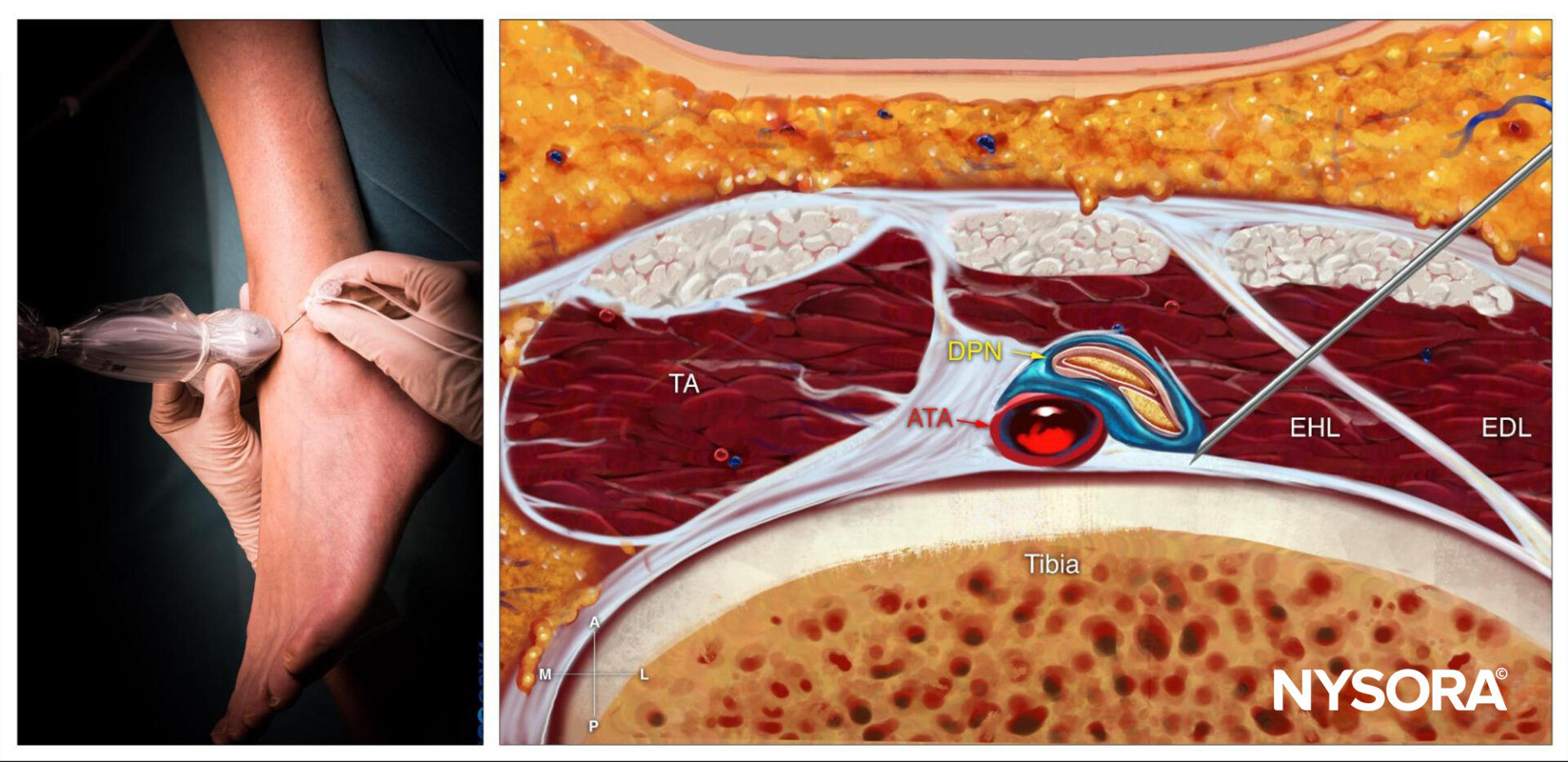
Reverse Ultrasound Anatomy for a deep peroneal nerve block at the ankle level with needle insertion in-plane and local anesthetic spread. TA, tibialis anterior muscle; ATA, anterior tibial artery; DPN, deep peroneal nerve; EHL, extensor hallucis longus; EDL, extensor digitorum longus.
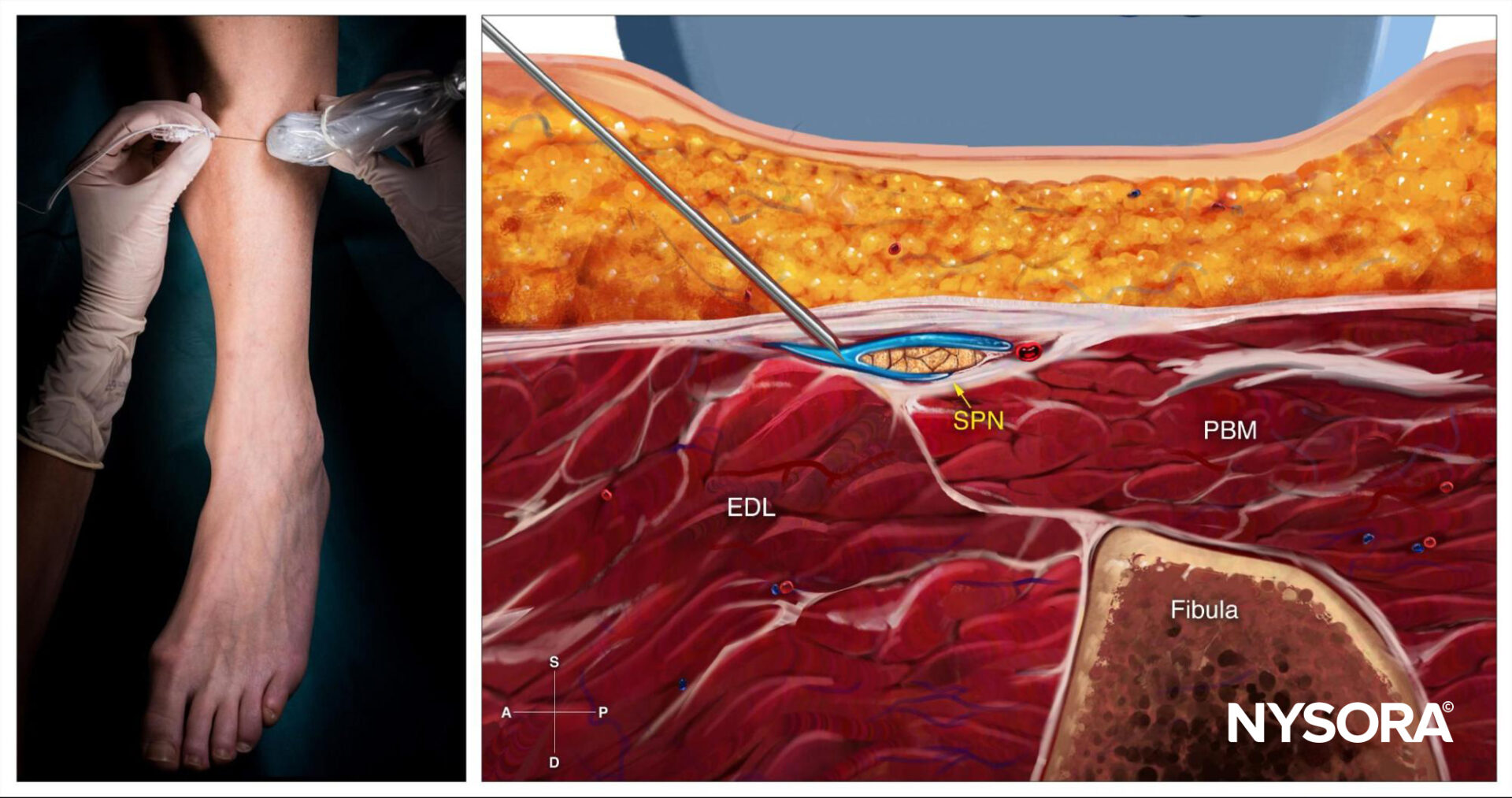
Reverse Ultrasound Anatomy for a superficial peroneal nerve block at the ankle level with needle insertion in-plane and local anesthetic spread. EDL, extensor digitorum longus; SPN, superficial peroneal nerve; PBM, peroneus brevis muscle.
Patient outcome
The ankle block was successfully administered without any immediate complications. The patient reported a complete loss of sensation in the targeted area and experienced effective pain relief for 24 hours post-surgery. This greatly minimized her need for opioid analgesics. A follow-up examination confirmed a satisfactory surgical outcome without any complications related to the nerve block.
This case highlights the effectiveness of ultrasound-guided nerve blocks in providing localized anesthesia and postoperative analgesia for hallux valgus surgery. Through precise targeting of relevant nerves, this approach can offer significant benefits, including reduced reliance on opioids, decreased postoperative pain, and potentially faster recovery.
For more case studies like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App in book format – the perfect study companion with the Nerve Blocks app!